










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.12 n.3 Pretoria Jul./Sep. 2018
http://dx.doi.org/10.7196/sajch.2018.v12i3.1477
ARTICLE
Ownership of mobile phones and willingness to receive childhood immunisation reminder messages among caregivers of infants in Ondo State, south-western Nigeria
O T AkinrinadeI; I O AjayiII; A A FatiregunIV; E E IsereV; B O YusufIII
IBTech, MPH;; African Field Epidemiology Network (AFENET), Ondo State, Nigeria
IIMBBS, MCLSC, MPH, PhD, FMCGP, FWACP; Department of Epidemiology and Medical Statistics, Faculty of Public Health, University of Ibadan, Nigeria
IIIBSc, MSc, PhD, CStat; Department of Epidemiology and Medical Statistics, Faculty of Public Health, University of Ibadan, Nigeria
IVMBBS, MSc Epid, FWACP; World Health Organization, Ondo State Office, Nigeria
VBSc, MPH; World Health Organization, Ondo State Office, Nigeria
ABSTRACT
BACKGROUND. The timely completion of the childhood immunisation schedule for children under the age of 1 year by caregivers is key to reducing the high morbidity and mortality of vaccine-preventable diseases among infants globally.
OBJECTIVE. To determine the ownership of mobile phones among caregivers of children under the age of 1 year, their knowledge about immunisation service delivery and willingness to receive childhood immunisation schedule reminder messages in Ondo State, south-western Nigeria.
METHOD. A descriptive cross-sectional study using semi-structured interviewer-administered questionnaires was conducted with 615 caregivers of infants, who brought their children to clinics conducting immunisation in 24 health facilities in rural, semi-urban and urban settlements in Ondo State in December 2014.
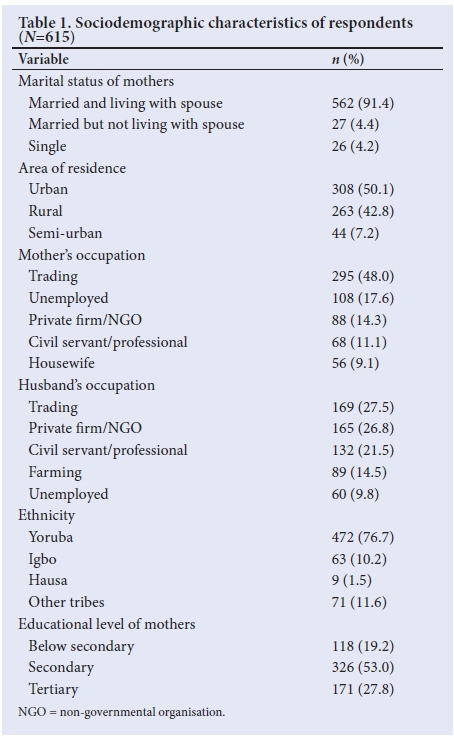
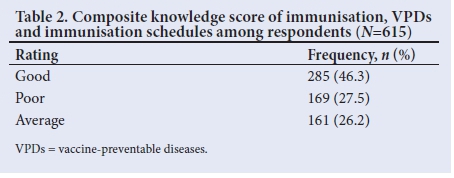
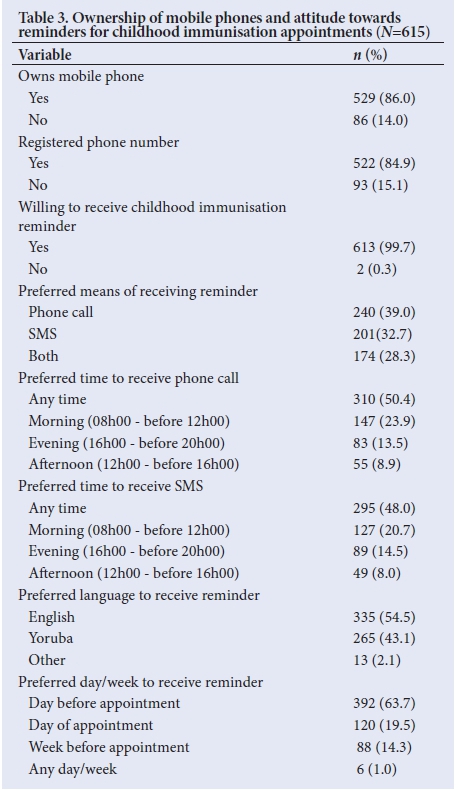
RESULTS. The mean (standard deviation, SD) age of respondents was 28.49 (6.01) years, 76.7% were Yoruba, 91.4% were married and living with their spouses and 4.2% were single. Mobile phone ownership was 74.5% among rural-based respondents, and 95.8% among urban-based. Forty-six percent of the respondents had good knowledge of immunisation, vaccine-preventable diseases and vaccination schedules, while 27.5% had poor knowledge. The majority of the respondents (99.7%) were willing to receive childhood immunisation reminder messages on their mobile phones. About 50% of the respondents preferred to receive reminder messages at any time, rather than specific times. The most preferred language for reminders was English (54.5%). Residing in an urban area and having post-secondary education were predictors of mobile phone ownership.
CONCLUSION. The high mobile phone ownership level, and the willingness of caregivers of infants in this study area to receive immunisation schedule reminder messages, is encouraging, and should be optimised to improve routine immunisation uptake. However, caregivers of infants in rural areas need to be provided with mobile phone support, and trained in their usage in order to benefit from such an intervention in childhood immunisation.
Immunisation remains the most cost-effective and important public health strategy for disease prevention.[1] Vaccine-preventable diseases (VPDs) such as tuberculosis, poliomyelitis, diphtheria, tetanus, Haemophilus influenzae type B and measles are the main causes of morbidity and mortality in children, especially in developing countries such as Nigeria.[2] Recently, Nigeria has been reported to have the second highest under-5 mortality rate in the world, with about 2 300 deaths of children under the age of 5 recorded daily.[2] The World Health Organization stated in 2012 that the estimated number of all deaths of children under 5 years old from VPDs was 1.49 million in 2008.[3] It is recognised that timely vaccination, particularly within the first 6 months of life, is extremely important in reducing the burden of VPDs.[3] As Nigeria continues to make efforts to increase the routine immunisation (RI) coverage, great variation in the amount of progress still exists, not only between states, but even within states, local government areas (LGAs) and wards.[4,5] Two main issues have been identified as associated with poor RI service delivery: access, which is illustrated by antigen coverage, and utilisation, which is seen in the immunisation dropout rate.[6-8] In south-western Nigeria, where Ondo State is located, the issues of access to immunisation services have been addressed by strengthening the cultural belief of the people that immunisation, which is called ajesara in the local dialect, is highly protective against diseases. However, the issue of immunisation utilisation remains a major hurdle to be addressed, as shown from the high dropout rate.[9-12] Presently in Nigeria, immunisation programmes involve the use of the child health card as a tool for reminding caregivers of children of the dates of their next immunisation visit.[9-11] This has been reported to have several drawbacks, including the card being misplaced, or destroyed by unattended children and rodents. As a result of these drawbacks in the use of child health cards as a reminder tool for caregivers of children eligible for immunisation, vaccines have not been properly disseminated among children.[9-12]
Mobile phone technology may have great potential to address some basic issues and challenges related to under- or partial immunisation of children in Nigeria, thereby improving the completion rate of children's immunisation schedules.[13-15] It could achieve this through providing an avenue for parents to be reminded days prior to their children's next immunisation appointment by phone calls or SMS reminders, which could motivate them to take their children to the planned RI session.[13-15] Against this background, before any direct technological intervention is applied, there is a need to determine the feasibility of using this technological intervention to solve this problem, by identifying the proportion of ownership of mobile phones among caregivers, and the willingness to receive childhood immunisation schedule reminder messages among mothers of infants attending immunisation clinics.[13-15] Therefore, this study was conducted to determine mobile phone ownership among caregivers of children under the age of 1 year attending clinics conducting RI in Ondo State, and their knowledge of immunisation service delivery and willingness to receive immunisation schedule reminder messages.
Methods
Description of the study area
Ondo State is located in the south-western region of Nigeria, and covers a land area of 14 793 km2, and has its administrative capital at Akure.[16] The total population for Ondo State that was projected from the 2006 National Census is 4 358 987, while the population of children under the age of 1 year is 174 359. This is estimated based on the state's population making up 4% of the total population. The early settlers of Ondo State were the Yoruba people. The main ethnic groups in Ondo State are the Yoruba and Ijaw people. Ondo State inhabitants are mostly Christians, although a sizeable number of Muslims can be found in some parts of the state. Ondo State is made up of predominantly tropical rainforest, with some areas of forest savannah to its north, and forest and mangrove swamps in the south of the state. There are eighteen LGAs, grouped into three senatorial districts (Ondo Central, Ondo North and Ondo South) in the state.
The state, at the time of this study, had 554 health facilities offering RI, with trained and qualified healthcare workers conducting monthly planned RI activities. The immunisation unit of the state is responsible for ensuring that all children aged 0 - 11 months in the state are immunised against all childhood preventable diseases (tuberculosis, poliomyelitis, diphtheria, whooping cough (pertussis), hepatitis B, Haemophilus influenzae type B, tetanus, pneumonia, measles and yellow fever. The mobile networks in the state are MTN, Airtel, Glo Mobile, Etisalat, Visafone and Multilinks Telkom.
Data collection
This descriptive cross-sectional study was conducted in 24 public health facilities (in rural, semi urban and urban settlements), selected randomly by balloting from a list of health facilities in three LGAs in the three senatorial districts in Ondo State, Nigeria. Sample size was calculated for two outcome variables, which were ownership of mobile phones and willingness to receive immunisation reminder messages. Sample size was estimated using the standard formula for descriptive studies,[15,17] assuming a proportion of 0.77 of mothers willing to receive reminder messages. A sample size of 559 was obtained. The sample size was increased to 615 to make up for non-responses. All mothers of infants bringing their children to the 24 clinics conducting RI were enrolled consecutively until the sample size was attained. The inclusion criterion for the interview was being a mother of a child aged 0 - 11 months. Mothers who had a disability that precluded participation (e.g. cognitive impairment) were excluded from the study. At each site, data were collected from mothers by means of semi-structured interviewer-administered questionnaires, by the principal investigators and trained research assistants. During the interviews, mothers were asked for their demographic information, educational level, knowledge about immunisation, VPDs and vaccination schedules, sources of information about immunisation, ownership and use of mobile phones, willingness to receive immunisation reminder messages on their mobile phones and preferred languages and time for reminder messages.
Data management and statistical analysis
Data were analysed using SPSS version 20.0 (IBM Corp., USA). Knowledge on immunisation, VPDs and vaccination schedules was measured using 11 knowledge-based questions in the questionnaire. All appropriate responses were coded as 1, and wrong responses as 0. The total attainable score was 11 points. Percentage scores of <50%, 50 - 69% or >70% were categorised as poor, average and good knowledge, respectively. Descriptive statistics such as frequency counts, percentages, mean and SD were used. Proportions were reported for categorical variables, while mean and SD were reported for quantitative variables. The outcome variables of the study were ownership of mobile phones by mothers, and willingness to accept the mobile phone intervention for immunisation reminders, while the explanatory variables were sociodemographic characteristics, age of mothers in years, urban or rural location, level of education, ethnicity, mothers' occupation and husbands' occupation. Bivariate analysis using statistical tests and a logistic regression model were performed, with p values of <0.05 considered significant.
Ethical approval (ref. no. AD. 4693/194) was obtained from the Research Ethical Review Committee, Ministry of Health, Ondo State. Written informed consent was obtained from all participating mothers prior to administering the questionnaire, after the provision of adequate, clear and complete information about the study.
Results
A total of 615 questionnaires were valid for analysis. The age of the respondents ranged from 13 - 56 years, with a mean (SD) age of 28.5 (6.01) years. The majority of the participants (91.4%) were married and living with their spouse, and 80.8% had at least a secondary school education. About 50.1% resided in urban areas (Table 1). Forty-six percent of the respondents had good knowledge of immunisation, vaccine-preventable diseases and vaccination schedules, while 27.5% had poor knowledge (Table 2). The majority (86.0%) of the respondents owned a mobile phone, while 84.9% had registered phone numbers (Table 3).
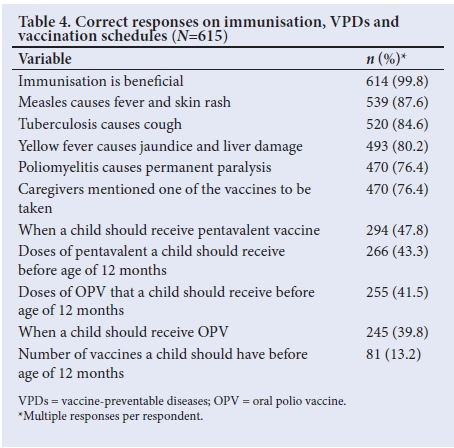
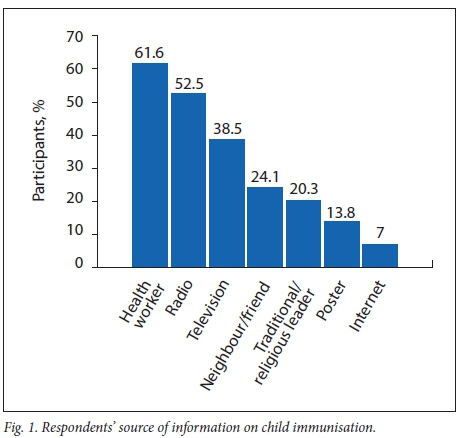
Almost all the caregivers (99.8%) responded that immunisation was beneficial to their children, although few (13.2%) knew the correct number of vaccines their children should take before the age of 12 months (Table 4). Over 61% of the respondents reported having heard about immunisation through health workers, while only 7% had heard about it through the internet (Fig. 1).
The majority of the participants were willing to receive reminder messages, with 71.7% preferring either a phone call or SMS, compared with 28.3% preferring both phone call and SMS. More than half of the participants (54.5%) would prefer messages to be sent in the English language, compared with 43.1% who would prefer the Yoruba language (Table 3).
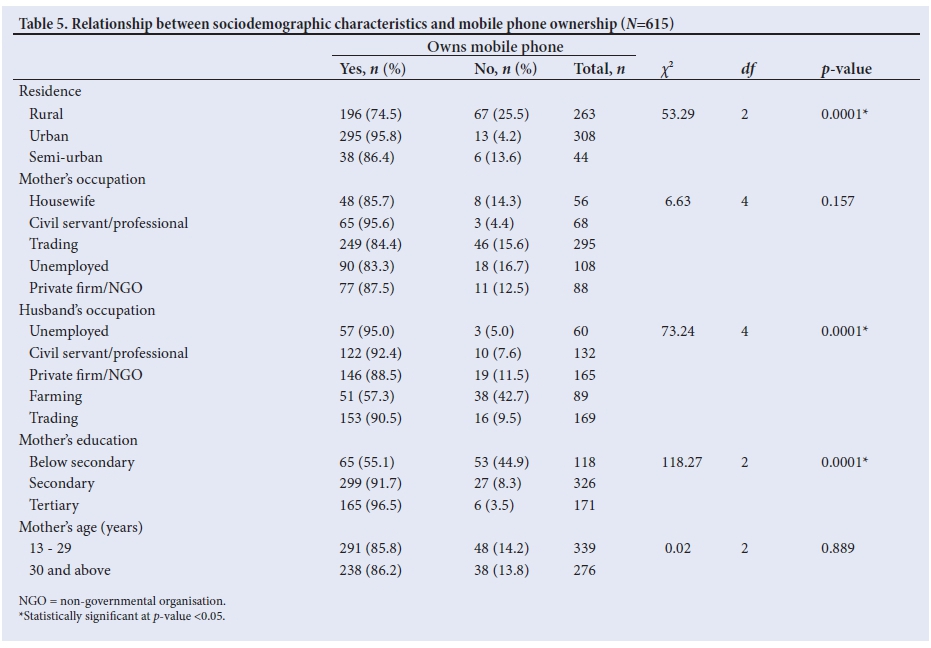
Bivariate analysis showed that there were statistically significant associations between area of residence, level of education and ownership of a mobile phone (Table 5).
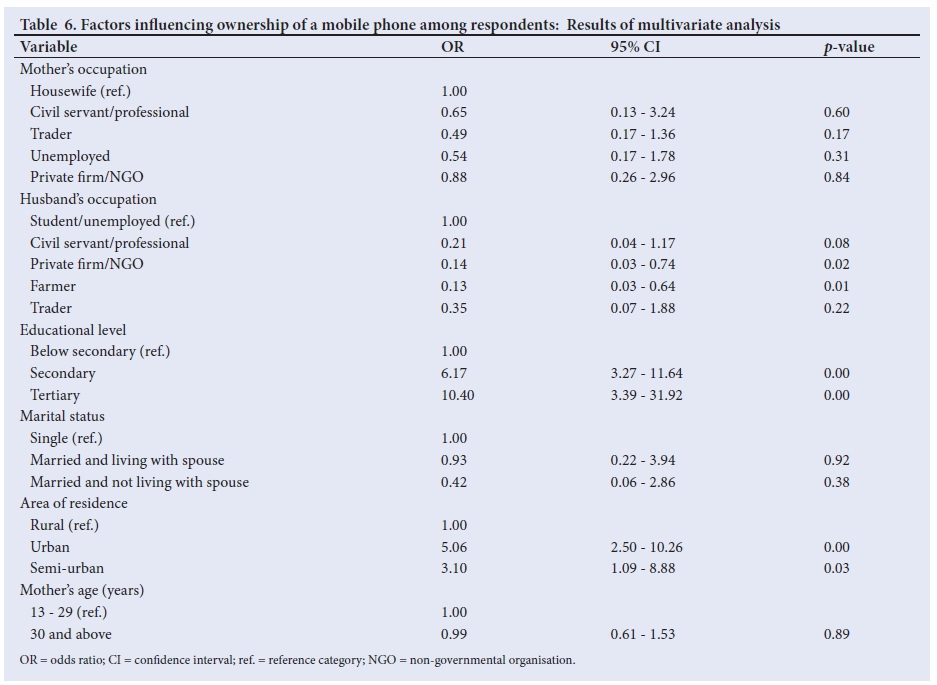
Table 6 shows the predictors of ownership of mobile phones. Respondents with a post-secondary education were 10 times more likely to own a mobile phone (odds ratio (OR) 10.40; 95% confidence interval (CI) 3.27 - 11.64) than those with below-secondary education only, while those who resided in urban areas were 5 times (OR 5.06, 95% CI 2.50 - 10.26) more likely to own a mobile phone than rural residents.
Discussion
The high proportion of respondents who owned a mobile phone in the study is very encouraging, and is comparable to a study conducted in Lagos, Nigeria, where 99% of respondents owned a mobile phone.[16] The proportion of mobile phone ownership in this study was probably not as high as that reported in Lagos, Nigeria, because that study was conducted in an urban setting, while this study was conducted in rural, semi-urban and urban settings.
Almost all respondents (99.8%) mentioned that immunisation was beneficial to their children.[18] This is consistent with results of a study conducted in Sabongidda-Ora, northern Nigeria, on determinants of vaccination coverage in rural Nigeria, which reported that almost all mothers (99.1%) felt that immunisation was beneficial to their children. The majority of the respondents in this study reported that the source of their information on immunisation was health workers.[19] This finding is similar to that of a study conducted on the uptake and behavioural and attitudinal determination of immunisation of hepatitis B among infants in a province outside of the Vancouver-Richmond health region, which showed that immunisation was significantly associated with recommendations from healthcare professionals. This finding also suggests a unique opportunity to positively influence the attitude of caregivers towards immunisation uptake through healthcare workers, as caregivers consider them the most important source of information on immunisation.[20] Health personnel should be mindful of this, because caregivers commonly comply with the information they receive at health facilities. Only 7.0% of respondents had heard about immunisation via the internet, suggesting that access to this technology is limited, which may be a result of the fact that many of the respondents are not computer literate.[21] This is in contrast to the findings of a study on the digital divide, titled 'Variation in internet and cellular phone use among women attending an urban sexually transmitted infections clinic, carried out in Baltimore, USA, where the prevalence of internet use was higher than expected, and significantly associated with higher educational attainment. This is understandable, as it was conducted in a developed country. In a lower-middle-income country such as Nigeria, the use of the internet varies, and is related to location. In this study we included women from rural, semi-urban and urban communities, and the state itself is an indigenous one, with information technology not as developed as in the metropolitan cities. The findings in this study also showed that knowledge increased with level of education.[22] This finding is similar to that of a study on mothers' knowledge, perception and practice of childhood immunisation in Enugu, Nigeria, which found that up to 90% of mothers in the study had at least a secondary education, which influenced their knowledge. A study on the knowledge, perception and beliefs of mothers on RI in a northern Nigerian village similarly reported that mothers with formal education were more likely to be aware of childhood immunisation than those who had no formal education.[23]
Another key finding in this study was that the majority of the respondents were willing to receive childhood immunisation reminder messages on their mobile phones. This is important, as the most common reason given for missing clinic appointments has been found to be that mothers forgot the dates of appointments.[15] This finding is consistent with that of a study conducted in Lagos, Nigeria, which showed that 77% of respondents were willing to receive SMS reminders about their child's immunisation schedule.[24] It is also consistent with a study in Kenya that showed that willingness to receive text message reminders was near-universal among the respondents (99.7%). This may be a result of the fact that mothers of infants would know when vaccinations were due, irrespective of the availability of their child health card.
Also, a key finding in this study was that a higher proportion of mothers were willing to receive immunisation reminder messages in English than in other languages, which corroborates the findings of a study conducted in Lagos, Nigeria, where 94% of respondents preferred English for reminders on their mobile phones,[24] and the findings of a similar study conducted in Kenya that found that mothers' preference for English language reminders could be attributed to their high literacy levels.[26] It was also found that most of the respondents would prefer a phone call reminder to an SMS.[27] This is also similar to a finding from a study conducted in the USA on parents' experiences and preferences for immunisation reminder or recall technologies, where the preferred mode was a phone call to the home telephone.[15] The findings of this study also corroborate those of a study in the African context, in Lagos, Nigeria, where 67% of respondents said they would prefer phone call reminders to SMS. This study also revealed that the preferred day to receive a reminder message is the day before the appointment.[15] This also corroborates the findings in Lagos, Nigeria, where 60% of the respondents would prefer a day before appointment reminder.
The findings presented in this study suggest that urban residence and maternal education make a mother more likely to own a mobile phone. This may be a result of the fact that educated mothers know the benefits of mobile phone technology, and can better afford the cost of a phone, compared with mothers with little or no formal education.'281 Similarly, in a study on mobile phone ownership and social integration in persons with spinal cord injuries (SCIs), which reported that out of 7 696 participants with traumatic SCIs surveyed, 73% owned a mobile phone, and people who had achieved education beyond grade school were more likely to own one. Also, mothers in urban residences are more likely to have access to a regular power supply than those in rural areas, which may encourage the use of mobile phones.
There are some limitations to this study, as only mothers of infants found in the health facilities during the researchers' visits were recruited for the study. It is possible that the inclusion of mothers of infants who were not present during the period of data collection would have had a significant impact on the study. In addition, the findings are applicable only to mothers attending public health facilities, while a significant proportion of mothers receive services in private health facilities. However, with the large number of mothers owning a mobile phone and their willingness to have reminder messages, it is possible that the findings from this study could be generalised.
Conclusion
The findings of this study are encouraging, as the majority of caregivers of children under the age of 1 year owned mobile phones and were willing to receive reminder messages. However, caregivers of infants in rural areas need to be provided with mobile phone support and trained in their usage, to benefit from such an intervention in childhood immunisation.
Acknowledgements. The authors would like to express their gratitude to the research assistants and caregivers who willingly participated in the study, the officers in charge of the 24 health facilities in the study, local immunisation officers of the three LGAs (Owo, Akure South and Ile-Oluji/Okeigbo), and Dr Akpa Matthew and Femi Alo for their immense contributions during data analysis.
Author contributions. OTA, AAF and EEI conceptualised the research idea, OTA designed and implemented the research, conducted the majority of participant interviews and performed data analysis and manuscript preparation. OTA, IOA and EEI contributed to the study design and manuscript review. IOA and BOY supervised the study design, implementation, data analysis and manuscript preparation.
Funding. The research was funded solely by the corresponding author, OTA.
Conflicts of interest. None.
References
1. Ubajaka FC, Ukegbu AU, Okafor NJ, Ejiofor O. The prevalence of missed opportunity for immunisation among children utilising immunisation services in Nnamdi Azikwe University Teaching Hospital, Nnewi. J Biol Agric Healthcare 2012;6(2):112-120. [ Links ]
2. United Nations Children's Fund. Maternal and Child Health. New York: UNICEF Statistics, 2012. http://www.unicef.org/Nigeria/children_1926_html (accessed 15 January 2012). [ Links ]
3. Menzies R, Turnour C, Chiu C, Mclntyre P. Vaccine preventable diseases and vaccination coverage in Aboriginal and Torres Strait Islander people, Australia, 2003 to 2006. Commun Dis Intell Q Rep 2008;32(Suppl):S2-S67. [ Links ]
4. Odusanya O, Ewan F, Meurice F, Ahonkhai V. Determinants of vaccination coverage in rural Nigeria. BMC Pub Health 2008;8(1):381. https://doi.org/10.1186/1471-2458-8-381 [ Links ]
5. National Immunisation Coverage Survey. Progress in immunisation, National and MNCH-PRRINN States performance. 2011. http://www.prrinnmnch.org/documents/Technical_brief_immunisation _progress_NICS_2010_review_ Feb11.pdf (accessed 15 January 2015). [ Links ]
6. Usman HR, Kristensen S, Rahbar H, Vermund SH, Habib F, Chamot E. Determinants of third dose of diphtheria-tetanus-pertussis (DPT) completion among children who received DPT 1 at rural immunisation centres in Pakistan: A cohort study. J Trop Med Int Health 2010;15(1):140-147. https://doi.org/10.1111/j.1365-3156.2009.02432.x [ Links ]
7. Usman HR, Rahbar MH, Kristensen S, et al. Randomized controlled trial to improve childhood immunisation adherence in rural Pakistan: Redesigned card and maternal education. J Trop Med Int Health 2011;16(3):334-342. https://doi.org/10.1111/j.1365-3156.2010.02698.x [ Links ]
8. Owais A, Hnif B, Siddiqui AR, Agha A, Zaidi A. Does improving maternal knowledge of vaccines impact immunisation rates? A community-based randomized-controlled trial in Karachi, Pakistan. BMC Pub Health 2011;11(1):239. https://doi.org/10.1186/1471-2458-11-239 [ Links ]
9. Ekure EN, Balogun MR, Mukhtar-Yola M, et al. Community knowledge, attitude and practice of childhood immunisation in Southwest Nigeria. Data from a Paediatric Association of Nigeria town hall meeting. Niger J Paed 2013;40(2):106-111. https://doi.org/10.4314/njp.v40i2,1 [ Links ]
10. Abdulraheem SI Onajole AT, Jimoh AA, Oladipo AR. Reasons for incomplete vaccination and factors for missed opportunities among rural Nigerian children. J Pub Health Epidemiol 2011;3(4):194-203. [ Links ]
11. Itimi K, Dienye PO, Ordinioha B. Community participation and childhood immunisation coverage: A comparative study of rural-urban communities of Bayelsa State, South-South Nigeria. Niger Med Journal 2012;53(1):21-25. https://doi.org/10.4103/0300-1652.99826 [ Links ]
12. Oladokun RE, Adedokun BO, Lawoyin TO. Children not receiving adequate immunisation in Ibadan, Nigeria: What reasons and beliefs do mothers have? BMC Pub Health 2010;13(2):173-178. [ Links ]
13. Carter MC, Burley VJ, Nykjaer C, Cade JE. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomised control trial. J Med Internet Res 2013;15(4):e32. https://doi.org/10.2196/jmir.2283 [ Links ]
14. Whittaker R, McRobbie H, Bullen C, Borland R, Rodgers A, Gu V. Mobile phone-based intervention for smoking cessation. 2016;10(4):CD006611. https://doi.org/10.1002/14651858.CD006611.pub4 [ Links ]
15. Balogun MR, Sekoni AO, Okafor IP, et al. Access to information technology and willingness to receive text messages reminders for childhood immunisation among mothers attending a tertiary facility in Lagos, Nigeria. S Afr J Child Health 2012;6(3):76-80. https://doi.org/10.7196/SAJCH.439 [ Links ]
16. National Population Commission, Population and Development Review. Abuja: National Population Commission; 2007;33(1):206-210. [ Links ]
17. Kish, L. Survey Sampling. New York: John Wiley, 1965: 78-94. [ Links ]
18. Odusanya O, Alufohai EF, Meurice F, Ahonkhai V. Determinants of vaccination coverage in rural Nigeria. BMC Pub Health 2008;8(1):381. https://doi.org/10.1186/1471-2458-8-381 [ Links ]
19. Big bam M, et al. Uptake, behavioural and attitudinal determinants of immunisation of Hepatitis B among infants. Ninth International Congress of Behavioural Medicine, Thailand, 2006. [ Links ]
20. Mapotamo MA, Kayembe K, Piripin L, Nyadwe K. Immunisation - related knowledge, attitudes and practices of mothers in Kinshasa, Democratic Republic of Congo. S Afr Fam Pract 2008;50(2):61-61e. [ Links ]
21. Samal L, Hutton H, Erbelding E, Brandon E, Finkelsstein J, Chander G. Digital divide: Variation in internet and cellular phone use among women attending an urban sexually transmitted infections clinic. J Urban Health 2010;87(1):122-128. https://doi.org/10.1007/s11524-009-9415-y [ Links ]
22. Tagbon BN, Uleanya ND, Nwokoye IC, Eze JC, Omotowo IB. Mothers' knowledge, perception and practice of childhood immunisation in Enugu. Niger J Paediatr 2012;39(3):90-96. https://doi.org/10.4314/njp.v39i3.1 [ Links ]
23. Kebir M, Liyazu Z, Abubakar IS, Gayida AU. Perception and beliefs of mothers on routine childhood immunisation in a Northern Nigeria village. Ann Nigerian Med 2005;1(1):21-26. [ Links ]
24. Gabriel O, Sophic G, Caroline J, Robert W, Abrose T, Dejan Z. The feasibility, patterns of use and acceptability of using mobile phone text messaging to improve treatment adherence and post treatment review of children with uncomplicated malaria in western Kenya. Malaria J 2014;13(1):44. https://doi.org/10.1186/1475-2875-13-44 [ Links ]
25. Ahlers-Schmidt CR, Chesser A, Hart, T, Pascal A, Nguyen T, Wittler RR. Text messaging immunisation reminders: Feasibility of implementation with low-income parents. Prev Med 2010;50(5-6):306-307. https://doi.org/10.1016/j.ypmed.2010.02.008 [ Links ]
26. Kharbanda EO, Stockwell MS, Fox HW, Rickert VI. Text4Health: A qualitative evaluation of parental readiness for text message immunisation reminders. Am J Pub Health 2009;99(12):2176-2178. https://doi.org/10.2105/AJPH.2009.161364 [ Links ]
27. Clark SJ, Butchart A, Kennedy A, Dombkowsy KJ. Parents' experiences and preferences for immunisation reminder/recall technologies. Pediatrics 2011;128(5):1100-1105. https://doi.org/10.1542/peds.2011-0270 [ Links ]
28. Roach MJ, Harrington A, Powell H, Nemunaitis G. Cell telephone ownership and social integration in persons with spinal cord injury. Arch Phys Med Rehabil 2011;92(3):472-476. https://doi.org/10.1016/j.apmr.2010.09.030 [ Links ]
 Correspondence:
Correspondence:
O T Akinrinade
omotola.akinrinade@yahoo.co.uk
Accepted 2 March 2018


{kind=link}
{kind=link}