










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.12 spe Pretoria 2018
http://dx.doi.org/10.7196/sajch.2018.v12i2.1526
ARTICLE
Sexual harassment in South African Schools: Is there an association with risky sexual behaviours?
K MabethaI; N de WetII
IMA; Demography and Population Studies, Faculties of Health Sciences and Social Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; Demography and Population Studies, Faculties of Health Sciences and Social Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Several drivers of risky sexual behaviour are known, although research has not yet examined the relationship between experiences of sexual harassment at school and risky sexual behaviours among adolescents.
OBJECTIVE. To examine the association between peer- and teacher-perpetrated sexual harassment and risky sexual behaviours among adolescents in South Africa.
METHODS. Cross-tabulations and logistic regression models were fitted to data from 219 456 school-going adolescents (aged 10 - 19 years) who participated in the fourth South African National HIV, Behaviour and Health Survey (2011/2012). The outcomes were lack of condom use during last sexual activity and multiple sexual partnerships.
RESULTS. Of the respondents who had experienced sexual harassment by peers, 27.27% did not use a condom during their last sexual activity and 41.67% reported having had multiple sexual partnerships. Of the respondents who had experienced sexual harassment by a teacher, 5.56% reported to have had multiple sexual partnerships in the study period. Results show that respondents who had experienced peer-perpetrated sexual harassment were more likely to not have used a condom during their last sexual activity (odds ratio (OR) 1.08; 95% confidence interval (CI) 1.04 - 1.11), as were those who had experienced teacher-perpetrated sexual harassment (OR 1.37; 95% CI 1.32 - 1.43).
CONCLUSION. A substantial number of school-going adolescents were found to have experienced sexual harassment and engaged in risky sexual behaviours. Sexual harassment at school should be considered as part of programmes aimed at addressing risky sexual behaviours among adolescents.
Risky sexual behaviours pose a continued risk to the health and development of adolescents. In recent decades, there has been a substantial increase in the number of school-going adolescents who engage in risky sexual behaviours, including having multiple sexual partners.[11] Studies in South Africa (SA) have shown that 50% of adolescents engage in sexual intercourse before the age of 16, with as many as 60% of these adolescents reporting not using condoms. [2,3] Furthermore, an earlier study among SA youth showed that up to 30% of adolescents with an early age of sexual debut are not in monogamous relationships.[2]
Lack of condom use and having multiple sexual partners are commonly reported to increase the risk of exposure to long-term negative health outcomes such as unplanned pregnancies and sexually transmitted infections, including HIV.[4,5] Considerable efforts have been made by the SA government to eliminate risky sexual behaviours among adolescents, including providing free condoms, providing information on HIV/AIDS and driving mass media campaigns.[6] However, despite these efforts, multiple sexual partnerships and the lack of condom use persist.[6]
Adolescents spend a large proportion of their time in school and although the primary purpose of schools is to foster academic development, the school environment also has broader effects on physical and mental health outcomes of adolescents.[71 Bullying, the lack of physical activities incorporated into the curriculum and poor or absent feeding schemes contribute to negative health outcomes of children and adolescents.[8-10] In addition, sexual harassment by peers and teachers is known to occur in SA schools, with a recent study reporting that as many as 14.8% of learners have experienced harassment.[11] Harassment causes depression, the inability to focus on academic tasks and school absenteeism, and can even be physically violent.[11]
Earlier research has found a relationship between various types of sexual abuse, including familial abuse, rape, incest and stranger-perpetrated sexual assault, and high-risk sexual behaviours.[12-14] The relationship between experiences of harassment in schools and risky sexual behaviours has been studied to a lesser extent.[15-17] This study aims to examine the relationship between peer- and teacher-perpetrated sexual harassment and risky sexual behaviours (namely the lack of condom use and having multiple sexual partnerships) among adolescents in SA schools.
Methods
This cross-sectional study analysed secondary data obtained from the 2011/2012 South African National HIV, Behaviour and Health Survey. The survey is the fourth in a series of population-based, nationally representative surveys conducted by the Human Sciences Research Council since 2002.[18] The survey used a multistage stratified cluster sampling design, with everyone in the sampled household invited to participate.[18] A total of 1 000 enumeration areas from the 2001 population census were randomly selected for the survey.[18] For the current study, data were used only from adolescents (10 - 19 years) who reported having had sexual intercourse in a 12-month period prior to the survey. The total weighted sample (N) was 10 254 975; however, for the purposes of this study, the sample was reduced to N=219 456 adolescents for whom complete information was available.
The two outcome variables in the study were condom use during last sexual activity and having multiple sexual partners. Condom use during last sexual activity was defined by asking participants whether they had used a condom the last time they had sex with their most recent partner. As our interest was lack of condom use, the response categories for this variable were coded as 0 for 'yes' and 1 for 'no' responses. To determine whether participants were involved in multiple concurrent sexual partnerships, they were asked how many sexual partners they had had in the previous 12 months. For the purposes of this study, participants who had fewer than two partners were considered to not be involved in multiple concurrent sexual partnerships while those who reported having had two or more partners were considered to be involved in multiple concurrent sexual partnerships. The response categories for this variable were coded as 1 for having two or more partners and 0 for having fewer than two partners.
The main predictor variable in this study was having experienced sexual harassment, assessed according to the following criteria: (i) boys sexually harassing girls by touching, threatening or making rude remarks to them; (ii) girls sexually harassing boys by touching, threatening or making rude remarks to them; (iii) male educators proposing relationships with female learners; (iv) female educators proposing relationships with male learners, and (v) educators proposing relationships with learners of the same sex. 'Peerperpetrated sexual harassment' refers to positive responses ('always' or 'often') to criterion i or ii, while positive responses to criterion iii, iv or v were coded as 'teacher-perpetrated sexual harassment' using principle component analysis.
The control variables in the study were: age (10 - 14 years or 15 - 19 years); sex (male or female); population group (black African or other); place of residence (rural or urban); age at first sex (<15 years or 16 - 18 years); highest level of education (primary or secondary), and HIV/AIDS knowledge. The reason for the specific categorisation of population group was that the survey sample included a majority of black African respondents (66.23%) and smaller percentages of white (6.22%), coloured (18.85%), Indian/Asian (8.59%) and other (0.10%) races.
The variable 'HIV/AIDS knowledge' was created from the following questions, to which respondents could answer 'yes, 'no' or 'don't know':
-
Can a person reduce the risk of HIV by having fewer sexual partners?
-
Can a healthy-looking person have HIV?
-
Can HIV be transmitted from a mother to her unborn child?
-
Can the risk of HIV transmission be reduced by having sex with only one partner?
-
Can a person be infected by HIV by sharing food with someone who is infected?
-
Can a person reduce the risk of HIV infection by using a condom every time he/she has sex?
-
Can medical male circumcision reduce the risk of HIV infection in males?
These questions were collapsed into two categories using principle component analysis, namely 'limited knowledge' and 'comprehensive knowledge'. 'Don't know' responses were excluded from the analysis.
Data were analysed at three levels. Descriptive analysis was used to show the frequency distribution of the two outcome variables (condom use at last sex; multiple sexual partnerships). A X test was used to test for an association between respondents' sociodemographic characteristics and experiences of sexual harassment, and the two outcome variables. For multivariate analysis, a binary logistic regression model was used to predict an association between experiences of sexual harassment and the two outcome variables, while controlling for other variables.
Results
Of the male respondents, 86.95% reported condom use during their last sexual activity, while 13.05% did not use condoms (Fig. 1). Of the female respondents, 74.20% reported using a condom during their last sexual intercourse. Results show that 42.2% of male respondents and 11.3% of female respondents had had multiple sexual partners in the 12-month period preceding the survey.
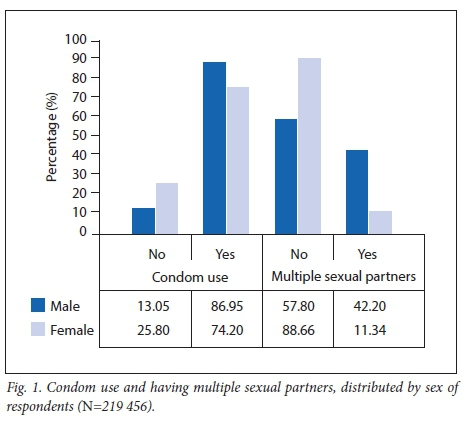
Table 1 shows that the sample included 54% male respondents and 46% female respondents, of whom 90% were black African. Approximately half (53.6%) of the respondents lived in urban areas. In addition, 82% of the respondents engaged in sexual intercourse for the first time between the age of16 and 18 years and most (95%) were in secondary school at the time of the survey. More than 60% of the respondents had comprehensive knowledge of HIV/AIDS.
Results also show that 27% and 14% of respondents who had experienced sexual harassment by peers and teachers, respectively, did not use a condom during their last sexual intercourse. In addition, 73% of the black African female respondents who engaged in sexual intercourse for the first time between the age of 16 and 18 years did not use a condom when last having sexual intercourse. A lack of condom use was more common among respondents without HIV knowledge, as 64% of them did not use co ndo ms during their last sexual activity. Place of residence did not affect condom use, as an equal percentage (50%) of respondents from urban and rural areas reported not having used a co ndom.
Furthermo re, the result s show that 27% and 12% of respondents who had experienced sexual harassment by peers and teachers, respectively, were involved in multiple concurrent sexual partnerships at the time of the survey. In addition, 57% of female respondents, 82% of black African respondents, 57% of respondents residing in urban areas and 88% of respondents who engaged in their first sexual activity between the age of 16 and 18 years were involved in multiple sexual partnerships.
While at school, 30.62% of respondents had experienced sexual harassment by peers, while 6.24% had experienced harassment by a teacher (Fig. 2). Of the respondents who had experienced sexual harassment by peers, 27.27% did not use a condom during their last sexual activity and 41.67% reported having multiple sexual partners in the preceding 12-month period. Of the respondents who had experienced sexual harassment by a teacher, 13.64% did not use a condom during their last sexual activity and 5.56% reported having multiple sexual partners in the preceding 12-month period.
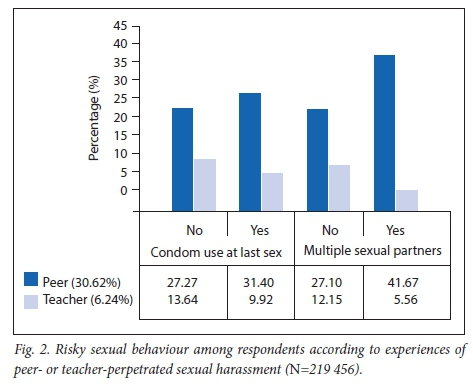
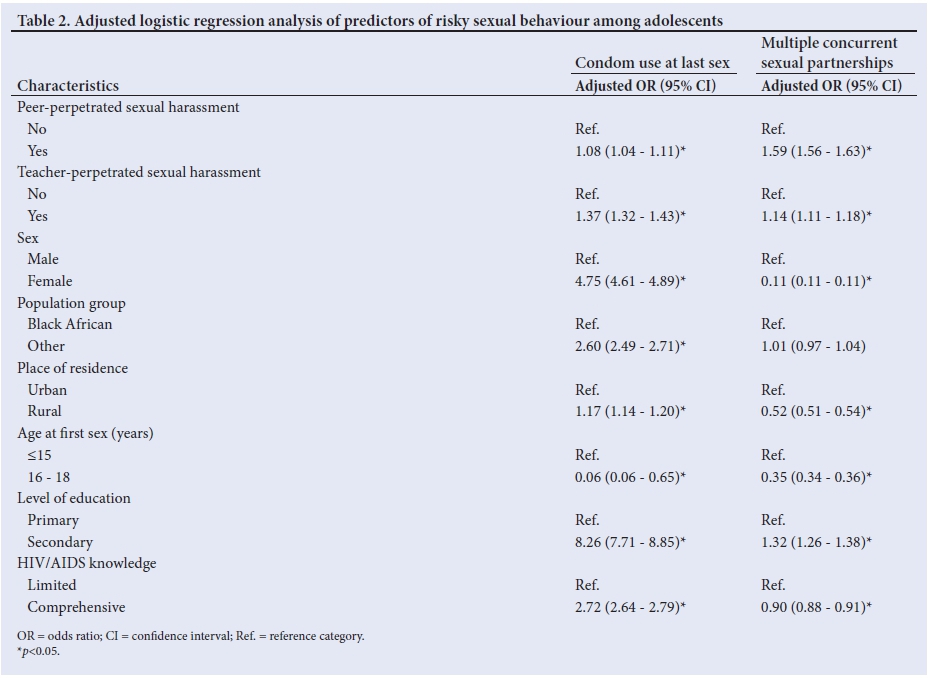
Table 2 shows the adjusted multivariate logistic regression results of all the selected variables. The results show that all the variables are significant predictors of not using a condom during the last sexual activity (all p-values <0.05). The results further show that sexual harassment by either peers or a teacher, the sex of the respondent, place of residence, age at first sex, level of education and knowledge about HIV/AIDS are significant predictors for being involved in multiple sexual partnerships. However, population group is not a significant predictor for multiple concurrent sexual partnerships. The results show that the odds for not using a condom during the last sexual activity are 1.08 times higher among respondents who reported experiencing sexual harassment by peers. Furthermore, the odds for not using a condom during the last sexual activity are also considerably higher among respondents who experienced teacher-perpetrated sexual harassment (odds ratio (OR) 1.37, p<0.05), female respondents (OR 4.75, p<0.05), those from race groups other than black African (OR 2.60, p<0.05) and respondents from rural areas (OR 1.17, p<0.05). An unanticipated finding is that the odds for not using a condom are 8.26 times higher among respondents with a secondary education and 2.72 times higher among respondents who have comprehensive HIV/AIDS knowledge compared with those who have only primary education and those who lack comprehensive knowledge about HIV/AIDS, respectively. Conversely, the odds for not using a condom are low (OR 0.06, p<0.05) among respondents who engaged in sexual intercourse between the age of 16 and 18 years.
The odds for being involved in multiple concurrent sexual partnerships are higher among respondents who have experienced sexual harassment by peers (OR 1.59, p<0.05) or teachers (OR 1.14, p<0.05) and among respondents who are in secondary school (OR 1.32, p<0.05). Conversely, the odds of being involved in multiple concurrent sexual partnerships are significantly lower among female respondents (OR 0.11, p<0.05), those who reside in rural areas (OR 0.52, p<0.05), those who engaged in sexual intercourse for the first time between the age of 16 and 18 (OR 0.35, p<0.05) and those who have comprehensive knowledge about HIV/AIDS (OR=0.90, p<0.05).
Discussion
Risky sexual behaviours among adolescents cause unintended pregnancies and the contraction of sexually transmitted infections.[19] These consequences affect development into adulthood and contribute to disease and mortality rates.[20] This study explored experiences of sexual harassment as a possible determinant of risky sexual behaviour and aims to expand the relevant knowledge by questioning the assumption of school environments protecting learners against risky sexual behaviours.
Experiences of sexual harassment at school are related to risky sexual behaviours such as engaging in unprotected sexual intercourse and multiple sexual partnerships. Research from elsewhere confirms this association.[16,21,22] In addition, Van Roode et al.[17]also report that the odds of not using a condom increase as a result of exposure to sexual harassment. Literature further suggests that victims of sexual harassment may be less assertive and have poorer sexual communication skills for successfully negotiating the use of condoms in their subsequent relationships.[23,24] Furthermore, an earlier study in SA schools found that adolescents who engage in risky sexual behaviours are more likely to have experienced multiple forms of victimisation at home and in their communities than those who do not engage in risky sexual behaviours.[25]
In our study, almost one-third of the respondents experienced sexual harassment by a fellow learner. This finding aligns with previous research in two SA provinces, which found 12.8% of adolescents experiencing sexual harassment in the 12 months prior to the interview.[11] Schools are meant to be protective environments conducive to learning, where adolescents should be free from abuse and harassment. The short-term consequences of sexual harassment in schools include victimisation and associated learning problems, while long-term consequences could include substance abuse, development of mental disorders such as depression, and possible engagement in risky sexual behaviours.[26,27] Sexual harassment at school undermines adolescents' ability to feel safe and sexually protected and prevents them from immersing themselves in the learning process.[28]
Study limitations
This study has several strengths. Firstly, the population size was large enough to conduct robust statistical analysis and produce statistically significant results. Secondly, the study provided a nationally representative sample to produce generalisable results with regard to adolescents who have experienced sexual harassment and engaged in risky sexual behaviours. This is crucial for introducing specific preventive interventions, as these adolescents may remain highly victimised throughout life.[29]
However, the study is not without its limitations. Experiences of sexual harassment, lack of condom use and involvement in multiple concurrent sexual partnerships may have been under-reported because of the social stigma associated with these behaviours. However, as significant associations were found between the main predictor and outcomes, this limitation is not regarded to have had serious implications for the findings of the study. In addition, causality could not be inferred between experiences of sexual harassment and risky sexual behaviours in this cross-sectional study.
Conclusion
Sexual harassment is a reality in SA schools and is associated with risky sexual behaviours. The large proportion of learners experiencing sexual harassment at school raises questions about the protective nature of these environments. More needs to be done to investigate the determinants of sexual harassment in schools and it is suggested that national bodies who are tasked with ensuring youth wellbeing at schools, including the departments of Social Development and Basic Education, need to implement programmes to address the causes and consequences of sexual harassment. For example, a better understanding of the type of environments that encourage peer harassment may help to direct implementation of intervention programmes among communities and households or through social media platforms. Also, other risky behaviours among adolescents who experience sexual harassment, such as illicit drug use and alcohol abuse, need to be investigated, as all forms of risky behaviour compromise health and progression to adulthood. Further research also needs to examine the causal relationship between harassment and risky sexual behaviours to help determine possible triggers.
Acknowledgements. The support of the DST-NRF Centre of Excellence in Human Development towards this research is hereby acknowledged. Opinions expressed and conclusions arrived at, are those of the author and are not necessarily to be attributed to the CoE in Human Development. The authors gratefully acknowledge the support of the Demography and Population Studies Programme, Schools of Public Health and Social Sciences, Faculties of Health Sciences and Humanities, University of the Witwatersrand, Johannesburg, South Africa.
Author contributions. KM was responsible for data analysis and prepared the manuscript. NdW conceptualised the study, reviewed and corrected the initial manuscript, and addressed all reviewer comments.
Funding. DST/NRF Centre of Excellence in Human Development Opportunity Grant was awared to NDW
Conflicts of interest. None.
References
1. Ugoji FN. Determinants of risky sexual behaviours among secondary school students in Delta State Nigeria. Int J Adolesc Youth 2014;19(3):408-418. https://doi.org/10.1080/02673843.2012.751040 [ Links ]
2. Eaton L, Flisher AJ, Aaro LE. Unsafe sexual behaviour in South African youth. Soc Sci Med 2003;56(1):149-165. https://doi.org/10.1016/s0277-9536(02)00017-5 [ Links ]
3. Stockl H, Kalra N, Jacobi J, Watts C. Is early sexual debut a risk factor for HIV infection among women in sub-Saharan Africa? A systematic review. Am J Reprod Immunol 2013;69(Suppl 1):27-40. https://doi.org/10.1111/aji.12043 [ Links ]
4. Gevers A, Mathews C, Cupp P, Russell M, Jewkes R. Illegal yet developmentally normative: A descriptive analysis of young, urban adolescents' dating and sexual behaviour in Cape Town, South Africa. BMC Int Health Hum Rights 2013;13:31. https://doi.org/10.1186/1472-698x-13-31 [ Links ]
5. Adeboye A, Yongsong Q, James N. Risky sexual behavior and knowledge of HIV/AIDS among high school students in Eastern Cape South Africa. J Hum Ecol 2016;53(3):194-204. https://doi.org/10.1080/09709274.2016.11906972 [ Links ]
6. Frank S, Esterhuizen T, Jinabhai CC, Sullivan K, Taylor M. Risky sexual behaviours of high-school pupils in an era of HIV and AIDS. S Afr Med J 2008;98(5):394-398. [ Links ]
7. Marin P, Brown B. The school environment and adolescent well-being: Beyond academics. Child Trends Research Brief. Washington DC: Child Trends, 2008. [ Links ]
8. Graham S. Victims of bullying in schools. Theor Pract 2016;55(2):136-144. https://doi.org/10.1080/00405841.2016.1148988 [ Links ]
9. Morton KL, Atkin AJ, Corder K, Suhrcke M, Van Sluijs EM. The school environment and adolescent physical activity and sedentary behaviour: A mixed-studies systematic review. Obes Rev 2016;17(2):142-158. https://doi.org/10.1111/obr.12352 [ Links ]
10. Owusu JS, Colecraft EK, Aryeetey RN, Vaccaro JA, Huffman FG. Comparison of two school feeding programmes in Ghana, West Africa. Int J Child Health Nutr 2016;5(2):56-62. https://doi.org/10.6000/1929-4247.2016.05.02.2 [ Links ]
11. Meinck F, Cluver LD, Boyes ME, Loening-Voysey H. Physical, emotional and sexual adolescent abuse victimisation in South Africa: Prevalence, incidence, perpetrators and locations. J Epidemiol Community Health 2016;70(9):910-916. https://doi.org/10.1037/e500792015-238 [ Links ]
12. Toska E, Cluver LD, Boyes M, Pantelic M, Kuo C. From 'sugar daddies' to 'sugar babies': Exploring a pathway among age-disparate sexual relationships, condom use and adolescent pregnancy in South Africa. Sex Health 2015;12(1):59-66. https://doi.org/10.1071/sh14089 [ Links ]
13. Zierler S, Feingold L, Laufer D, Velentgas P, Kantrowitz-Gordon I, Mayer K. Adult survivors of childhood sexual abuse and subsequent risk of HIV infection. Am J Public Health 1991;81(5):572-575. https://doi.org/10.2105/ajph.81.5.572 [ Links ]
14. Ackermann L, De Klerk GW. Social factors that make South African women vulnerable to HIV infection. Health Care Women Int 2002;23(2):163-172. https://doi.org/10.1080/073993302753429031 [ Links ]
15. Hong JS, Voisin DR, Cho SC, Espelage DL. Association among subtypes of bullying status and sexually-risky behaviors of urban African American adolescents in Chicago. J Immigr Minor Health 2016;18(5):1007-1016. https://doi.org/10.1007/s10903-016-0375-5 [ Links ]
16. Cunningham RM, Stiffman AR, Doré P, Earls F. The association of physical and sexual abuse with HIV risk behaviors in adolescence and young adulthood: Implications for public health. Child Abuse Negl 1994;18(3):233-245. https://doi.org/10.1016/0145-2134(94)90108-2 [ Links ]
17. Van Roode T, Dickson N, Herbison P, Paul C. Child sexual abuse and persistence of risky sexual behaviors and negative sexual outcomes over adulthood: Findings from a birth cohort. Child Abuse Negl 2009;33(3):161-172. https://doi.org/10.1016/j.chiabu.2008.09.006 [ Links ]
18. Shisana O, Rehle T, Simbayi LC, et al. South African national HIV prevalence, incidence and behaviour survey. Cape Town: HSRC Press, 2014. [ Links ]
19. Bearinger LH, Sieving RE, Ferguson J, Sharma V. Global perspectives on the sexual and reproductive health of adolescents: Patterns, prevention, and potential. Lancet 2007;369(9568):1220-1231. https://doi.org/10.1016/s0140-6736(07)60367-5 [ Links ]
20. Bogg T, Roberts BW. Conscientiousness and health-related behaviors: A meta-analysis of the leading behavioral contributors to mortality. Psychol Bull 2004;130(6):887-919. https://doi.org/10.1037/0033-2909.130.6.887 [ Links ]
21. NIMH Multisite HIV Prevention Trial Group. A test of factors mediating the relationship between unwanted sexual activity during childhood and risky sexual practices among women enrolled in the NIMH Multisite HIV Prevention Trial. Women Health 2001;33(1-2):163-180. https://doi.org/10.1300/j013v33n01_10 [ Links ]
22. Elze DE, Auslander W, McMillen C, Edmond T, Thompson R. Untangling the impact of sexual abuse on HIV risk behaviors among youths in foster care. AIDS Educ Prev 2001;13(4):377-389. https://doi.org/10.1521/aeap.13.4.377.21427 [ Links ]
23. Clum GA, Chung S-E, Ellen JM, et al. Victimization and sexual risk behavior in young, HIV positive women: Exploration of mediators. AIDS Behav 2012;16(4):999-1010. https://doi.org/10.1007/s10461-011-9931-0 [ Links ]
24. Mullen PE, Martin JL, Anderson JC, Romans SE, Herbison GP. The effect of child sexual abuse on social, interpersonal and sexual function in adult life. Br J Psychiatry 1994;165(1):35-47. https://doi.org/10.1192/bjp.165.1.35 [ Links ]
25. Leoschut L, Kafaar Z. The frequency and predictors of poly-victimisation of South African children and the role of schools in its prevention. Psychol Health Med 2017;22(Suppl 1):81-93. https://doi.org/10.1080/13548506.2016.1273533 [ Links ]
26. Sweeting H, Young R, West P, Der G. Peer victimization and depression in early-mid adolescence: A longitudinal study. Br J Educ Psychol 2006;76(3):577-594. https://doi.org/10.1348/000709905x49890 [ Links ]
27. Perez DM. The relationship between physical abuse, sexual victimization, and adolescent illicit drug use. J Drug Issues 2000;30(3):641-662. https://doi.org/10.1177/002204260003000308 [ Links ]
28. Espelage DL, Aragon SR, Birkett M, Koenig BW. Homophobic teasing, psychological outcomes, and sexual orientation among high school students: What influence do parents and schools have? School Psychol Rev 2008;37(2):202-216. [ Links ]
29. Finkelhor D, Turner H, Hamby SL, Ormrod R. Polyvictimization: Children's exposure to multiple types of violence, crime, and abuse. National survey of children's exposure to violence. Juvenile Justice Bulletin. Washington DC: Office of Juvenile Justice and Delinquency Prevention, 2011. [ Links ]
 Correspondence:
Correspondence:
K Mabetha
khuthala.mabetha@wits.ac.za
Accepted 20 April 2018


{kind=link}
{kind=link}