










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.13 no.1 Pretoria Abr. 2019
http://dx.doi.org/10.7196/sajch.2019.v13i1.1532
ARTICLE
A study of self-reported handwashing practices of caregivers in relation to acute respiratory infections and gastroenteritis in infants in a peri-urban community in KwaZulu-Natal Province, South Africa
N M NseleI; N H McKerrowII
IMB ChB, FC Paed (SA); Department of Paediatrics and Child Health, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIMB ChB, DCH (SA), FC Paed (SA), MMed (Paed), PG Dip Int Res Ethics; KwaZulu-Natal Department of Health, Durban, South Africa
ABSTRACT
BACKGROUND: Handwashing is a recognised cost-effective intervention for the prevention of common childhood infections, including pneumonia and diarrhoeal disease. Globally, handwashing practices may be poor and little is known about handwashing practices in South Africa
OBJECTIVES: To describe and compare handwashing practises of caregivers whose infants are admitted with acute gastroenteritis and acute lower respiratory tract infection with those of healthy infants who are attending primary healthcare clinics for routine immunisation
METHODS: A cross-sectional study of self-reported handwashing practices was conducted among caregivers of infants from the Vulindlela area, Pietermaritzburg. Respondents were interviewed regarding household structure, services and handwashing practices
RESULTS: During the 3-month study period, 137 respondents were interviewed. Of these, 41 (30%) had infants with pneumonia, 41 (30%) with diarrhoea and 55 (40%) had healthy infants. A high rate of handwashing with soap and water (81.8%) was found in this study, with 58.4% of the respondents using running rather than stagnant water. Logistic regression identified some variables associated with higher odds of having a healthy infant, namely: a monthly household income >ZAR2 000 (odds ratio (OR) 4.74; 95% confidence interval (CI) 1.99 - 11.25); washing hands with soap and running water (OR 3.88; 95% CI 1.55 - 9.76); washing hands before eating (OR 7.41; 95% CI 0.79 - 68.76), and washing hands after household chores (OR 9.24; 95% CI 1.85 - 46.25
CONCLUSION: A higher than anticipated number of participants washed their hands with soap and running water and at critical moments
In 2016, the United Nations Children's Fund (UNICEF) estimated that 1.4 million children die from pneumonia and diarrhoea every year. These conditions account for 15% and 9% of under-5 deaths, respectively, with the majority occurring in low-resource settings.[1] According to the an earlier 'Saving Children' report,[2] 80% of early infant deaths in hospital can be attributed to acute gastroenteritis (AGE), acute respiratory infections (ARIs) and sepsis in the South African (SA) setting. Despite considerable progress in reducing child mortality, diarrhoeal disease and pneumonia still account for almost 20% of under-5 deaths.[3]
The World Health Organization (WHO) and UNICEF recommend breastfeeding, adequate nutrition, vaccination, access to a safe water source, basic sanitation and hand hygiene for the prevention of diarrhoea and pneumonia. When these fail, improved care-seeking behaviour is recommended, together with oral rehydration and vitamin A and zinc supplementation for the treatment of diarrhoeal disease and antibiotics for the treatment of pneumonia.[1,4]
The Centers for Disease Control and Prevention (CDC) has identified that critical moments for household handwashing include: before, during and after preparing food; before eating; after using the toilet; after changing a diaper or cleaning up a child who has used the toilet; after blowing one's nose or coughing; after touching animals or animal waste; and after touching garbage. The CDC recommends a five-step procedure for washing hands: wetting hands with clean running water and applying soap; rubbing the hands together, including the back of the hands, the web spaces and under the fingernails; scrubbing for 20 seconds; rinsing with running water; and drying with a clean towel.[5]
A meta-analysis by Aiello et al.[6]found that washing hands with soap was associated with a 40% and 17% reduction in the incidence of diarrhoeal disease and ARIs, respectively. Two-thirds of these studies were conducted in developed countries. Most were based in childcare centres and over half focused on children under 5 years of age.
Information about handwashing practices in SA communities is limited. According to the 2009 Global Hygiene Survey, 60% of South Africans do not wash their hands properly after using the toilet, sneezing or handling pets and food.[7] In assessing the cost and effect of scaling up interventions to save the lives of mothers and children in SA, Chola et al.[8] reported baseline coverage of 17% for soap-associated handwashing and identified handwashing to be the fifth most cost-effective intervention for reducing newborn and childhood deaths. Cole et al.[9] further demonstrated that in a periurban community in the Western Cape, SA, infectious illnesses were reduced by up to 75% in households that received hygiene products (antibacterial soaps, surface cleaners and antiseptic liquids) and subsequently practised basic good hygiene habits, including washing hands with soap. This reduction included an 80% and 70% reduction in the incidence of gastrointestinal and respiratory infections, respectively.
Little is known about handwashing practices in KwaZulu-Natal Province. This study was undertaken to describe household handwashing practices specifically of the primary caregiver and its impact on the incidence of infectious diseases in infants in Vulindlela, Pietermaritzburg.
Methods
This cross-sectional study was conducted in the Edendale Hospital and its draining primary healthcare clinics (PHCs), which represents a peri-urban setting outside Pietermaritzburg, from July to September 2016. Caregivers of infants admitted to the hospital with a primary diagnosis of either AGE or ARI and caregivers of healthy infants attending a PHC for routine immunisation were eligible for the study.
Although a convenience sample of 150 caregivers was planned, equally divided between the three criteria groups, the final sample consisted of only 137 caregivers owing to fewer patients admitted with diarrhoea or pneumonia than expected during the study period. Of the final sample, 41 caregivers were from the AGE and ARI groups each and 55 were from the group with healthy infants.
After giving informed consent, participants were interviewed by the principal researcher using a structured questionnaire. In an effort to minimise bias, the first section of the questionnaire (covering the participant's demographics) was interviewer administered, whereas the second section (on handwashing practices) was self-administered, with the assistance of the principal researcher as needed. In section 1, information regarding demographics of the caregiver, infant and household was obtained. Section 2 explored caregivers' handwashing practices in various circumstances, including: after using the toilet; when changing an infant's diaper; when handling pets and performing household chores; and before preparing or eating food or feeding their infant.
Data were captured in a spreadsheet and analysed using SPSS (IBM Corp., USA) to derive descriptive statistics and compare categorical variables by means of a chi-squared test. A significance level of p<0.05 was used. Ethical approval was obtained from the University of KwaZulu-Natal (ref. no. BREC BE013/16).
Results
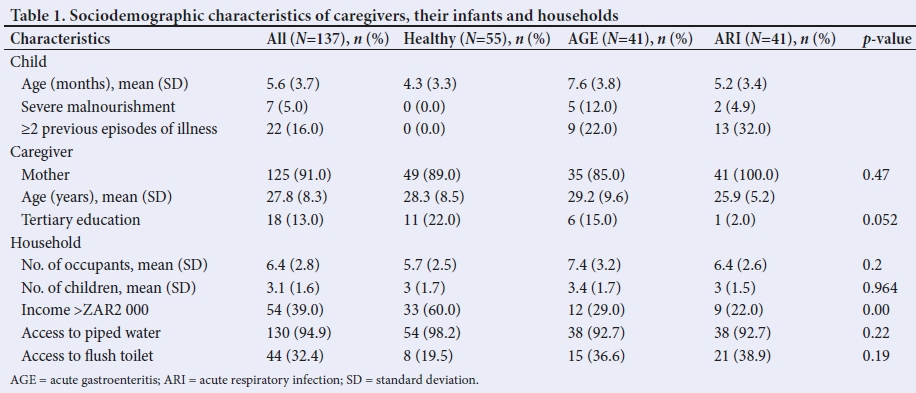
The mean age of the infants across the total sample was 5.6 months; the mean age was lowest in the healthy group (4.3 months) and highest in the AGE group (7.6 months) (Table 1). Only seven infants were severely malnourished, with five of them being in the AGE group. Previous episodes of illness with AGE or a lower respiratory tract infection were recorded for 16% (n=22) of the infants, with a larger proportion (n=13; 32%) seen in the ARI group. No previous episodes of illness were recorded in the healthy group.
The majority of caregivers (n=125; 91.0%) were the mothers of the infants, with the fewest mothers (n=35; 85%) seen in the AGE group and most (n=41; 100%) in the ARI group; however, this difference was not statistically significant (p=0.47). The mean age of the caregivers was 27.8 years, with the youngest (25.9 years) in the ARI group and the oldest (29.2 years) in the AGE group. Only 13% of the caregivers (n=18) had tertiary education, with the highest percentage (22%) in the healthy group. However, this was not statistically significant (p=0.052).
In addition to having the fewest occupants per household, the healthy group had the greatest proportion of households with a monthly income >ZAR 2 000 (p=0.00). Most households (n=130; 94.9%) had access to piped water but only a third, including 19.5% of the healthy group, reported having a flush toilet at home. This difference was not statistically significant (p=0.19).
All participants reported washing their hands, with 82% reporting using soap but only 58% using soap and running water (Table 2). The highest proportion of respondents who used soap and running water were in the healthy group (p=0.00). The majority of participants (67%) washed both hand surfaces, but only 22% (n=30) also paid attention to the web spaces. Most of these respondents (n=14) were from the ARI group. This number was higher than in either of the two other groups, although the difference was not statistically significant.
Responses regarding when participants washed their hands differed between the three groups, and complying with accepted norms was consistently lower in the AGE group. All participants in the healthy group washed their hands after using the toilet (p=0.04) and before preparing food (p=0.007), which compared significantly with practices in the other groups. A significantly greater proportion of caregivers from the healthy group also reported washing their hands after household chores (p=0.00) and before eating (p=0.02). A logistic regression model showed that using soap and running water and washing hands before eating and after household chores were associated with higher odds of the infant being healthy.
Discussion
In a peri-urban community of a developing country, where diarrhoeal disease and ARIs are the leading causes of death in children under 5 years, handwashing has a crucial role in reducing the incidence of such infectious diseases.[2]
Infants
The Expanded Programme on Immunisation in SA requires frequent visits to a healthcare facility during the first 14 weeks of life, which may explain why the lowest mean age was reported in the healthy group. Only 5% of infants were severely malnourished, with most (n=5) seen in the AGE group. Although the relationship between AGE and severe malnourishment has previously been described,[10] this relationship was not considered in the current study.
Caregivers
Most of the caregivers were the mothers of the infants, which is similar to findings from earlier studies in India and Nigeria.[11,12] However, the caregivers in our study were slightly younger than participants in the comparative earlier studies. Although fewer caregivers in our study had tertiary education than in the study by Odu et al.[12](13.0% v. 70.3%), it should be noted that education was not associated with better handwashing practices(p=0.052). In contrast, Luby et al.[13] found that having an education above primary level was associated with higher chances of washing both hands after contact with excreta. As both the current study and that of Odu et al.[12]were conducted in African communities, whereas that of Luby et al.[13]focused on an Asian community, it is possible that cultural attitudes towards handwashing are more important in determining handwashing practices than education.
Households
The only household characteristic found to have a significant effect on handwashing practices was a monthly income >ZAR2 000 (USD 160). This is similar to the findings by Luby et al.,[13]who showed that in Bangladesh handwashing behaviour was not influenced by access to piped water or improved sanitation in the household; handwashing was more likely to occur in households in the top 40% of the population with regard to income.
Burton et al.[14]concluded that using soap and water was superior to using water alone in removing bacteria of faecal origin from the hands. Despite more than 60% of the participants reporting a monthly household income <ZAR2 000 and an average of 6.4 occupants, the occurrence of washing hands with soap was high (81.8%). However, only 58% of the participants in the study reported using soap and running water when washing their hands, although this trend was not uniform across all three groups. As 60% of households in the healthy child group had a monthly household income >ZAR2 000 compared to 29% of AGE households, availability of income may explain the increased use of soap in the healthy child group. This finding supports earlier findings that showed that the availability of soap in households increases according to the level of income.[15] It is also possible that people perceive soap to be important for household hygiene and therefore prioritise soap even within a limited household budget.
In a meta-analysis by Freeman et al.,[16]the global mean prevalence of handwashing after contact with excreta was estimated to be 19%.
Little variation was seen between regions of the same income, ranging from 5% to 25% in the developing world and 48% to 72% in the developed world. However, it should be noted that only studies that employed direct observation of handwashing behaviour were included in that meta-analysis, as self-reporting has been known to overestimate real handwashing rates.
Handwashing practices
Although all of the participants reported using water, either running or stagnant, for washing their hands and 94.9% of households had piped water on site, only 70.8% used running water when washing their hands. This may be due to the household having only one tap on the property and therefore not at the place of handwashing after critical moments. An earlier study has shown that improved water availability is associated with an increase in the frequency of handwashing and also the amount of water used for hygiene purposes.[17] In our study, 58.4% of participants reported using soap and running water when washing their hands, which is higher than the 17% reported by Chola et al.[8] but similar to the global figure of 55% identified in the 2009 Global Hygiene Survey. However, it should be noted that this survey included predominantly developed countries such as Australia, the UK, Germany and the USA.[7]
The CDC-recommended procedure for handwashing includes washing between the fingers. Only 21.9% of participants in our study reported doing this. There is limited evidence as to how the procedure employed in handwashing, with regard to either duration of handwashing or technique, can maximise the efficacy of the handwashing practice.[18] This may therefore be an important area for future public health intervention. Although our study did not establish the duration of handwashing, Khan et al.[11]found that despite the WHO recommendation for caregivers to wash the palms and back of the hands for more than 20 seconds, this practice did not influence the number of cases of diarrhoeal disease or ARI in infants.
The majority of participants (81.8%) reported washing their hands at critical points, especially after using the toilet, before eating and before feeding their infant. Handwashing after handling pets, however, was limited. This high rate of handwashing at critical points is in contrast to the 40% reported for SA by the 2009 Global Hygiene Survey,[7] which noted that the country had poor handwashing practices compared with many developed countries. However, the rate is similar to that reported in studies from India[11] (82.6%) and Nigeria[12] (75.5%) and considerably higher than the 18% reported in a study in Bangladesh.[13] The high rate may be due to self-reporting used in this study, as participants may have provided the answers they perceived to be 'right. Close-ended questions as used in this study may also have invoked a positive response from the participants.
Conclusion
Most of the participants washed their hands with soap and water and after critical moments. The rates are higher than those reported in other studies, but may be a result of self-reporting. Caregivers with a monthly household income >ZAR2 000 were more likely to wash their hands; however, the level of education of the caregivers did not appear to influence handwashing practices. Handwashing was more common among caregivers of healthy infants. This group was also noted to have more participants with a monthly income >ZAR2 000 and fewer household occupants.
Proper handwashing can contribute to reducing infectious diseases among children. However, studies on handwashing practices in the SA community setting are limited. Although our study yielded exploratory results in a peri-urban community, observational studies rather than self-reporting and across a larger sample may provide a more robust assessment of handwashing practices in this setting.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the degree of Master of Medicine.
Acknowledgements. The authors would like to express their gratitude to the participants in this study and the staff of the Edendale Hospital's paediatric wards who were involved in the infants' care. Ms Busisiwe Msweli is acknowledged for assistance with data collection.
Author contributions. NMN and NHM designed and developed the study. NMN collected the data, performed the analysis and prepared the manuscript. NHM supervised the study and reviewed and edited the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. United Nations Children's Fund. One is too many: Ending child deaths from pneumonia and diarrhea. New York: UNICEF, 2016. [ Links ]
2. Stephen CR, Bamford LJ, Patrick ME, Wittenburg DF. Saving Children 2009: Five years of data: A sixth survey of child healthcare in South Africa. Pretoria: MRC, 2011. [ Links ]
3. Statistics South Africa. Mortality and causes of death in South Africa, 2015: Findings from death notification. Pretoria: StatsSA, 2017. [ Links ]
4. World Health Organization. World Health Report 2005: Make every mother and child count. Geneva: WHO, 2005. [ Links ]
5. Centers for Disease Control and Prevention. Handwashing: Clean hands saves lives. https://www.cdc.gov/handwashing/when-how-handwashing.html (accessed 15 April 2016). [ Links ]
6. Aiello AE, Coulborn RM, Perez V, Larson EL. Effect of hand hygiene on infectious disease risk in the community setting: A meta-analysis. Am J Public Health 2008;98(8):1372-1381. https://doi.org/10.2105/ajph.2007.124610 [ Links ]
7. Global Hygiene Council. Setting the hand hygiene standards: Global Health Survey. London: Global Hygiene Council, 2009. [ Links ]
8. Chola L, Pillay Y, Barron P, Tugendhaft A, Kerber K, Hofman K. Cost and impact of scaling up interventions to save lives of mothers and children: Taking South Africa closer to MDGs 4 and 5. Glob Health Action 2015;8:27265. https://doi.org/10.3402/gha.v8.27265 [ Links ]
9. Cole EC, Hawkley M, Crookstan BT, et al. Comprehensive family hygiene promotion in peri-urban Cape Town: Gastrointestinal and respiratory illness and skin infection reduction in children aged under 5. S Afr J Child Health 2012;6(4):109-117. https://doi.org/10.7196/sajch.459 [ Links ]
10. Talbert A, Thuo N, Karisa J, et al. Diarrhoea complicating severe acute malnutrition in Kenyan children: A prospective descriptive study of risk factors and outcome. PLoS One 2012;7(6):e38321. https://doi.org/10.1371/journal.pone.0038321 [ Links ]
11. Khan S, Kumar V, Priya N, Yadar SS. Handwashing practices among the caregivers of under 5 children in rural and urban areas of Morabadad, India: A community based study. Int J Med Sci Public Health 2016;6(1):1-6. https://doi.org/10.5455/ijmsph.2017.10072016573 [ Links ]
12. Odu OO, Emmanuel EE, Amu EO, Deji S, Dada SA, Marais O. Practice of effective hand washing and associated factors among caregivers of infants attending infant welfare clinics in Ado-Ekiti, Ekiti State, Nigeria. Br J Med Med Res 2017;19(11):1-8. https://doi.org/10.9734/bjmmr/2017/31836 [ Links ]
13. Luby SP, Halder AK, Tronchet C, Akhter S, Bhuiya A, Johnston RB. Household characteristics associated with handwashing with soap in rural Bangladesh. Am J Trop Med Hyg 2009;81(5):882-887. https://doi.org/10.4269/ajtmh.2009.09-0031 [ Links ]
14. Burton M, Cobb E, Donachie P, Judah G, Curtis V, Schmidt W. The effect of handwashing with water or soap on bacterial contamination of hands. Int J Environ Res Public Health 2011;8(1):97-104. https://doi.org/10.3390/ijerph8010097 [ Links ]
15. Luby SP, Halder AK. Associations among handwashing indicators, wealth and symptoms of childhood respiratory illness in urban Bangladesh. Trop Med Int Health 2008;13(6):835-844. https://doi.org/10.1111/j.1365-3156.2008.02074.x [ Links ]
16. Freeman MC, Stocks ME, Cumming O, et al. Hygiene and health: Systematic review of handwashing practices worldwide and update of health effects. Trop Med Int Health 2014;19(8):906-916. https://doi.org/10.1111/tmi.12339 [ Links ]
17. Biran A, Schmidt W, Wright R, et al. The effect of soap promotion and hygiene education campaign on handwashing behaviour in rural India: A cluster randomised trial. Trop Med Int Health 2009;14(10):1303-1314. https://doi.org/10.1111/j.1365-3156.2009.02373.x [ Links ]
18. Bloomfield SF, Aiello AE, Cookson B, O'Boyle C, Larson EL. The effectiveness of hand hygiene procedures in reducing the risks of infections in home and community settings including handwashing and alcohol-based hand sanitizers. Am J Infect Control 2007;35(10 Suppl 1):S27-S64. doi:10.1016/j.ajic.2007.07.001 [ Links ]
Accepted 23 August 2018


{kind=link}
{kind=link}