










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.12 no.3 Pretoria Jul./Set. 2018
http://dx.doi.org/10.7196/sajch.2018.v12i3.1528
ARTICLE
Traditional red cell indices are not suggestive of iron deficiency in children with chronic kidney disease
A MudiI, II; C LevyIII, IV
IMBBS, FWACP, Cert Nephrol (Paed), PhD; Department of Paediatrics, Faculty of Clinical Sciences, Bayero University, Kano, Nigeria
IIMBBS, FWACP, Cert Nephrol (Paed), PhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB BCh, FCPaed, MMed, Cert Nephrol (Paed); MBBS, FWACP, Cert Nephrol (Paed), PhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVMB BCh, FCPaed, MMed, Cert Nephrol (Paed) Department of Paediatric Nephrology, Nelson Mandela Children's Hospital, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Iron deficiency (ID) contributes significantly to the chronic anaemia seen in chronic kidney disease (CKD). The use of traditional red cell indices such as mean corpuscular volume (MCV), mean corpuscular haemoglobin (MCH), mean corpuscular haemoglobin concentration (MCHC) and red cell distribution width (RCDW) in screening for ID has been recommended, because they are inexpensive and widely available, especially in low-income settings.
OBJECTIVES. To determine the prevalence of anaemia and ID, and the role of traditional red cell indices in screening for ID in children with CKD.
METHODS. A sample of 130 children (aged 5 - 18 years) with various stages of CKD was recruited. Blood samples were taken and assessed for traditional red cell indices (MCV, MCH, MCHC and RCDW), serum haemoglobin, creatinine, C-reactive protein, iron, transferrin, transferrin saturation (TSAT) and ferritin.
RESULTS. The mean (standard deviation) age was 10.7 (3.6) years, with a male-to-female ratio of 1.8:1. There was a high prevalence (32%) of anaemia among the patients. The median TSAT and ferritin were 19 (range 13 - 26)% and 50 (28 - 102) ng/mL, respectively. The prevalence of ID and ID with anaemia (IDA) was 43% and 11%, respectively. The majority of the patients (110/130; 85%) were iron deplete, and serum ferritin and RCDW were found to be independent predictors for anaemia, ID and IDA. There was no significant difference in the traditional red cell indices in iron-deplete and iron-replete patients.
CONCLUSION. The routine use of traditional red cell indices alone in screening for ID in children with CKD should be discouraged.
Anaemia is frequently seen in children with chronic kidney disease (CKD), where it has been associated with increased morbidity and mortality.[1-3] Iron deficiency (ID) contributes significantly to the chronic anaemia seen in CKD, especially in patients on maintenance dialysis.[4] Other causes of anaemia include erythropoietin deficiency, decreased red cell survival, chronic inflammation, poor nutrition and marrow hyporesponsiveness.[4,6]
ID in CKD has been attributed to chronic blood loss, poor gut absorption, reduced intake or poor nutrition, chronic inflammation and increased requirements owing to therapy with erythropoiesis stimulating agents.[7] In addition to anaemia, ID has also been implicated in lower cognitive function in children, and long-term developmental outcomes.[8-10]
Both the Kidney Diseases Outcome Quality Initiative (KDOQI) [11] and the Kidney Disease Improving Global Outcomes (KDIGO)[12] clinical practice guidelines for anaemia in CKD recommend the use of iron parameters, namely serum ferritin and transferrin saturation (TSAT), in determining the iron status in CKD, as routine direct quantification of body iron stores by bone marrow iron staining is impracticable. More effective methods for assessing iron status include measuring the percentage of circulating hypochromic red blood cells (PHRC) and the reticulocyte haemoglobin content (CHr), but they are not widely available.[13-15]
The use of haemoglobin levels and other traditional red cell indices, such as mean corpuscular volume (MCV), mean corpuscular haemoglobin (MCH), mean corpuscular haemoglobin concentration (MCHC) and red cell distribution width (RCDW), in screening for ID has also been recommended, because they are inexpensive and widely available.[16,17] However, these measures are often late indicators of ID, have low specificity and sensitivity and their normal values differ with age, sex and race.[16-18]
In our experience, in poor-resource settings, especially in Africa, where means of assessing for ferritin and TSAT are expensive or not readily available, clinicians often use traditional red cell indices to screen for ID in children with CKD, despite the drawbacks mentioned above. The present study determined the prevalence of anaemia and ID, and the role of red cell indices in screening for ID in children with CKD.
Methods
One hundred and thirty children (aged 5 - 18 years) with various stages of CKD, including those on maintenance dialysis being followed up in the Divisions of Paediatric Nephrology of the Charlotte Maxeke Johannesburg Academic Hospital and Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa (SA), were recruited consecutively between August 2015 and July 2016. Ninety-four patients had pre-dialysis CKD (GFR >15 mL/ min/1.73 m2), and 36 patients were on maintenance haemodialysis and peritoneal dialysis. The pre-dialysis group comprised 58 CKD-I, 19 CKD-II, 11 CKD-III and 6 CKD-IV patients. Patients who had received a blood transfusion in the last 4 months were excluded. There were no known patients with haemoglobinopathies in the study group.
All patients had a short demographic and clinical history taken, along with a physical examination. Routine blood samples for red cell indices (MCV, MCH, MCHC and RCDW), serum haemoglobin, creatinine, C-reactive protein (CRP), iron, transferrin, TSAT and ferritin were analysed.
Anaemia was defined based on age and gender, and the severity of anaemia was graded into mild, moderate and severe.[11,12,19] Microcytosis was defined for age,[20] and elevated CRP classified as >10 mg/L.[21] Low TSAT was defined as <20%, and low ferritin as <100 ng/mL in all children with CKD.[1,112,22] Absolute ID was defined as low TSAT and ferritin, functional ID as low TSAT and normal ferritin, ID anaemia (IDA) as having ID with anaemia, iron deplete as low TSAT and/or low ferritin, and iron replete as normal TSAT and ferritin.
Data analysis
All data were collected and managed using research electronic data capture (REDCap) tools, hosted at the University of the Witwatersrand, Johannesburg, SA.[23] Computer-based statistical package Stata 13.1 (StataCorp, USA) was used for the analysis. Continuous variables were described using means and standard deviations (SDs) for data normally distributed, and medians and interquartile ranges for skewed data. Categorical variables were presented as percentages and frequencies. Statistical significance in the prevalence of risk factors was tested for using tests, or Fisher's exact test where appropriate. The mean/median values of the different groups were compared using f-tests and Mann-Whitney U tests, depending on the distribution of the data. Logistic regression was used to determine the predictors of anaemia, ID and IDA. A confidence interval of 95% was used, and p<0.05 was regarded as significant.
Ethics and permission
The study was approved by the University of the Witwatersrand Human Research Ethics Committee (ref. no. M150312), and was conducted in conformance with the Helsinki Declaration and Good Clinical Practice guidelines, and within the laws and regulations of SA. Written consent was obtained from each participating parent/ guardian, with assent from those children >8 years old.
Results
The mean (SD) age was 10.7 (3.6) years, with a male-to-female ratio of 1.8:1. Thirty-two (25%) of the patients were on oral iron supplements, and 32 (25%) on erythropoietin. Twenty-one (16%) had an elevated CRP (>10 mg/L) (Table 1). There was a high prevalence (41/130; 32%) of anaemia among the patients, and the dialysis CKD patients had a higher prevalence of anaemia (30/36; 83%) than the pre-dialysis group (11/94; 12%) (Table 2).
The traditional red cell indices (mCV, MCH, MCHC and RCDW) for the patients can be seen in Table 1. Microcytosis was observed in 28/130 (22%) and macrocytosis in 3/130 (2%) of the patients. A higher prevalence of microcytosis (22/94; 23%) was recorded in the pre-dialysis group when compared with the dialysis group (6/36; 17%). Macrocytosis was exclusively seen in the dialysis group.
The median (interquartile range; IQR) TSAT and ferritin were 19 (13 - 26)% and 50 (28 - 102) ng/mL respectively. There was no significant difference in the TSAT levels in the pre-dialysis and dialysis group (p=0.120), but a significant difference was noted when patients on iron supplements were excluded (p=0.034) (Table 2). Ferritin levels were significantly higher in the dialysis group than the pre-dialysis group (p<0.001) (Table 2). There was a higher prevalence of abnormal CRP in the dialysis group, when compared with the pre-dialysis group (p=0.026), and a weak correlation between CRP and ferritin levels was also observed p=0.28; p=0.002.
Low TSAT was recorded in 72 (55%) patients (Table 1). There was no significant difference in the prevalence of low TSAT among the two CKD groups (p=0.109) (Table 2). However, when patients on iron supplements and patients with an elevated CRP were excluded, a significant difference was observed between the two study groups (p<0.05). Low ferritin was observed in 94 (72%) patients (Table 1).
There was a significant difference in the prevalence of low ferritin between the two study groups (p<0.005) (Table 2).
Absolute and functional ID were observed in 56 (43%) and 16 (12%) patients, respectively (Table 1). There was no significant difference in the prevalence of absolute ID when compared between the pre-dialysis and dialysis patients (p=0.551). Functional ID was observed to be more common in the dialysis group than the pre-dialysis group (p<0.050) (Table 2).
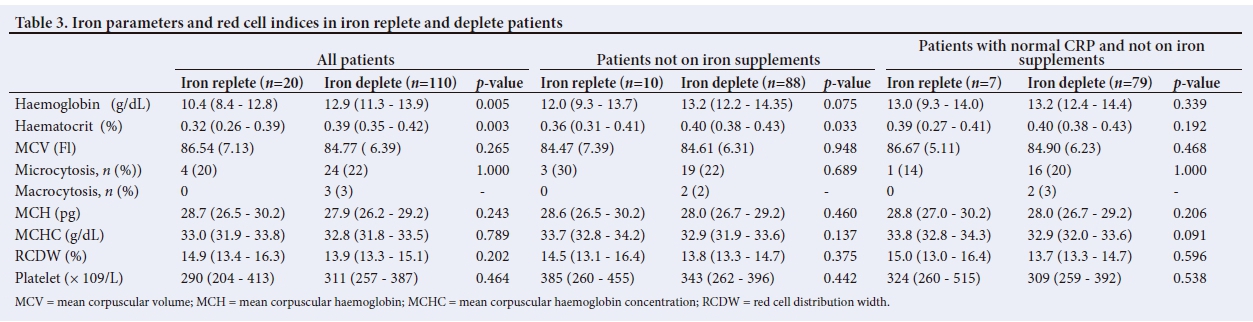
IDA was observed in 14 (11%) of the patients. The prevalence of IDA was found to be significantly higher in the dialysis patients (9/36; 25%) than the pre-dialysis patients (5/94; 5%) (p<0.001). The majority of the patients (110/130; 85%) were observed to be iron deplete, and no significant difference was observed in the prevalence of iron deplete status between the pre-dialysis and dialysis CKD groups (p>0.050) (Table 2). In spite of the significant difference in haemoglobin levels between patients who were iron deplete and those who were iron replete, we did not observe any significant difference in the red cell indices in these patients (Table 3). We also did not observe any significant difference in the haemoglobin levels and red cell indices between iron-deplete and iron-replete patients in a subgroup analysis for the pre-dialysis and dialysis patients, even when patients on iron supplements and patients with an elevated CRP were excluded (p>0.050).
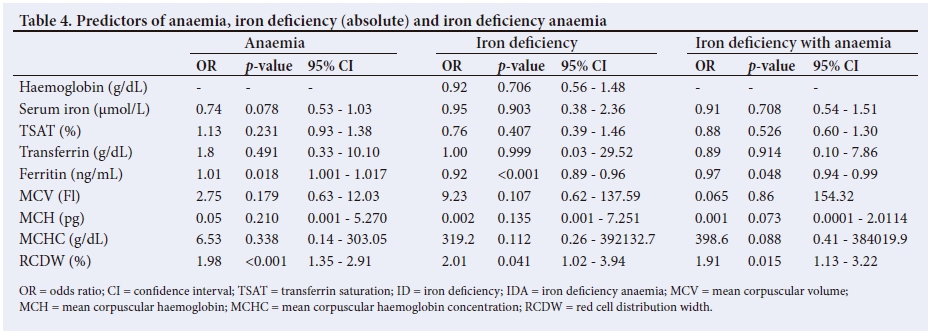
Serum ferritin and RCDW were found to be the only independent predictors for anaemia, iron deficiency and IDA (p<0.050) (Table 4).
Discussion
Frequent occurrence of anaemia has been reported in children with CKD, including patients on maintenance dialysis. We found a high prevalence (32%) of anaemia in our cohort, and the majority of those children with anaemia were on maintenance dialysis. Wong et al.,[24] in a multicentre study that recruited children in all stages of CKD, found a similar prevalence of 37%,while Rinat et al.[25] reported a prevalence of 54% in a group of children with CKD 3-5. The Chronic Kidney Disease in Children (CKiD) study and the North American Pediatric Renal Trials and Collaborative Studies database (NAPRTCS) also report the high prevalence of anaemia (45% and 44%, respectively) in children with CKD, but their reports only looked at children with pre-dialysis CKD.[1,2]
There are a number ofpossible explanations for the disparity in the reported prevalence of anaemia in children with CKD' not least of which are the differences in the cohorts in terms of CKD groups, and also the various definitions of anaemia used in the different studies. The majority of the studies referred to above were carried out before the release of the KDIGO guideline for anaemia, and they relied on the KDOQI and the Third National Health and Nutritional Examination Survey (NHANES III) definitions of anaemia.[11'12'26] Furthermore, some of the studies used haemoglobin or haematocrit z-scores or percentile-for-age to define anaemia, while others used fixed values such as haematocrit levels <33% or haemoglobin levels <11 g/dL for all ages.[1,2,25,27] For example, the NAPRTCS study used two definitions of anaemia: a haematocrit z-score of <-2 SD, and a haematocrit level <33%. The study reported a higher prevalence of anaemia when the z-scores were used rather than haematocrit levels, at 44% and 35%, respectively.[2]
Although our study observed a high prevalence of anaemia (83%) in the dialysis patients, in keeping with previously reported ranges (65 - 93%), we found a significantly lower prevalence of anaemia (12%) in the pre-dialysis group than those found by the CKiD and NAPRTCS reports. This difference may be due to the composition of our pre-dialysis group, where the majority had mild disease compared with the subjects in the CKiD and NAPRTCS studies, in which the majority of their patients had moderate to advanced disease.[1,21 The significantly high prevalence of anaemia (83%) observed in the dialysis patients in our study is in keeping with previous reports (65 - 93%).[24,25]
The predominant morphologic pattern of anaemia in CKD has been described as similar to the pattern seen in anaemia of chronic disease.[121 In CKD, microcytosis may be attributed to ID and/or haemoglobinopathies, while macrocytosis may be attributed to folate and/or vitamin B12 deficiency.[12] In keeping with a previous report, our study reports a higher prevalence of microcytosis than macrocytosis, with the former being more common in the pre-dialysis group and the latter being more common in the dialysis group.[28]
The overall median TSAT and ferritin levels in our patients differ from those reported by Atkinson et al.[29]They reported higher TSAT levels and lower ferritin levels than those found in our study. These differences may be attributed to the difference in patient selection method; our study recruited children with all stages of CKD, including those on dialysis, while Atkinson et al. recruited only children with mild to moderate CKD (pre-dialysis CKD). It is interesting that when we excluded patients on iron supplementation and those with inflammation, as defined by an elevated CRP, from our pre-dialysis patients, our results were similar to the values reported by Atkinson et al.
The finding of a higher TSAT levels in the pre-dialysis group than the dialysis group, and the reverse pattern in the case of ferritin levels in our patients, may be related to disease severity. With advancing disease, TSAT levels are expected to be lower than in patients with mild to moderate disease, especially in dialysis patients, owing to chronic blood loss, poor gut absorption, reduced intake/poor nutrition and increased requirements due to therapy with erythropoiesis-stimulating agents.[4,7] Similarly, as a result ofthe increased risk of inflammation with advancing CKD, especially in dialysis patients, ferritin, which is an acute-phase reactant, may be much higher in those with advanced CKD than in those with mild to moderate disease[13,29,30]
In our study, the majority (82%) of the pre-dialysis patients failed to meet the criteria for normal ferritin levels (>100 ng/mL) recommended by the KDOQI and KDIGO guidelines, and this is in keeping with the high prevalence of low ferritin (93%) reported in the CKiD study.[29] In spite of the mild to moderate disease in pre-dialysis CKD, and the knowledge that inflammation increases with advancing CKD, especially in patients on dialysis, the 100 ng/mL cut-off value for ferritin may be too high for pre-dialysis paediatric CKD. This may be the reason why Baracco et al.[22]used lower cutoff values for ferritin to define ID in their CKD patients.
In spite of the differing definitions of abnormal ferritin levels used, the prevalence of ID in the pre-dialysis patients in our study (45%) is similar to that reported by Baracco et al.[22]in pre-dialysis patients. The prevalence of IDA in children with CKD increases with the progression of CKD, and tends to be highest in patients on dialysis, and especially haemodialysis.[4,22] A similar pattern of IDA was observed in our study.
Serum ferritin levels, and not TSAT levels, have been shown to be strongly associated with haemoglobin levels.[29] A similar association between ferritin levels and anaemia (p=0.018) was observed in our patients. Furthermore, ferritin levels and RCDW were found to be the independent predictors of anaemia, ID and IDA (p<0.050).
In summary, our results confirm that the traditional red cell indices (MCV, MCH, MCHC and RCDW) have a low specificity and sensitivity for distinguishing between iron-deplete and iron-replete patients, and also tend to be late indicators of ID.[16,18] Therefore it is important to emphasise that the routine use of red cell indices such as MCV, MCH, MCHC and RCDW in screening for ID in children with CKD by clinicians in poor-resource settings should be discouraged.
Limitations
This study highlights the problem associated with the use of traditional red cell indices alone in screening for ID in children with CKD. The major limitations are the small sample size and the fact that the study did not assess other markers of anaemia such as absolute reticulocyte count, reticulocyte haemoglobin concentration and vitamin B12 and folate blood levels.
Conclusion
This comparative study demonstrated a high prevalence of anaemia and ID in children with CKD, with the dialysis patients having a higher prevalence than their pre-dialysis counterparts. In addition to the significant relationship between anaemia and ferritin levels observed in this study, ferritin levels and RCDW were found to be independent predictors of anaemia, ID and IDA. The study also reports no significant difference in the traditional red cell indices (MCV, MCH, MCHC and RCDW) of iron-deplete and iron-replete patients, and therefore the routine use of these indices alone in screening for ID in children with CKD may be misleading. We advise the use of serum iron parameters, rather than red cell indices alone, to assess for ID in CKD, as recommended by the KDIGO guidelines.
Acknowledgements. The authors acknowledge the contribution of all team members who provided care for these children and assisted with this study.
Author contributions. Both authors have contributed to all aspects of the research and preparation of the manuscript; they have reviewed and approved its submission to the publishing journal.
Funding. None.
Conflicts of interest. None.
References
1. Fadrowski JJ, Pierce CB, Cole SR, Moxey-Mims M, Warady BA, Furth SL. Haemoglobin decline in children with chronic kidney disease: Baseline results from the Chronic Kidney Disease in Children prospective cohort study. Clin J Am Soc Nephrol 2008;3(2):457-462. https://doi.org/10.2215/cjn.03020707 [ Links ]
2. Staples AO, Wong CS, Smith JM, et al. Anemia and risk of hospitalization in pediatric chronic kidney disease. Clin J Am Soc Nephrol 2009;4(1):48-56. https://doi.org/10.2215/cjn.05301107 [ Links ]
3. Akizawa T, Gejyo F, Nishi S, et al. Positive outcomes of high hemoglobin target in patients with chronic kidney disease not on dialysis: A randomized controlled study. Trier Apher Dial 2011;15(5):431-440. https://doi.org/10.1111/j.1744-9987.2011.00931.x [ Links ]
4. Koshy SM, Geary DF. Anemia in children with chronic kidney disease. Pediatr Nephrol 2008;23(2):209-219. https://doi.org/10.1007/s00467-006-0381-2 [ Links ]
5. McGonigle RJ, Wallin JD, Shadduck RK, Fisher JW. Erythropoietin deficiency and inhibition of erythropoiesis in renal insufficiency. Kidney Int 1984;25(2):437-444. [ Links ]
6. Ly J, Marticorena R, Donnelly S. Red blood cell survival in chronic renal failure. Am J Kidney Dis 2004;44(4):715-719. https://doi.org/10.1053/j.ajkd.2004.06.018 [ Links ]
7. Horl WH. Clinical aspects of iron use in the anemia of kidney disease. J Am Soc Nephrol 2007;18(2):382-393. https://doi.org/10.1681/asn.2006080856 [ Links ]
8. Ji X, Cui N, Liu J. Neurocognitive function is associated with serum iron status in early adolescents. Biol Res Nurs 2017;19(3):269-277. https://doi.org/10.1177/1099800417690828 [ Links ]
9. Halterman JS, Kaczorowski JM, Aligne CA, Auinger P, Szilagyi PG. Iron deficiency and cognitive achievement among school-aged children and adolescents in the United States. Pediatrics 2001;107(6):1381-1386. https://doi.org/10.1542/peds.107.6.1381 [ Links ]
10. Lozoff B, Jimenez E, Wolf AW. Long-term developmental outcome of infants with iron deficiency. N Engl J Med 1991;325(10):687-694. https://doi.org/10.1056/NEJM199109053251004 [ Links ]
11. National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for anemia in chronic kidney disease. Am J Kidney Dis 2006;47(5 Suppl 3):S11-S145. [ Links ]
12. KDIGO [Kidney Disease Improving Global Outcomes]. Clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl 2012;2(4):279-335. [ Links ]
13. Ratcliffe LE, Thomas W, Glen J, et al. Diagnosis and management of iron deficiency in CKD: A summary of the NICE guideline recommendations and their rationale. Am J Kidney Dis 2016;67(4):548-558. https://doi.org/10.1053/.ajkd.2015.11.012 [ Links ]
14. Schapkaitz E, Buldeo S, Mahlangu JN. Diagnosis of iron deficiency anaemia in hospital patients: Use of the reticulocyte haemoglobin content to differentiate iron deficiency anaemia from anaemia of chronic disease. S Afr Med J 2016;106(1):53-54. https://doi.org/10.7196/SAMJ.2016.v106i1.9934 [ Links ]
15. Urrechaga E, Borque L, Escanero JF. Biomarkers of hypochromia: The contemporary assessment of iron status and erythropoiesis. Biomed Res Int 2013;1:603786. https://doi.org/10.1155/2013/603786 [ Links ]
16. Cook JD. Diagnosis and management of iron-deficiency anaemia. Best Pract Res Clin Haematol 2005;18(2):319-332. https://doi.org/10.1016/j.beha.2004.08.022 [ Links ]
17. Goddard AF, James MW, McIntyre AS, Scott BB, British Society of Gastroenterology. Guidelines for the management of iron deficiency anaemia. Gut 2011;60(10):1309-1316. https://doi.org/10.1136/gut.2010.228874 [ Links ]
18. Beutler E, West C. Hematologic differences between African-Americans and whites: The roles of iron deficiency and alpha-thalassemia on hemoglobin levels and mean corpuscular volume. Blood 2005;106(2):740-745. https://doi.org/10.1182/blood-2005-02-0713 [ Links ]
19. World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Geneva: WHO, 2011. http://www.who.int/vmnis/indicators/haemoglobin/en/ (accessed 30 June 2017). [ Links ]
20. Ozdemir N. Iron deficiency anemia from diagnosis to treatment in children. Turk Pediatri Ars 2015;50(1):11-19. https://doi.org/10.5152/tpa.2015.2337 [ Links ]
21. McIntyre C, Harper I, Macdougall I, Raine A, Williams A, Baker L. Serum C-reactive protein as a marker for infection and inflammation in regular dialysis patients. Clinical Nephrol 1997;48(6):371-374. [ Links ]
22. Baracco R, Saadeh S, Valentini R, Kapur G, Jain A, Mattoo TK. Iron deficiency in children with early chronic kidney disease. Pediatr Nephrol 2011;26(11):2077-2080. https://doi.org/10.1007/s00467-011-1946-2 [ Links ]
23. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-381. https://doi.org/10.1016/j.jbi.2008.08.010 [ Links ]
24. Wong H, Mylrea K, Feber J, Drukker A, Filler G. Prevalence of complications in children with chronic kidney disease according to KDOQI. Kidney Int 2006;70(3):585-590. https://doi.org/10.1038/sj.ki.500160825 [ Links ]
25. Rinat C, Becker-Cohen R, Nir A, et al. A comprehensive study of cardiovascular risk factors, cardiac function and vascular disease in children with chronic renal failure. Nephrol Dial Transplant 2010;25(3):785-793. https://doi.org/10.1093/ndt/gfp57026 [ Links ]
26. US Department of Health and Human Services. Third National Health and Nutrition Examination Survey, 1988 - 1994, NHANES III. Hyattsville: National Center for Health Statistics, 1996. https://wwwn.cdc.gov/nchs/data/nhanes3/3a/VIFSE-acc.pdf (accessed 6 October 2017). [ Links ]
27. Atkinson MA, Martz K, Warady BA, Neu AM. Risk for anemia in pediatric chronic kidney disease patients: A report of NAPRTCS. Pediatr Nephrol 2010;25(9):1699-1706. https://doi.org/10.1007/s00467-010-1538-6 [ Links ]
28. Afshar R, Sanavi S, Salimi J, Ahmadzadeh M. Hematological profile of chronic kidney disease (CKD) patients in Iran, in pre-dialysis stages and after initiation of hemodialysis. Saudi J Kidney Dis Transpl 2010;21(2):368-371. [ Links ]
29. Atkinson MA, Pierce CB, Fadrowski JJ, et al. Association between common iron store markers and hemoglobin in children with chronic kidney disease. Pediatr Nephrol 2012;27(12):2275-2283. https://doi.org/10.1007/s00467-012-2266-x [ Links ]
30. Bonanni A, Sofia A, Saffioti S, et al. The human kidney as a regulator of body cytokine homeostasis. J Biol Res 2011;84(1):76-78. https://doi.org/10.4081/jbr.2011.4498 [ Links ]
 Correspondence:
Correspondence:
A Mudi
abdulmudi@gmail.com
Accepted 20 April 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}