










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.12 n.3 Pretoria Jul./Sep. 2018
http://dx.doi.org/10.7196/sajch.2018.v12i3.1469
ARTICLE
Acceptance of an orange-fleshed sweet potato complementary food by infant caregivers in KwaZulu-Natal Province - a preliminary study
K PillayI; N KhanyileII; M SiwelaI
IPhD; Department of Dietetics and Human Nutrition, College of Agriculture, Engineering and Science, University of KwaZulu-Natal, Pietermaritzburg, South Africa
IIMSc (Diet); Department of Dietetics and Human Nutrition, College of Agriculture, Engineering and Science, University of KwaZulu-Natal, Pietermaritzburg, South Africa
ABSTRACT
BACKGROUND. Vitamin A deficiency (VAD) is a major public health problem that affects South African children and is a major contributor to the mortality of children under five years of age. VAD can result in visual impairment, diarrhoea and increased risk of severe measles and death. Orange-fleshed sweet potato (OFSP), a staple crop biofortified with provitamin A, has the potential to improve vitamin A intake in infants, especially when used as a complementary food.
OBJECTIVE. To assess the acceptance of an OFSP complementary food by infant caregivers.
METHODS. This study was conducted at the Newtown Community Health Centre, Inanda, in the eThekwini District of KwaZulu-Natal (KZN). Sixty-three infant caregivers assessed the acceptance of complementary foods made from OFSP and white-fleshed sweet potato (WFSP) (control), using a five-point hedonic rating test. In addition, ten caregivers participated in two focus group discussions, using pre-determined questions.
RESULTS. There were no statistically significant differences in the sensory attribute ratings of complementary foods made from WFSP and OFSP. The OFSP complementary food was well-accepted, especially its colour and soft texture. None of the focus group discussion participants had seen or tasted the OFSP before. Caregivers were willing to buy the OFSP, if it were available and cheaper than the WFSP.
CONCLUSION. The complementary food made from the OFSP was highly acceptable to infant caregivers attending the Newtown Community Health Centre in KZN. It has the potential to be used in complementary feeding and to improve the vitamin A status of infants.
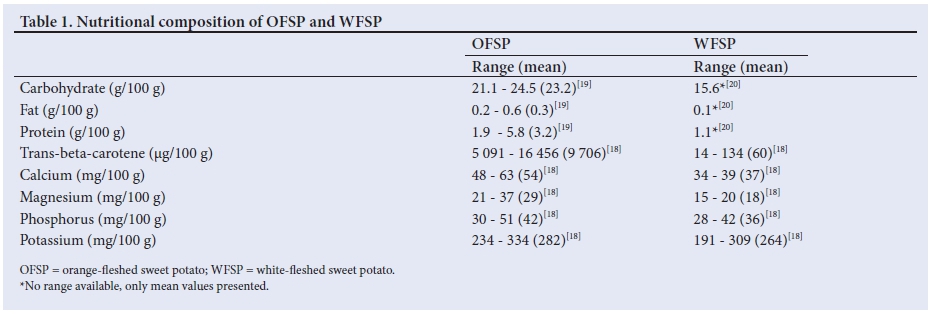
Vitamin A deficiency (VAD) is a major public health problem in lower-income countries [1] and it affects 250 million preschool children worldwide.[2] In South Africa (SA), the South African National Health and Nutrition Examination Survey (SANHANES-1) reported that 43.6% of under-5 children had VAD.[3] This was significantly higher than the national VAD prevalence of 33%, which was reported by the SAVACG study in 1994.[4] KwaZulu-Natal (KZN) Province of SA was found to have the highest number of children with VAD (56.4%) in 2005.[5] Despite the implementation of various strategies to address VAD in SA, including commercial food fortification, vitamin A supplementation and dietary diversification, VAD continues to be a problem.[6] Biofortification provides another strategy for dealing with nutrient deficiencies, especially micronutrient malnutrition, and it involves improving the vitamin and mineral levels in a crop through plant breeding, transgenic techniques or agronomic practices. Biofortified staple crops have the potential to improve human health and nutrition, if consumed on a regular basis.[7] Vulnerable rural populations, with poor access to diverse diets, supplementation and commercially-fortified foods, could access biofortified staple crops through biofortification programmes.[8] Orange-fleshed sweet potato (OFSP) is a staple crop that is high in beta-carotene, a provitamin A carotenoid,[9] and it is one of six staple crops in the HarvestPlus Crop Biofortification Program that is being widely promoted in developing countries.[10,11] The South African Agricultural Research Council (ARC) and Medical Research Council (MRC) are involved in leading research and in promoting the use of the beta-carotene-rich sweet potato, as a crop-based approach for addressing VAD.[12-14] The ARC has been involved in developing improved varieties of the OFSP.[15,16] Sweet potato has a much higher carbohydrate content (26.3 g/100 g) than other foods, such as maize porridge (15.6 g/100 g), sorghum porridge (17.0 g/100 g) and potatoes (18.5 g/100 g);[17] however, the protein content is lower than in potatoes and other grain crops.[17] The nutritional composition of the OFSP and the WFSP is shown in Table 1. A study by Laurie et al.[18] found that almost 96% of the total beta-carotene in OFSP was in the trans configuration, which provides an additional benefit when addressing VAD, as the trans isomer has more than double the provitamin A activity compared with the cis isomer.[18] Apart from its nutritional value, the sweet potato is also known for its high yield, its hardiness, its low demand on soil nutrients and cultivation input, as well as its storability and versatility in processing.[17]
A study conducted in KZN found that regular consumption of the Resisto variety of the sweet potato, containing a mean (standard deviation (SD)) beta-carotene amount of 9 980 (1 167) |ig per 100 g cooked sweet potato, led to an improvement in the vitamin A status of primary school children.[21] The introduction of OFSP to the diet of young children in rural Mozambique increased the concentration of serum retinol in the intervention group.[22] The consumption of OFSP was also found to reduce the prevalence and duration of diarrhoea in children.[23] Given the reported benefits of feeding OFSP to children,[21-23] it may also be beneficial in complementary feeding. Complementary feeding refers to the introduction of solid foods at six months, when breastmilk alone is no longer able to meet the nutritional requirements of an infant.[26] The introduction of inappropriate foods, as well as an inadequate dietary intake during the complementary feeding stage, can increase the risk of malnutrition.[25,26] The intake of vitamin A-rich vegetables and fruits in SA is lowest in the 6- to 9-month age group (the complementary feeding stage) and only 18% of children consume vitamin A-rich fruit and vegetables.[27] OFSP-based complementary foods have been found to be a better source of vitamin A than those that are maize-and legume-based.[28] As is the case in other parts of SA, OFSP is not commonly used in KZN where consumers are accustomed to white-fleshed sweet potato (WFSP). The adoption of OFSP for use in complementary foods depends on, among other factors, their acceptability to the infant caregivers, as they usually decide which type of complementary food to feed the infants in their care. There are no published findings on the acceptance of complementary foods containing OFSP by caregivers. This study, therefore, aimed to determine whether the caregivers of infants attending the Newtown Community Health Centre in Inanda, in the eThekwini District of KZN, would accept a complementary food made from OFSP, and what their perceptions of this complementary food would be.
Methods
Preparation of complementary food samples
In this study, WFSP was used as the control. Both the OFSP and WFSP used in this study were sourced from a local fruit and vegetable store. Mashed sweet potato was chosen for use in this study, as it is a popular complementary food. An adult woman from rural KZN, who has experience in preparing complementary foods, was asked to do so for the current study. Both the WFSPs and OFSPs were boiled in water, with their skins on, for about 30 minutes, until they were soft. Thereafter, the skin was removed and the sweet potatoes were mashed until the mixture was soft and smooth. No seasoning was added to the samples. The samples were prepared and transported in containers, with tight-fitting lids, to the Newtown Community Health Centre on the day of data collection.
Sensory evaluation
A pilot study of the sensory evaluation and the focus group discussion was conducted on the same day, prior to the main study. Ten caregivers attending the Paediatric Outpatients Department (POPD) at the Newtown Community Health Centre at Inanda, in the eThekwini District of KZN, voluntarily participated in a sensory evaluation pilot study. A short while later, five of the caregivers who had participated in the sensory evaluation, were randomly selected to participate in a pilot focus group discussion. The aim of the pilot study was to test the sensory evaluation questionnaire and the procedures for conducting the sensory evaluation and the focus group discussion. The pilot study was conducted on a different day to the main study, in order to prevent the participants from participating in the main study. As the caregivers were not available to participate in the sensory evaluation session after their consultations at the POPD, it was decided that they should be conducted early in the morning. As the pilot study venue was too far away from the POPD, a closer alternative venue was used for the main study. No changes were made to the sensory evaluation questionnaire after the pilot study.
Sixty-three caregivers, who cared for children aged 8 - 24 months at the time of the study, participated voluntarily in the main sensory evaluation study. This study was conducted in a designated private room, close to the POPD. The caregivers were seated a distance away from each other and were asked not to communicate with each other during the sensory evaluation session. The samples were randomly labelled, using a unique three-digit code obtained from a table of random numbers, and they were served in a random order.[29] The samples were warmed in a microwave oven for 10 seconds, at a medium heat, before serving. Each caregiver received 30 ml samples of WFSP and OFSP in separate polystyrene cups. The caregivers were provided with a spoon and a cup of water to rinse their palates between samples. A sensory evaluation questionnaire, which used a five-point facial hedonic scale (1 = very bad to 5 = very good), was developed in isiZulu, and a research assistant explained it to the caregivers in isiZulu. The caregivers rated the taste, texture, aroma, colour and overall acceptability of both the WFSP (control) and the OFSP samples. Research assistants assisted the caregivers, when necessary.
Focus group discussions
Focus group discussions were conducted about 30 minutes after the sensory evaluation study was completed. The 63 caregivers who participated in the sensory evaluation were randomly allocated a number between 1 and 63. Ten numbers were randomly selected, using a table of random numbers, and the corresponding caregivers were invited to participate in the focus group discussions. The 10 caregivers were further divided into 2 groups, 1 with 6 participants, and the other with 4 participants. A trained facilitator directed the discussions, using a structured discussion guide. The focus group discussion guide consisted of a brief explanation of the samples that were tasted during the sensory evaluation as well as a set of questions for initiating and facilitating the discussion. The questions for the caregivers included the following: Have you ever heard of, seen or tasted OFSP before? What is your perception of the taste, smell, colour and texture of the OFSP complementary food? Is the OFSP different to the WFSP, and if so, how is it different? Would you feed OFSP to children in your care? And would you consider adding any other foods to the OFSP? The discussions were facilitated in isiZulu and were recorded using a digital voice recorder, while a scribe took notes of the discussion. During the focus group discussions, the facilitator also made a note of the nonverbal communication, gestures and behavioural responses of the participants. These were used to supplement the discussion transcripts.
Data analysis
Sensory evaluation data were analysed by using the Statistical Package for Social Sciences (SPSS) Version 15 (SPSS Inc., USA).
The means and standard deviations (SD) were calculated. The oneway Analysis of Variance (ANOVA) and Dunnett's test were used to analyse the data. A p-value <0.05 was considered to be significant. A verbatim transcript of the focus group discussions was translated into English by the focus group discussion facilitator. Another isiZulu-speaking person checked the accuracy of the English translation, by comparing it to the isiZulu recordings and the notes of the scribe. The researcher analysed the focus group discussions, using the four stages of content analysis. During the first stage of decontexualisation, the researcher read the transcribed text, which was then broken down into smaller meaning units, which were labeled with a code. A coding list was developed to explain the codes. In the second stage of recontextualisation, the original text was read again, together with the final list of meaning units. Coloured pens were used to identify each meaning unit in the original transcript. During the third stage of categorisation, the themes and categories were identified, and in the fourth stage, the researcher selected verbatim quotations for each theme.
Ethics approval
Ethical approval was obtained from the University of KwaZulu-Natal (UKZN), Humanities and Social Sciences Ethics Committee (ref. no. HSS/0486/015M). The KZN Department of Health (ref no. HRKM180/15) and the medical manager of the Newtown Community Health Centre also approved the study. All caregivers gave their written consent prior to participating in the sensory evaluation and the focus group discussion. In addition, focus group participants gave their written consent for the voice recording.
Results
Sensory evaluation
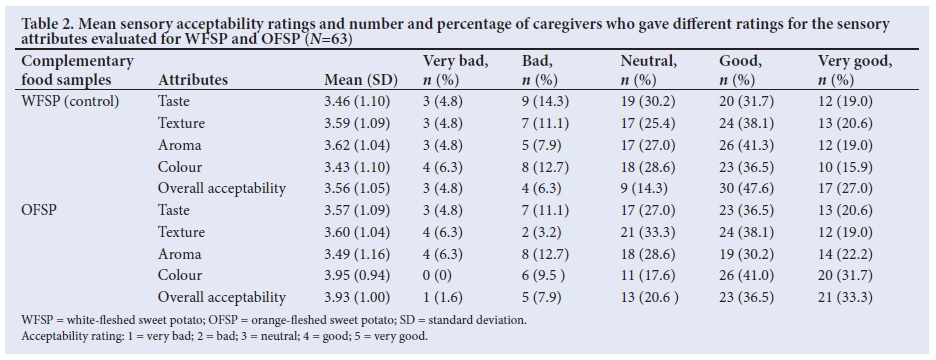
Table 2 shows the mean sensory acceptability ratings for the WFSP and OFSP, according to the different sensory attributes and the number and percentage of caregivers who gave the different ratings for the sensory attributes for both samples. The OFSP scored higher for taste (3.57), texture (3.60), colour (3.95) and overall acceptability (3.93). However, the WFSP scored higher for aroma (3.62). There were no statistically significant differences between the mean sensory acceptability scores for the WFSP and OFSP. Thirteen caregivers (20.6%) rated the taste of OFSP as 'very good, compared with 12 (19.0%) for the WFSP. Twenty (31.7%) of the caregivers rated the colour of the OFSP as 'very good', compared with 10 (15.9%) for the WFSP. The overall acceptability of the OFSP was rated as 'very good' by 21 (33.3%) of the caregivers, while 17 (27.0%) gave the same rating for the WFSP.
Focus group discussions
All participants in the focus group discussions indicated that they had not seen or tasted OFSP before.
'I thought this was butternut. If you had not said this is sweet potato,
I wouldn't have known that this is sweet potato.'
Some of them thought that the OFSP was pumpkin or butternut. They were also interested in finding out where they could buy it. The softness and colour of the OFSP appealed to the caregivers. They had the perception that children would also accept it.
'The colour of the OFSP is good for the kids since it is bright and kids like colourful things.'
The caregivers likened the texture of the OFSP to commercial baby food products and perceived it to be ideal for children, compared with the WFSP, which they perceived to be drier.
'Its texture, the softness. If you compare this to Purity, they are the same. The white one is okay for adults but this would be best for kids.' 'The orange one is very soft which is good for the kids since they will not choke while eating it as kids choke very easily, the white one is more suitable for adults.'
The caregivers expressed a desire to purchase OFSP, instead of WFSP, if the prices were comparable, and if they were cheaper.
'I will buy it if was equal or less expensive than the white one.'
'I will choose the orange one over the white one if they were both in
the shops and I had to choose one for my child.'
Discussion
VAD in children remains a major problem worldwide.[2] It is associated with reduced resistance to common childhood infections, such as respiratory and diarrhoeal diseases, measles and malaria.[30] OFSP is a provitamin A-rich crop that is promoted to address VAD in developing countries.[18] The South African ARC promotes the use of OFSP by means of agricultural training, nutrition education, and by establishing community-based nurseries, and it focuses on the consumption of unprocessed, boiled roots to address vitamin A deficiency.[31] Interventions promoting the production of OFSP, particularly the Bophelo variety, have been implemented in certain areas of the North-west Province, Gauteng, Mpumalanga, the Limpopo Province, the Eastern Cape and Umkhanyakude, as well as in Zululand in KZN.[31] Although WFSPs are commonly used in complementary feeding and are commercially available, they are devoid of provitamin A and cannot contribute to vitamin A intake. Therefore, this study aimed to determine whether the caregivers of infants would accept a complementary food made from OFSP, a rich source of provitamin A and, particularly, beta-carotene.
The results of this study indicated that the sensory attributes of the complementary food made from OFSP were acceptable to the infant caregivers who evaluated it. This is in keeping with findings of a Ugandan study, which found that baby-weaning food made from OFSP was more acceptable to children and mothers than the traditional maize weaning porridge.[32] A study conducted using Ugandan famers found a definite preference for OFSP-based complementary foods over WFSP,[33] while other studies also found a preference for OFSP over WFSP.[34-36] Other products in SA, such as juice, chips and doughnuts made from beta-carotene-rich sweet potatoes, have also been found to be acceptable among consumers.[37] These products have also been promoted with the implementation of vegetable gardens emphasising the production of beta-carotene-rich sweet potato, in various sites throughout SA.[12] Orange-fleshed sweet potatoes have the potential to meet the daily vitamin A requirements of children. The Bophelo variety of the OFSP, which is promoted by the ARC in SA, contains 6 708 |ig beta-carotene/100 g, and a 67 g portion is sufficient to meet the vitamin A requirements of children between 12 and 36 months.[31]
The production of OFSP in areas with a high prevalence of VAD should be promoted. This crop can be produced and made available all year round in the tropical and subtropical areas of SA, including the drought-prone areas.[38] Sweet potato, including OFSP, is drought tolerant and has a greater yield potential than other SA staple crops, including maize.[38] The fact that none of the focus group participants had ever seen or tasted OFSP prior to the current study indicates that there is a need to raise awareness about it and to increase its availability in KZN. Nutrition education, highlighting the nutritional benefits of the OFSP, as well as its improved availability on the market, may lead to an improvement in its consumption. Communities that receive both production training and nutrition education on the OFSP are more likely to grow and use it.[39] This study was limited, in that it was only conducted at one site in KZN. Future studies should include more areas in KZN and the rest of SA, especially in the rural areas, where VAD is more prevalent.
Conclusion
A complementary food made from OFSP was acceptable to the infant caregivers who tasted it. There was a willingness to purchase OFSP, instead of WFSP, if the price was comparable and cheaper than that of WFSP. The findings suggest that the OFSP has the potential to be used in complementary feeding and to improve vitamin A intake in infants, a group that is vulnerable to VAD.
Acknowledgements. The authors thank the caregivers who consented to participate in the study.
Author contributions. KP and MS designed the study and developed the methodology. NK collected and analysed the data. KP prepared the manuscript with input from NK and MS. The final manuscript was reviewed and edited by KP. This study was supervised by KP and MS and submitted by NK to the University of KwaZulu-Natal (UKZN) in fulfilment of an MSc in Dietetics.
Funding. Funding was received from the College of Agriculture, Engineering and Science, UKZN.
Conflicts of interest. None.
References
1. World Health Organization (WHO). Global prevalence of vitamin A deficiency in populations at risk 1995 - 2005: WHO global database on vitamin A deficiency. Geneva: WHO, 2009. http://whqlibdoc.who.int/publications/2009/9789241598019_eng.pdf (accessed 25 August 2017). [ Links ]
2. World Health Organization (WHO). Micronutrient deficiencies: Vitamin A deficiency. Geneva: WHO, 2010. [ Links ]
3. Shisana O, Labadarios D, Rehle T, et al. South African National Health and Nutrition Examination Survey (SANHANES-1). Cape Town: HSRC Press, 2013. http://www.hsrc.ac.za/uploads/pageNews/72/SANHANES-launch%20edition%20(online%20version).pdf (accessed 29 August 2017). [ Links ]
4. South African Vitamin A Consultative Group. Anthropometric, vitamin A, iron and immunisation coverage status in children aged 6-71 months in South Africa, 1994. S Afr Med J 1996;86:354-357. [ Links ]
5. Labadarios D, Swart R, Maunder EMW, et al. Executive summary of the National Food Consumption Survey-fortification baseline (NFCS-FB-1), South Africa, 2005. S Afr J Clin Nutr 2008; 21(Suppl 2):245-300. [ Links ]
6. Labadarios D, Steyn NP, Mgijima C, Dladla N. Review of the South African nutrition policy 1994-2002 and targets for 2007: Achievements and challenges. Nutrition 2005;21:100-108. https://doi.org/10.1016/j.nut.2004.09.014 [ Links ]
7. Bouis HE, Saltzman A. Improving nutrition through biofortification: A review of evidence from HarvestPlus, 2003 through 2016. Glob Food Sec 2017;12:49-58. https://doi.org/10.1016Zj.gfs.2017.01.009 [ Links ]
8. Saltzman A, Birol E, Bouis HE, et al. Biofortification: Progress towards a more nourishing future. Glob Food Sec 2013;2:9-17. https://doi.org/10.1016/j.gfs.2012.12.003 [ Links ]
9. Takahata Y, Noda T, Nagata T. HPLC determination of β-carotene content of sweet potato cultivars and its relationship with colour values. Japan J Breed 1993;43:421-427. https://doi.org/10.1270/jsbbs1951.43.421 [ Links ]
10. Nestel P, Bouis HE, Meenakshi JV, Pfeiffer W. Biofortification of staple food crops. Symposium: Food fortification in developing countries. J Nutr 2006;136:1064-1067. [ Links ]
11. Pfeiffer WH, McClafferty B. HarvestPlus: breeding crops for better nutrition. Crop Sci 2007; 47:S88-S105. https://doi.org/10.2135/cropsci2007.09.0020ipbs [ Links ]
12. Faber M, Phungula MAS, Venter SL, Dhansay MA, Benade AJS. Home gardening focusing on the production of yellow and dark-green leafy vegetables increase the serum retinol concentrations of 2 - 5-y-old children in South Africa. Am J Clin Nutr 2002; 76:1048-1054. https://doi.org/10.1093/ajcn/76.5.1048 [ Links ]
13. Laurie SM, Faber M. Integrated community-based growth monitoring and vegetable gardens focusing on crops rich in β-carotene - project evaluation in a rural community in the Eastern Cape, South Africa. J Sci Food Agric 2008;88:2093-2101. https://doi.org/10.1002/jsfa.3319 [ Links ]
14. Laurie SM, Mtileni MM, Mphaphuli NS, Tjale SS, Domola MJ. Experiences with orange-fleshed sweetpotato in vegetable garden projects. Proceedings: Orange-fleshed sweetpotato symposium. 2008. Pretoria, 3 October 2007. MRC/ ARC Cape Town, South Africa. [ Links ]
15. Laurie SM, Van den Berg AA, Magoro MD, Kgonyane MC. Breeding of sweetpotato and evaluation of advanced breeding lines and imported varieties in off-station trials in South Africa. Afr J Crop Sci J 2004;2(3):189-196. https://doi.org/10.4314/acsj.v12i3.27877 [ Links ]
16. Laurie SM, van den Berg AA, Tjale SS, Mulandana NS, Mtileni MM. Initiation and first results of a biofortification program for sweet potato in South Africa. J Crop Improvement 2009;23(3):235-251. https://doi.org/10.1080/15427520902774298 [ Links ]
17. Woolfe J. Sweet potato an untapped food resource. Cambridge: Cambridge University Press, 1992;5:122-124. [ Links ]
18. Laurie SM, van Jaarsveld PJ, Faber M, Labuschagne MT. Trans-|3-carotene, selected mineral content and potential nutritional contribution of 12 sweetpotato varieties. J Food Compos Anal 2012;27:151-159. https://doi.org/10.1016/j.jfca.2012.05.005 [ Links ]
19. Alam MK, Rana ZH, Islam SN. Comparison of the proximate composition, total carotenoids and total polyphenol content of nine orange-fleshed sweet potato varieties grown in Bangladesh. Foods 2016;5(3):64. https://doi.org/10.3390/foods5030064 [ Links ]
20. Wolmarans P, Danster N, Dalton A, Rossouw K, Schonfeldt H. Condensed Food Composition Tables for South Africa. Parow: Medical Research Council, 2010. [ Links ]
21. Van Jaarsveld PJ, Faber M, Tanumihardjo SA, Nestel P, Lombard CJ, Benade AJS. B-carotene-rich orange-fleshed sweet potato improves the vitamin A status of primary school children assessed with the modified-relative-dose-response test. Am J Clin Nutr 2005;81:1080-1087. https://doi.org/10.1093/ajcn/8L5.1080 [ Links ]
22. Low JW, Arimond M, Osman N, Cunguara B, Zano F, Tschirley D. A food-based approach introducing orange-fleshed sweet potatoes increased vitamin A intake and serum retinol concentrations in young children in rural Mozambique. J Nutr 2007;137(5):1320-1327. https://doi.org/10.1093/jn/137.5.1320 [ Links ]
23. Jones KM, de Brauw A. Using agriculture to improve child health: Promoting orange sweet potatoes reduces diarrhea. World Dev 2015;74:15-24. https://doi.org/10.1016/j.worlddev.2015.04.007 [ Links ]
24. World Health Organization (WHO). Complementary feeding. Geneva: WHO, 2012. http://who.int/nutrition/topics/complementary_feeding/en/ (accessed 25 August 2017). [ Links ]
25. Faber M, Wenhold F. Nutrition in contemporary South Africa. Water SA 2007;33:S393-S400. https://doi.org/10.4314/wsa.v33i3.49122 [ Links ]
26. Faber M, Benade AJ. Breastfeeding, complementary feeding and nutritional status of 6-12-months-old infants in rural KwaZulu-Natal. S Afr J Clin Nutr 2007;20(1):16-24. https://doi.org/10.1080/16070658.2007.11734118 [ Links ]
27. Faber M. Complementary foods consumed by 6 - 12-month-old rural infants in South Africa are inadequate in micronutrients. Public Health Nutr 2005;8(4):373-381. https://doi.org/10.1079/phn2004685 [ Links ]
28. Amagloh FK, Coad J. Orange-fleshed sweet potato-based infant food is a better source of dietary vitamin A than a maize-legume blend as complementary food. Food Nutr Bull 2013;35(1):51-59. https://doi.org/10.1177/156482651403500107 [ Links ]
29. Heymann H. Three-day Advanced Sensory Analysis Workshop. Pretoria: Agricultural Research Council, 1995. [ Links ]
30. Rice AL, West Jr KP, Black RE. Vitamin A deficiency. In: Ezzati M, Lopez AD, Rodgers A, Murray CJL, eds. Comparative Quantification of Health Risks. Global and Regional Burden of Disease Attributable to Selected Major Risk Factors. Geneva: WHO, 2004. [ Links ]
31. Laurie SM. A crop-based approach focused on orange-fleshed sweet potato as means to address vitamin A deficiency. ARC vegetable and Ornamental Plants. Media Statement, 25 October 2017. http://www.arc.agric.za/Agricultural%20Sector%20News/Orange%20fleshe d°/o20sweet°/o20potato.pdf [ Links ]
32. Tumwegamire S, Kapinga R, Zhang D, Crisman C, Agilli S. Opportunities for promoting orange-fleshed sweetpotato among food based approach to combat vitamin A deficiency in sub-Saharan Africa. Afr Crop Sci J 2004;12(3):241-253. https://doi.org/10.4314/acsj.v12i3.27884 [ Links ]
33. Ssebuliba JM, Muyonga JH, Ekere W. Performance and acceptability of orange fleshed sweetpotato cultivars in Eastern Uganda. Afr Crop Sci J 2006;14(3):231-240. [ Links ]
34. Tomlins K, Ndunguru G, Stambul K, et al. Sensory evaluation and consumer acceptability of pale-fleshed and orange-fleshed sweetpotato by school children and mothers with preschool children. J Sci Food Agric 2007; 87(13):2436-2446. https://doi.org/10.1002/jsfa.2931 [ Links ]
35. Leksrisompong M, Whitson N, Truong V, Drake M. Sensory attributes and consumer acceptance of sweet potato cultivars with varying flesh colours. J Sens Stud 2012;27:59-69. https://doi.org/10.1111/j.1745-459x.2011.00367.x [ Links ]
36. Omodamiro RM, Afuape SO, Njoku CJ, Nwankwo IIM, Echendu TNC, Edward TC. Acceptability and proximate composition of some sweet potato genotypes: Implication of breeding for food security and industrial quality. Int J Biotechnol Food Sci 2013;1(5):97-101. [ Links ]
37. Laurie SM, Van Heerden SM. Consumer acceptability of four products made from beta-carotene-rich sweet potato. Afr J Food Sci 2012;6(4):96-103. https://doi.org/10.5897/AJFS12.014 [ Links ]
38. Motsa NM, Modi AT, Mabhaudhi T. Sweet potato (Ipomoea batatas L.) as a drought tolerant and food security crop. S Afr J Sci 2015;111(11/12):1-8. https://doi.org/10.17159/sajs.2015/20140252 [ Links ]
39. Nabugoomu J, Namutebi A, Kaaya AN, Nasinyama G. Nutrition education influences vitamin A-related knowledge, attitudes, and practices of child caregivers towards the production of orange-fleshed sweet potato in Uganda. J Food Nutr Sci 2015;3(2):38-47. https://doi.org/10.11648/j.jfns.20150302.13 [ Links ]
 Correspondence:
Correspondence:
K Pillay
pillayk@ukzn.ac.za
Accepted 23 April 2018


{kind=link}
{kind=link}