










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.12 no.4 Pretoria Dez. 2018
http://dx.doi.org/10.7196/sajch.2018.v12i4.1485
ARTICLE
Family environment, socioeconomic conditions and childhood health and wellbeing in informal settlements in Mozambique
B M Cau
PhD; Department of Geography, Faculty of Arts and Social Sciences, Eduardo Mondlane University, and Centre for Research on Population and Health, Maputo, Mozambique
ABSTRACT
BACKGROUND. A possible relationship between slum residence and children's health and wellbeing in sub-Saharan Africa has been relatively under-researched.
OBJECTIVE. To investigate the relationship between the type of area of residence and children's and adolescents' health and wellbeing in urban Mozambique.
METHODS. Descriptive and logistic regression techniques were employed on data from 1 913 children and 798 adolescents, to analyse several key outcomes.
RESULTS. The descriptive findings indicate that children in slum areas are the most disadvantaged, followed by those in quasi-slum areas, in terms of school enrolment, health and the type of care received in the home. Similar descriptive results were found for the adolescents' outcomes. Multivariate analyses showed that compared with children in slum areas, those in non-slum areas were more likely to be attending school (odds ratio (OR) 4.22; confidence interval (CI) 1.73 - 10.31), less likely to be typically sick (OR 0.26; CI 0.14 - 0.47) and less likely to be left alone in the household (OR 0.29; CI 0.18 - 0.48). Adolescents in non-slum areas tended to have completed >6 years of education (OR 3.01; CI 1.78 - 5.07), to be aware of HIV/AIDS programmes (OR 4.29; CI 2.43 - 7.55), to believe that HIV/AIDS may be transmitted through unprotected sex (OR 13.01; CI 3.76 - 45.02) and to have parents or caregivers who had ever talked to them about matters related to sex (OR 3.15; CI 1.76 - 5.65). Family structure and sowcioeconomic characteristics, together, account for most of the differences between slum and quasi-slum areas, particularly for children's outcomes.
CONCLUSION. The health and the wellbeing of children and adolescents in slums is negatively affected, compared with other urban places in Mozambique. However, for children, family structure and other socioeconomic factors remove most slum/quasi-slum effects.
The United Nations estimates that approximately 40% of the population of sub-Saharan Africa lives in urban areas.[1] However most of these urban residents live in slums.[2] Previous literature on sub-Saharan Africa has described slum residence in the region in terms of various negative health outcomes.[3-5] Yet one key concern less researched in sub-Saharan Africa is the possible relationship between slum residence and children's and adolescents' health and wellbeing. The few existing studies investigating links between slum residence and children's health and wellbeing, mostly based in Nairobi, in Kenya, have reported a higher risk of illness and mortality[6] and lower school enrolment[7] among children in slums, compared with those in more formal, non-slum urban areas. Given the high prevalence of slums in urban areas of sub-Saharan Africa,[2] there is a need for further studies on connections between slum residence and children's and adolescents' health and wellbeing in the region. Furthermore, considering that slums in sub-Saharan Africa are typically labelled as places of poverty with harsh living conditions,[2,3] there is a need to also investigate the possible role that household conditions and living environment plays regarding the health and wellbeing of children and adolescents living in slums. Indeed, recently, scholars have expressed the need for more research on health in slums in low-income countries.[8,9]
One key household characteristic that is likely to amplify or moderate any negative effects of slum residence on children's and adolescents' health and wellbeing in sub-Saharan Africa is family structure. Children of single mothers tend to experience negative health outcomes compared with those of mothers in union ties in the region.[10] The wellbeing of single mothers' children and
adolescents in urban slum areas is also likely to be negatively affected by their mothers' lack of resources and time for providing them with enough care and attention.[11] Children's and adolescents' education - a proxy for their future wellbeing - is also likely to be affected by slum residence and the household family structure. Although in some circumstances, children and adolescents in female-headed households may have positive school outcomes,[12] single mothers' children are likely to lack sufficient parental support and guidance to enrol and succeed in school.[13] Adolescents from female-headed households in slum areas of sub-Saharan Africa are also likely to lack adequate sexual knowledge and education,[3] a fact that may expose them to HIV infection and other threats to their current and future wellbeing.
There is also a possibility that other household socioeconomic characteristics, such as the age of the household head, household composition and household wealth/financial status, as well as the type of care that children and adolescents receive in the household, may modify the effects of slum residence on children's and adolescents' health and wellbeing. In this study, we investigate the relationship between slum residence, family and household environment and children's and adolescent's health and wellbeing in Mozambique. In particular, we attempt to answer the following research questions: (i) What are the differences in health and wellbeing between children's and adolescents' residing in slum, quasi-slum and non-slum urban areas in Mozambique? (ii) What is the role of the household family structure and other household socioeconomic characteristics in modifying the relationship between slum residence and children's and adolescents' health and wellbeing
in urban areas of Mozambique? As a southern African country in which -56% of its population are aged <20 (with 23% aged 10 - 19 years),[14] non-marital fertility estimated at three children per woman[15] and -80% of its urban residents living in informal settlements,[2] Mozambique is an interesting setting in which to assess the health and wellbeing of children and adolescents in slum areas.
Methods
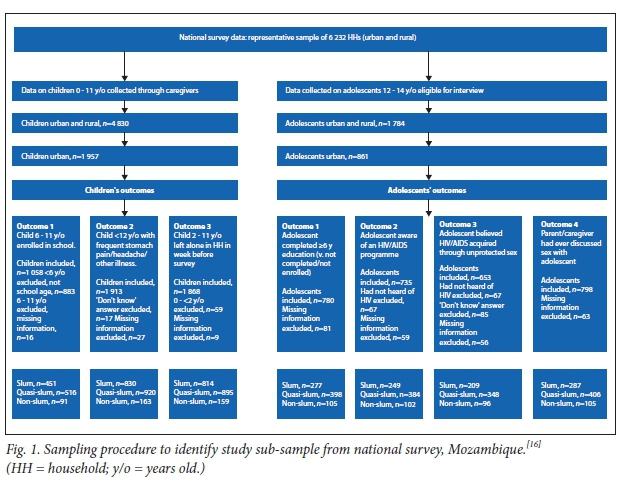
The data for this study are from a nationally representative survey on the 'prevalence, behavioural risks and information about HIV/AIDS' in Mozambique, conducted in 2009.[16] From a representative sample of 6 232 households, a total of 1 900 female and male adolescents aged 12 - 14 years were interviewed (930 in urban areas).[16] The survey also collected information about 4 830 children aged 0-11 years (1 957 in urban areas) from their caregivers. The present study uses data from a total of 1 913 children and 798 adolescents residing in urban areas, for whom the relevant information was available (the analytic sample size varies according to the outcome andthe completeness of relevant information on the predictors of interest).
The study assessed several key measures of health and wellbeing, as outcomes, relevant for the current context of most countries in sub-Saharan Africa, for children and adolescents. The outcome variables for children are the following: (i) whether or not a child aged 6-11 years is enrolled in school; (ii) whether or not there is a child in the household <12 years old who frequently suffers from pain in the stomach, headaches or other illness; and (in) whether or not a child aged 2-11 years was often or sometimes left alone in the household during the week before the survey date. Children's care and education are critical factors for their current and future wellbeing.
For adolescents, the outcomes of interest are the following: (i) whether an adolescent has completed > 6 years of education (as opposed to non-completed or not enrolled in school); (ii) whether or not an adolescent is aware of an HIV/AIDS programme; (Hi) whether or not an adolescent believes that HIV/AIDS may be acquired through unprotected sex; and (iv) whether or not an adolescent's father/ mother or a caregiver has ever talked to him/ her about matters related to sex. In the context of southern Africa, a region heavily affected by HIV/AIDS, adolescents' knowledge and beliefs about it are crucial for their health and wellbeing. Adolescents' education is also a key determinant of their health and wellbeing in adulthood. Owing to limitations in the dataset, for adolescents' wellbeing alone, the study only considers education as a proxy measure of future wellbeing. Fig. 1 provides a detailed description of the study outcome variables and the sampling procedure, from the national survey to the sub-sample considered in each outcome of interest.
The primary predictor was the type of place of residence within an urban area (slum, quasi-slum or non-slum). In addition to major cities such as Maputo, Matola and Beira, there are informal settlements in other urban areas throughout Mozambique.[2] Following an approach introduced by Zulu et al. (2002),[3] we considered a household as being in a slum area if it simultaneously lacked piped water, electricity and a flush toilet. A household was seen as being in a non-slum area if it concurrently possessed piped water, electricity and a flush toilet. Households with at least one or two of the items were considered as located in a quasi-slum area.
Another key predictor of interest was family structure, which considers two variables: the sex of the household head; and the marital status of the household head. Marital status was classified into one of three categories: married (the reference); widow(er); and other (never married, divorced or separated). Other variables considered in the study measure further household socioeconomic characteristics that are likely to modify the relationship between slum residence and children's and adolescents' health and wellbeing. These were the age of the household head (with six categories: 15-24 (the reference), 25 - 34, 35 - 44, 45 - 54, 55 - 64 and >65); the person who cared for a child or an adolescent most of the time (four categories: father or mother, including step-father/mother (the reference), brother or sister, other family member, and other non-family adult); the number of household members (<4 (the reference), 4 -5, 6 - 7, and >8); and the household wealth position, according to an adaptation of the national survey's wealth categorisation index (low (the reference), middle and high). The survey's wealth index variable consisted of five categories (poorest, poorer, middle, richer and richest). For the purposes of this study, the first two categories (poorest and poorer) were collapsed into low', and richer and richest combined to form 'high. The study also considered the sex of the child or adolescent as a control variable, to account for possible variation in the outcomes of interest, particularly for school education.
Our analytical process had two main steps. First, the pattern of variation of the outcomes and predictors of interest by the type of urban residential area was assessed. Second, for each outcome, we ran three models. The first considered only the type of urban residential area as the predictor. The second added family structure variables. The final model added the rest of the predictors. In the results section, we only present findings from the last model (results from the other models are included in appendix A at http:// sajch.org.za/public/files/SAJCH1485_ Supplementary_Tables_May2018.docx.
Results
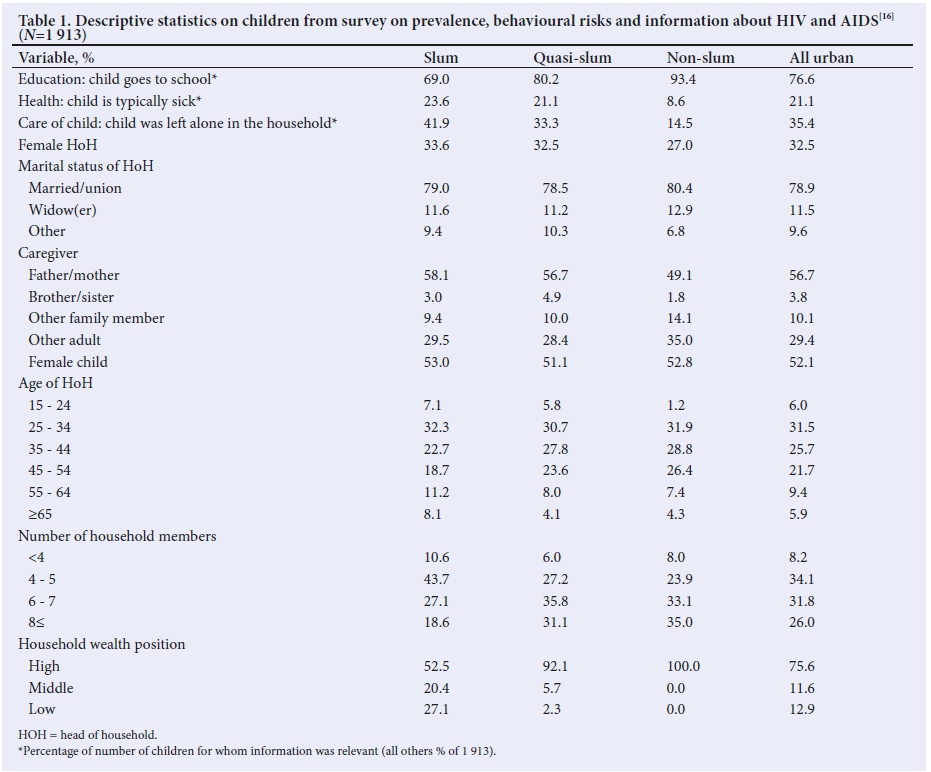
Table 1 presents selected descriptive statistics on the children. A gradient pattern emerges, where those in slum areas are the most disadvantaged, followed by those in quasi-slum areas, for school enrolment, health and children's care. Regarding education, for example, 93.4% of the children aged 6-11 years in non-slum areas were enrolled in school, against 80.2% in quasi-slum areas and only 69.0% in slum areas. Various differences by type of urban residential area were also observed concerning family structure and other household socioeconomic characteristics. For instance, those in non-slum areas were most likely to be married, while the percentages of those married or in union ties in slum and quasi-slum areas are both similar, at -79%. However, those in slum areas were the least likely to be in the high household wealth position, compared with those in quasi-slum and non-slum areas.
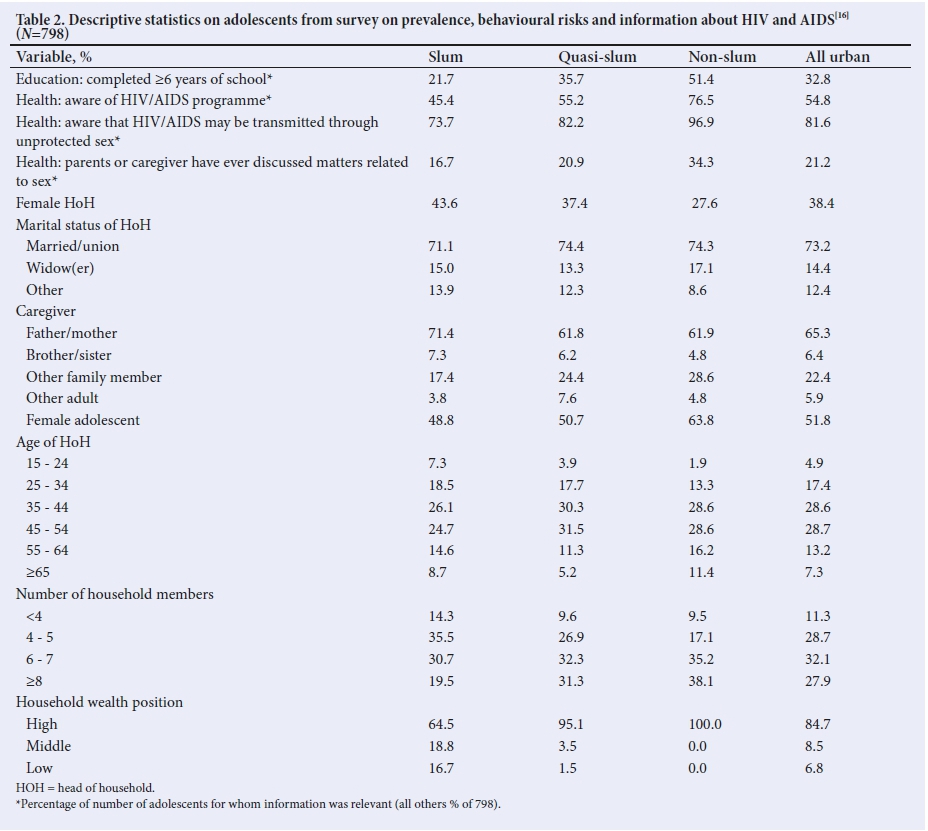
Table 2 shows the descriptive statistics for adolescents. As with the children in Table 1, adolescents in slum areas displayed poor outcomes in comparison with those in quasi-slum and non-slum urban areas. While only 45.4% of adolescents in slum areas were aware of an HIV/AIDS programme, the corresponding figure was 55.2% in quasi-slum areas, and nearly 77% in non-slum urban areas. A similar pattern was observed with respect to adolescents' beliefs regarding whether or not HIV/AIDS could be transmitted through unprotected sexual intercourse, whether or not adolescents' parents or caregivers had ever talked to them about sexual matters, and whether or not adolescents had completed >6 years of education.
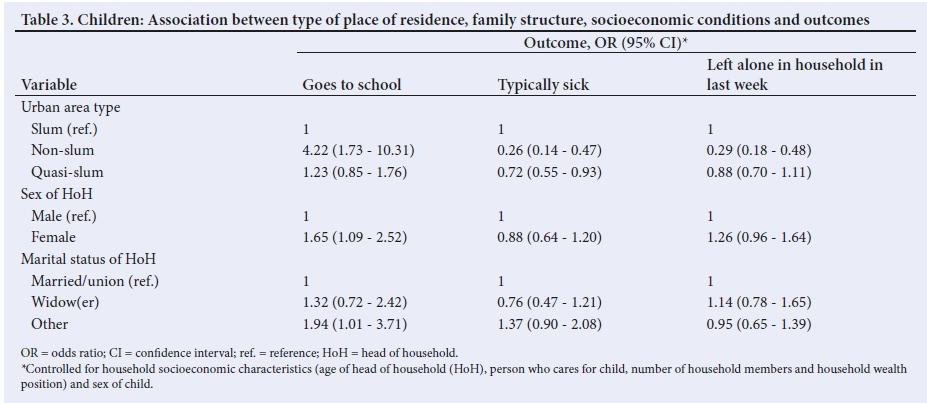
Multivariate associations for children's outcomes are shown in Table 3. The table only displays results pertaining to the type of urban residential area and family structure predictors. For the probability of a child being in school, it was found that those living in non-slum areas were substantially more likely to be attending school, compared with children residing in slum areas, when controlling for other factors. Children from female-headed households and those from households with heads of 'other' marital status were significantly more likely to be attending school than their peers. Regarding child health, the findings in Table 3 show that children residing in non-slum and quasi-slum areas were significantly less likely to be typically sick than those from slum areas. For the probability that a child had been left alone in the household during the past week, it was found that those in non-slum areas were significantly less likely to have been.
Table 4 presents multivariate results for adolescents. It was found that slum residence was significantly associated with adolescents' education, health knowledge and beliefs. For instance, compared with adolescents in slums, those in non-slum and quasi-slum areas were significantly more likely to have completed >6 years of education, adjusting for other factors. Adolescents in non-slum areas and quasi-slum areas were also significantly more likely to be aware of HIV/AIDS programmes. Those residing in non-slum and quasi-slum areas were substantially more likely to believe that HIV/AIDS can be transmitted through unprotected sex, relative to the reference group. Adolescents in the non-slum areas also exhibited an advantage in the likelihood of their parents or caregivers having talked to them about matters related to sex. Interestingly, as pertains to household family structure, adolescents in widow-headed households were significantly more likely to believe that HIV/AIDS can be transmitted through unprotected sexual intercourse than the reference group.
Discussion
Consistent with previous studies,[6,7] the findings in this paper show a strong link between slum residence and negative outcomes for children and adolescents. Children living in slum areas exhibit a disadvantage, particularly relative to those in non-slum urban areas. Specifically, it was found that relative to children in non-slum areas, those in slum areas were less likely to be attending school, more likely to be typically sick and more likely to be left alone in the household. Similarly, adolescents living in slum areas were substantially disadvantaged in educational and health outcomes, compared with those in quasi-slum and non-slum areas. In particular, adolescents in quasi-slum and non-slum areas tended to be more likely to have completed >6 years of education, and to have been exposed to or to possess information and knowledge concerning sexual matters, including HIV/AIDS.
Given the increasing rate of urbanisation in sub-Saharan Africa and the overwhelming presence of slums, with over 74% of their urban populations in countries such as the Democratic Republic of Congo, Madagascar and Mozambique living in informal settlements,[2] these findings are alarming with respect to the current and future wellbeing of children and adolescents in the region. Without education, children and adolescents in slums have their opportunities to enjoy adulthood free of serious material deprivations, social and health disadvantages compromised. Adolescents' lack of exposure to or possession of information and knowledge pertaining to sexual matters and HIV/AIDS is likely to jeopardise their health and wellbeing as well, particularly in southern Africa, the region with the highest prevalence of HIV/AIDS in the world.[17] This concern is justified, as previous studies have indicated that slum residents are more likely to engage in earlier sexual activity, and to have multiple sexual partners, compared with other urban dwellers.[3]
An important aspect to understand with respect to the relationship between slum residence, health and wellbeing is the processes through which such areas risk children's and adolescents' health and wellbeing. Given the diversity of slum areas,[2] this issue is important, as it may suggest which specific factors need to be addressed to improve lives in this particular context. Therefore,
in this study we also tried to assess the role of the household family structure and socioeconomic characteristics in modifying links between slum residence and children's and adolescents' health and wellbeing. Although the descriptive analysis displayed disadvantages for children in slums compared with those in non-slum and quasi-slum areas for a number of family structure and socioeconomic characteristics, multivariate analyses revealed an interesting picture. For the probability that a child was in school, for example, the findings indicated that children living in female-headed households and those from households whose family head had never been married, divorced or separated were more likely to be attending school. This is in line with Lloyd and Blanc's[12] argument that female household heads may be more inclined to invest in the educational success of the children in their households. For adolescents, those living in widow-headed households were more than three times as likely to believe that HIV/ AIDS may be transmitted through unprotected sexual intercourse compared with peers in married or union-headed households. Given the high prevalence of HIV/AIDS in southern Africa, and the possibility that some widowhood may have been caused by AIDS, adolescents in widow-headed households may be more aware of the link between sexual intercourse and HIV infection.
Overall, the findings in this study appear to suggest that family structure and socioeconomic characteristics together override most of the differences between slum and quasi-slum areas in health and wellbeing, particularly for children. With the addition of family structure and socioeconomic characteristics, most differences between slum and quasi-slum areas for children disappeared. Children from quasi-slum areas were only significantly different from those in slum areas with respect to the probability of being typically sick. Regarding this finding, it might be that children's sickness is especially sensitive to the few advantages that quasi-slum areas hold relative to slum ones. The lack of significant advantage for children in quasi-slum areas as compared with those in slum areas for the other outcomes suggests that efforts to tackle adverse conditions for children's health and wellbeing in urban areas should target both slum and quasi-slum areas. Interestingly, for adolescents' health and wellbeing, with the exception of parent-adolescent conversations about matters related to sex, it appears that the few socioeconomic advantages of adolescents in quasi-slum areas make a significant difference in comparison to their peers in slum areas. There are some limitations to this study. Notwithstanding the research interest in assessing relationships between slum residence and children's and adolescents' health and wellbeing, the outcome variables used may not adequately measure health and wellbeing. For instance, getting information about children's health and wellbeing from their caregivers may have shortcomings. However, despite these data limitations, the research questions that this article has attempted to address are relevant and important for subsanaran Africa and other low-income regions, and future studies could try to find answers to them using data with better measures. Furthermore, the analysis presented contributes to the literature by showing how family structure and socioeconomic characteristics may play out in differentiating children's and adolescents' health and wellbeing, particularly between residents of slum and quasi-slum urban areas.
Conclusion
This study has shown that in Mozambique, non-slum and slum areas are significantly different in terms of child health and wellbeing outcomes, independently of family structure and socioeconomic characteristics. Family structure and socioeconomic characteristics appear to matter the most for variations in child health and wellbeing between slum and quasi-slum areas. For adolescents' health and wellbeing, slum areas are mostly disadvantaged relative to quasi-slum and non-slum urban areas, regardless of family structure and socioeconomic characteristics. These findings suggest that programmes to improve child health and wellbeing in Mozambique and other countries with similar characteristics should target both slum and quasi-slum areas. For promoting adolescent health and wellbeing, however, priority should be given to slum areas.
Acknowledgements. The author is thankful for the instructive comments and suggestions from anonymous reviewers and the editor.
Author contributions. Sole author.
Funding. None.
Conflicts of interest. None
References
1. United Nations. World Urbanization Prospects: The 2014 Revision, Highlights. New York: UN, 2014. [ Links ]
2. UN-Habitat. Slum Almanac 2015/2016: Tracking Improvement in the Lives of Slum Dwellers. Nairobi: PSUP Team Nairobi, 2016. https://unhabitat.org/wp-content/uploads/2016/02-old/Slum%20Almanac%202015-2016_EN.pdf (accessed 8 February 2018). [ Links ]
3. Zulu EM, Dodoo FN, Ezeh, CA. Sexual risk-taking in the slums of Nairobi, Kenya, 1993 - 98. Popul Stud 2002;56(3):311-323. https://doi.org/10.1080/00324720215933 [ Links ]
4. Lungu EA, Biesma R, Chirwa M, Darker C. Healthcare-seeking practices and barriers to accessing under-five child health services in urban slums in Malawi: A qualitative study. BMC Health Services Res 2016;16:410. https://doi.org/10.1186/sl2913-016-1678-x [ Links ]
5. Penrose K, de Castro MC, Werema J, Ryan ET. Informal urban settlements and cholera risk in Dar es Salaam, Tanzania. PLoS Negl Trop Dis 2010;4(3):e631. https://doi.Org/10.1371/j ournal.pntd.0000631 [ Links ]
6. Kyobutungi C, Ziraba AK, Ezeh A, Yé Y. The burden of disease profile of residents of Nairobi's slums: Results from a demographic surveillance system. Popul Health Metrics 2008;6:1. https://doi.org/10.1186/1478-7954-6-l [ Links ]
7. Mugisha F. School enrolment among urban non-slum, slum and rural children in Kenya: is the urban advantage eroding? Int J Educ Dev 2006;26(5):471-482. https://doi.Org/10.1016/j.ijedudev.2005.09.012 [ Links ]
8. Ezeh A, Oyebode O, Satterthwaite D, et al. The history, geography, and sociology of slums and the health problems of people who live in slums. Lancet 2017:389(10068):547-558. https://doi.org/10.1016/S0140-6736(16)31650-6 [ Links ]
9. Lilford R, Oyebode O, Satterthwaite D, et al. Improving the health and welfare of people who live in slums. Lancet 2017;389(10068):559-570. http://doi.org/10.1016/S0140-6736(16)31848-7 [ Links ]
10. Ntoimo LFC, Odimegwu CO. Health effects of single motherhood on children in sub-Saharan Africa: A cross-sectional study. BMC Publ Health 2014;14:1145. http://www.biomedcentral.com/1471-2458/14/1145 (accessed 19 September 2017). [ Links ]
11. Gurmu E, Elana D. Household structure and children's nutritional status in Ethiopia. Genus 2013;69(2):113-130. [ Links ]
12. Lloyd CB, Blanc AK. Children's schooling in sub-Saharan Africa: The role of fathers, mothers, and others. Popul Dev Rev 1996;22(2):265-298. https://doi.org/10.2307/2137435 [ Links ]
13. Astone NM, McLanahan SS. Family structure, parental practices and high school completion. Am Sociol Rev 1991;56(3):309-320. https://doi.org/10.2307/2096106 [ Links ]
14. Instituto Nacional de Estatística, Mozambique. III Recenseamento Geral da População e Habitação 2007: Resultados Definitivos - Moçambique. Maputo: Instituto Nacional de Estatística, 2010. [ Links ]
15. Arnaldo C. Dinâmica de fecundidade em Moçambique. Centro de Pesquisa em População e Saude, Gazeta Demográfica No. 1, 2013. [ Links ]
16. Instituto Nacional de Saude, Instituto Nacional de Estatística, ICF Macro. Mozambique: National Survey on Prevalence, Behavioural risks and Information about HIV and AIDS (2009 INSIDA), 2010. Calverton, Maryland, EUA: INS, INE and ICF Macro, 2010. [ Links ]
17. Joint United Nations Programme on HIV/AIDS. Global Aids Update 2016. Geneva: UNAIDS, 2016. http://www.unaids.org/sites/default/files/media_asset/global-AIDS-update-2016_en.pdf (accessed 3 March 2018). [ Links ]
 Correspondence:
Correspondence:
B M Cau
boaventura.cau@uem.ac.mz
Accepted 9 May 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}