








Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.12 n.2 Pretoria Apr./Jun. 2018
http://dx.doi.org/10.7196/sajch.2018.v12i2.1458
RESEARCH
The use of the Road-to-Health card by doctors in a tertiary paediatric hospital setting
J I WilesI; G H SwinglerII
IMB ChB, DCH, FCPaed, MMed; Department of Paediatrics, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa
IIMB ChB, FCPaed, PhD Department of Paediatrics, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa
ABSTRACT
BACKGROUND. Low possession of the Road-to-Health card (RTHC) by parents, as well as inadequate use of the RTHC by health professionals, have reduced its efficacy.
OBJECTIVES. To describe the level of possession of the RTHC by a sample of patients admitted to the Red Cross War Memorial Children's Hospital (RCWMCH), and to determine the extent and accuracy of doctors' transfer of clinical information between the RTHC and hospital records.
METHODS. A cross-sectional analytical study conducted in four general paediatric wards over six weeks, during which data were extracted from participants' RTHC and hospital record. The presence or absence of selected items of information on the RTHC and the hospital record was recorded; the primary outcome was the transfer of the specified items of information between records.
RESULTS. A total of 133 (81%) eligible caregivers had the RTHC on their person. Variables including perinatal information, immunisation record and weight-for-age chart were well-documented on the RTHC prior to hospital admission, and mostly well-transferred to the hospital record. In general, new information in the hospital record was poorly transferred to the RTHC on discharge; for example, weight (31%), diagnosis (63%) and treatment (48%).
CONCLUSIONS. The possession rate of RTHCs within the study sample was within an acceptable range. Although doctors generally made use of the RTHC as a reference source, their recording of new clinical information on the RTHC was poor, missing the opportunity to use it as a communication tool for continuity of care.
Patient-retained personal child health records (PCHRs) are used globally as a tool for the coordination of healthcare and to promote preventative health strategies.1-23 The South African version of the PCHR is the Road-to-Health Card (RTHC) with two versions currently in use: a 1995 chart version, and an updated 2011 booklet version.4,5 The Booklet is a more comprehensive record that contains space for clinical notes, updated growth charts and a recent version of the South African public immunisation schedule.
Low possession and retention of PCHRs, and inadequate use of PCHRs by health professionals, have lessened its efficacy. An international report advised that the median prevalence rate should not fall below 80% if vaccination coverage and health care co-ordination are to be achieved.6
Numerous international and local studies have highlighted three weak links in the use of the PCHR by health professionals: failure to request the record from the caregiver, failure to use the record as a reference source of the child's medical background, and failure to comprehensively and accurately record new information in the record.7-20 Much of the research on the weak links has relied on participant recall, which in many cases has not matched the health professional's medical notes. Few studies have examined both the PCHR and institutional clinical records to determine what information has been transferred in either direction.16,18,19
In this study, we sought to describe the level of possession of the RTHC by caregivers of patients admitted to Red Cross War Memorial Children's Hospital (RCWMCH), and to assess the degree and accuracy of doctors' use of the RTHC.
The study was approved by the Human Research Ethics Committee of the University of Cape Town (ref. no. HREC 119/2012) and the Hospital Research Committee of RCWMCH.
Methods
A descriptive, cross-sectional analytical study was conducted in four general paediatric wards at RCWMCH, a public sector teaching hospital in Cape Town providing a range of general and tertiary paediatric services. The four wards in which the study took place represented both acute care (short-stay wards) and longer-term care (long-stay wards).
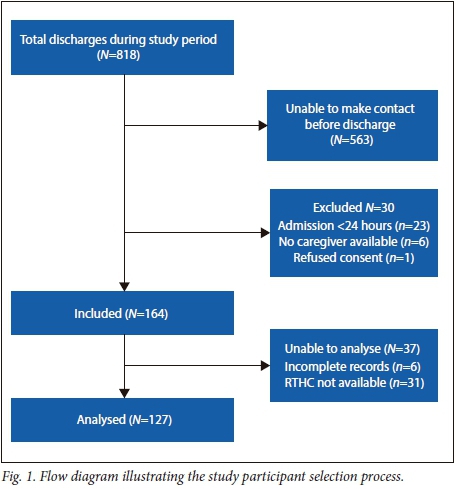
Consecutive patients were enrolled at discharge from these wards during office hours between 23 March and 30 April 2012. Exclusion criteria were: admission for <24 hours; absence of a caregiver; or absence of informed consent.
Following informed consent and enrolment, the primary author photographed all relevant pages of the RTHC. Data were extracted from the photographs of the RTHC and the participants' original hospital records. Two types of hospital records were in use at the time: an old version with a simple front sheet that was used to record a few patient and medical details, and a new version with a more comprehensive front section modelled on the RTHC Booklet, which was being phased in. Both the Chart and the Booklet versions of the RTHC were included. Only the front sections of the hospital record, the admission and discharge notes, and the treatment chart relevant to the most recent hospital stay were examined.
Demographic details, duration of hospital stay, primary diagnosis, and the presence or absence of pre-specified items of information on the RTHC and hospital record were recorded (Tables 1 and 2). It was assumed that the inward transfer of information occurred on admission, and outward transfer at admission and/or discharge. No attempt was made to categorise the clinical appropriateness of pre-specified information items in specific clinical cases.
The primary outcome was the proportion of pre-specified information that was transferred between RTHC and hospital clinical records, in both directions.
Target sample size was estimated by calculating 95% confidence intervals (CIs) for a range of potential sample sizes. A sample of 150 participants would have given confidence limits of 42% - 58% for a point estimate of 50%, and 6% - 16% for an estimate of 10%. Those were judged to be meaningfully precise for the purpose of the study.
Data were captured in Epidata 3.1, using patient code numbers to maintain anonymity. Thereafter the captured data were exported to a Microsoft Excel 2013 spreadsheet, in which much of the analysis was conducted. Data cleaning and analyses were performed using SPSS Statistics version 22 (IBM Corp., USA).
The database was stored securely on the main author's personal computer (PC) and on Google Drive, accessible only by the main author and the study supervisor (GS). Digital photographs were stored on the main author's PC and destroyed after review.
The presence of the pre-specified items of information in each record, and the transfer of available items between the records, were presented as proportions with Clopper-Pearson (exact) binomial CIs. A sub-group analysis was performed for 5 variables judged to be essential to any child's hospital admission, regardless of the child's age or diagnosis. Transfer proportions of these variables were compared by type of ward (short-stay v. long-stay), type of RTHC (chart v. booklet) and type of hospital record (old v. new). χ2 or Fisher's exact tests were used, as appropriate, for hypothesis testing.
Results
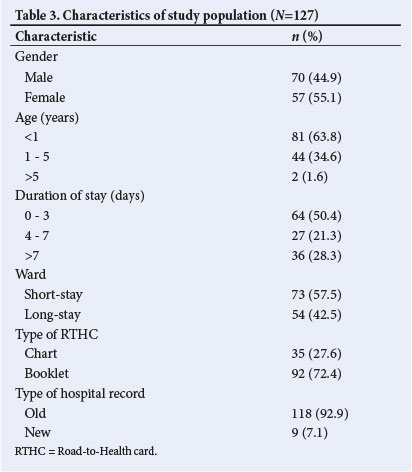
A total of 133 (81%) eligible participants had an RTHC with them and were recruited for this study (Fig. 1). Two of the hospital records were missing and 4 photos were incomplete, therefore only 127 participants were included in the analysis. The study population was classified according to various characteristics (Table 3.). Almost two-thirds of the participants were <1 year old (63.8%). The duration of stay for many of the patients was 3 - 7 days, and the distribution of patients between short-stay and long-stay wards was similar (57.5% and 42.5% respectively). Most of the participants possessed the RTHC Booklet (72.4%) and very few of the hospital records (7.1%) were in the new format. The two most common diagnoses were acute gastroenteritis (29%) and pneumonia (27%).
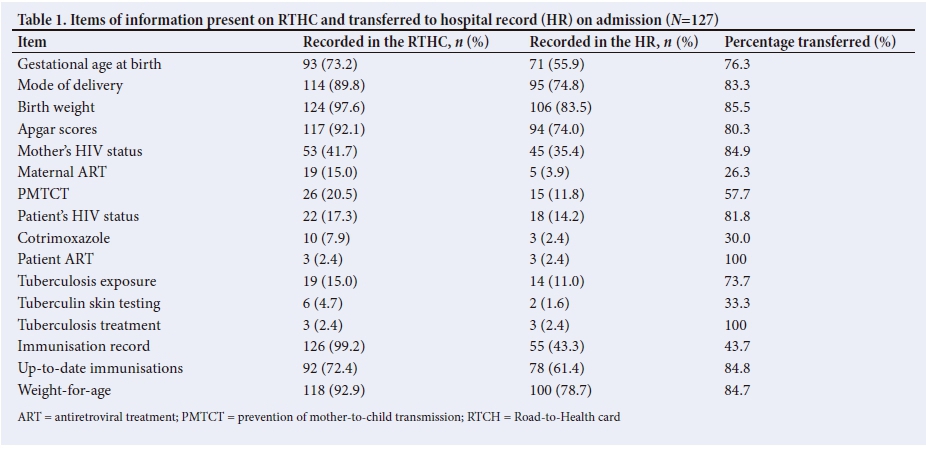
Information recorded on the patient's RTHC in most cases was well-transferred to the hospital record (Table 1). HIV status information was poorly transferred to the hospital record, except for maternal HIV status (transfer proportion 84.9%). Information on exposure to tuberculosis (TB) was mostly well-transferred (73.7%) but tuberculin skin test results were neither well-documented in the RTHC (4.7%; 95% CI 1.8 - 10) nor well-transferred to the hospital record (33.3%). Less than half (43.7%) of the full immunisation records were copied into the hospital record (95% CI 34.5 - 52.4) but the presence of completed age-appropriate, up-to-date (UTD) immunisations were transferred in 84.8% of cases. Weight-for-age scores were transferred in 84.7% of cases.
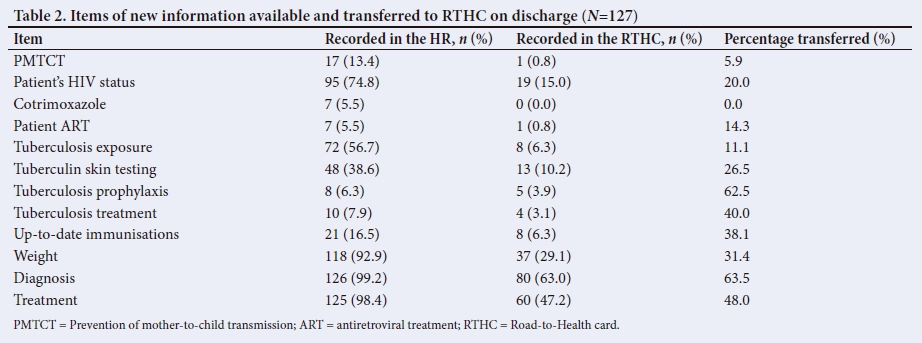
In general, the new information in the patient's hospital record was poorly recorded on the RTHC (Table 2). HIV status was available in 74.8% (95% CI 66.3 - 82.1) of hospital records but transferred to the RTHC in only 20% of such cases. Queries about TB exposure and the occurrence of tuberculin skin testing was noted relatively often in the hospital record, but not well-transferred to the RTHC (in only 11.1% and 26.5% of cases, respectively). The patient's weight was recorded or plotted in 92.9% (95% CI 87.0 - 96.7) of hospital records but transferred to RTHCs in only 31.4% of cases. The patient's diagnosis and treatment were almost always recorded in the hospital record but transferred in 63% and 48% respectively.
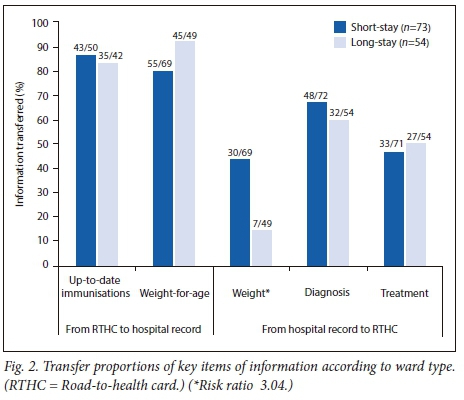
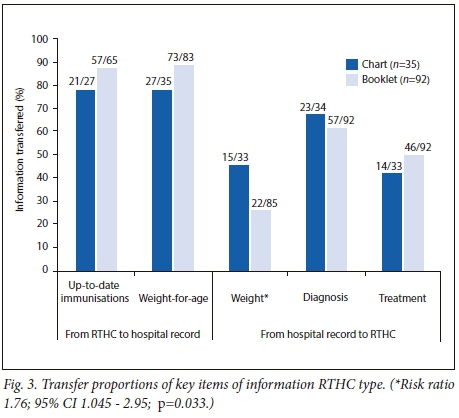
There was no statistically significant difference in the transfer proportions of key items of information by type of ward, type of RTHC and type of hospital record, except for the transfer of weight from the RTHC to the hospital record on discharge. The risk ratio for the transfer of weight data from the hospital record to RTHC in short-stay wards compared with long-stay wards was 3.04 (95% CI 1.46 - 6.36, p=0.003), and was 1.76 (95% CI 1.045 - 2.95, p=0.033) for the RTHC chart compared with the RTHC booklet (Figs 2 and 3, respectively). The sample size of new hospital records was too small (n=9) for any comparison with the older hospital records.
Discussion
This study sought primarily to determine the accuracy of bi-directional information transfer between patient-held records and institutional clinical records by comparing information in both sources of information. Whereas most previous research has focused on the possession of, and information recorded on, the PCHR, this study provides process information about key steps in the use of the PCHR as a tool for the continuity of health care i.e. transfer of information from the PCHR to institutional records, and of institutional information to the PCHR. This is also the first published study of the use of the South African 2011 RTHC Booklet in operational conditions that described its effectiveness as a means of communication between health professionals.
This study focused on practice in a specialised children's hospital, a small niche in the context of child health; but such hospitals remain important participants in the flow of clinical information about children with complex health problems.
The RTHC possession rate of 81% was just within the generally accepted recommended range of 80% or more6 and is a considerable improvement on the findings of previous research conducted at RCWMCH in 1991 (43%)21 and 1995 (61%).22
This study found that doctors at RCWMCH generally examined the RTHC and transferred relevant clinical information to the hospital record during admission. However, documentation of perinatal HIV information in the RTHC before arrival at RCWMCH was poor, and even what was available on admission was not well transferred. This probably reflects the social sensitivity of HIV infection in South Africa. The 2010 National Prevention of Mother-to-Child Transmission effectiveness survey showed that only 34% of the 10 612 included mothers had a clear indication of their HIV status on their child's RTHC.23 The low proportion of transfer to the hospital record in this study is presumably due to the priority given by busy clinicians to more recent data such as the patient's HIV and antiretroviral therapy status.
This study showed that the recording of new clinical information relating to the patient's hospital stay was poorly recorded on the RTHC. Much of the previous research on the RTHC, and PCHRs in general, has taken the form of simple audits that did not explicitly distinguish between information that was truly missing and information that was unavailable for transfer in the first place.
Some studies have aimed to assess agreement between the original medical record and the PCHR, generally showing that the transfer to the PCHR was poor. Although the findings of a 2008 French study showed excellent agreement for perinatal information, the transfer of Apgar scores (felt to be a socially sensitive subject) was poor.19 A 1998 South African study observed that, although new information was often entered on the RTHC during consultations, these details were often incomplete when compared with the clinic notes.16
Similarly, in a recent audit performed at RCWMCH, only 65% of the 41 RTHCs examined contained a clinical note pertaining to the patient's hospital visit.24 It is policy on discharge from RCWMCH to give the patient's caregivers a written summary of their hospital stay, and also to record salient information in the RTHC. This probably contributes to the poor recording of information on the RTHC, undermining its role and suggesting that it be used as the sole means of communication for less complex admissions. However, the use of a separate discharge letter nullifies the unique purpose of the RTHC to act as a central record of the child's health. These findings serve to confirm that the optimal use of the RTHC by doctors as a tool of communication for continuity of patient care was lacking.
No attempt was made to specify what information was clinically relevant to each child's age, diagnosis and reason for admission. However, in the subgroup analyses by types of ward, RTHC and hospital record, only variables that were deemed to be essential to any hospital admission, regardless of the child's age or diagnosis, were analysed. In this way, the study attempted to identify associations between transfer proportions and these three contexts. It was found that the probability of having weight transferred to the RTHC in short-stay wards was in short-stay wards compared with long-stay wards. Interpretation of this finding is difficult because differences in the health conditions managed in short-stay and long-stay wards could at least partially explain this difference, e.g. discharge weight would be essential information for children with acute gastroenteritis. Age was equally distributed across the wards and is unlikely to have been a contributing factor.
A convenience sample was used because of resource constraints, which undermines the generalisability of the findings to the study population (served by the four hospital wards in question). Misclassification could have occurred as some information recorded in the hospital record may have been obtained through history given verbally by the caregiver and not by only referencing the RTHC. This study may not exclusively represent the use of the RTHC by doctors, as no strategies were applied to identify information that may have been recorded by other types of health professionals. The unusual context for the use of this card in a specialist hospital further complicates the application of the findings to non-specialist health care settings. Nevertheless, these identified areas of weakness are likely to exist elsewhere, albeit to different degrees.
Conclusions
The level of possession of the RTHC by the children's caregivers admitted during the study period was acceptable. In a tertiary paediatric hospital setting, doctors used the RTHC as a reference source but failed to record new clinical information relating to the patient's hospital stay on the RTHC.
Recommendations
This audit serves as an initial step for an audit cycle at RCWMCH. Exploring barriers to the optimal use of the RTHC could be a first step to development and testing of interventions to improve performance, at RCWMCH and beyond.
Acknowledgements. The authors thank the caregivers who participated in this study and the hospital staff for their assistance and cooperation. We acknowledge the contributions from the UCT Writing Centre (translation of the consent form to Xhosa) and the UCT Department of Statistical Sciences (the statistical analysis).
Author contributions. JW and GS designed the study and developed the methodology. JW collected the data, performed most of the analyses and prepared the manuscript. The study was supervised by GS; the final manuscript was reviewed and edited by GS. This study was submitted by JW to UCT in partial fulfilment of an MMed in Paediatrics.
Funding. Funding was received from the UCT Department of Paediatric and Child Health and was used for payment of the statisticians; it was otherwise funded by the main author.
Conflicts of interest. None.Chopra M, Sanders D. Growth monitoring. In: Kibel M, Saloojee H, Westwood T, eds. Child Health for All: A manual for Southern Africa. Cape Town: Oxford University Press South Africa; 2012:108-109.
References
1. UNICEF. Home-based vaccination record repository. New York: UNICEF, 2003. http://www.immunizationcards.org/ (accessed 29 November 2015). [ Links ]
2. Turner KE, Fuller S. Patient-held maternal and/or child health records: Meeting the information needs of the patients and healthcare providers in developing countries? Online J Public Health Inform 2011;3(2). https://doi.org/10.5210/ojphi.v3i2.3631 [ Links ]
3. Western Cape Government Department of Health. The Road to Health Card. Western Cape Government; 2015. https://www.westerncape.gov.za/general-publication/road-health-card (accessed 29 November 2015). [ Links ]
4. Western Cape Government Department of Health. Minister Botha launches Road to Health Booklet. Western Cape Government; 2015. https://www.westerncape.gov.za/news/minister-botha-launches-road-health-booklet (accessed 29 November 2015). [ Links ]
5. Brown DW, Gacic-Dobo M. Home-based record prevalence among children aged 12-23 months from 180 demographic and health surveys. Vaccine 2015;33(22):258-293. https://doi.org/10.1016/j.vaccine.2015.03.101 [ Links ]
6. Tarwa C, de Villiers FPR. The use of the Road to Health Card in monitoring child health. SA Fam Pract 2007;49(1):15c-15d. https://doi.org/10.1080/20786204.2007.10873497 [ Links ]
7. Yach D, Metcalf C, Lachman P, et al. Missed opportunities for measles immunisation in selected Western Cape hospitals. S Afr Med J 1991;79(8):437-439. [ Links ]
8. Metcalf CA, Yach D, De Beer ZJ. Missed opportunities for immunisation at hospitals in the Western Cape - a reappraisal. S Afr Med J 1994;84(3):149-152. [ Links ]
9. Jeffs D, Nossar V, Bailey F, Smith W, Chey T. Retention and use of personal health records: A population based study. J Paediatr Child Health 1994;30(3):248-252 http://dx.doi.org/10.UU/j.1440-1754.1994.tb00627.x [ Links ]
10. Jeffs D, Harris M. The personal health record. Making it work better for general practitioners. Aust Fam Physician 1993;22(8):1417-1427. [ Links ]
11. Stacy RD, Sharma M, Torrence WA. Evaluation of the use of a parent-held Child health record by pregnant women and mothers of young children. Calif J Health Promot 2008;6(1):138-142. [ Links ]
12. Kitenge G, Govender I. Nurses' monitoring of the Road to Health Chart at primary healthcare level in Makhado, Limpopo Province. SA Fam Pract 2013;55(3):275-280. https://doi.org/doi.org/10.1080/20786204.2013.10874350 [ Links ]
13. Young S, Fasher M. An observational study of the NSW parent-held record in a GP setting. Aust Fam Physician 1994;23(4):704-712. [ Links ]
14. Donald PR, Hesseling PB. The 'Road to Health' card in a paediatric outpatient department. S Afr Med J 1987;72(5):356. [ Links ]
15. Harrison D, Heese HD, Harker H, Mann MD. An assessment of the 'Road-to Health' card based on perceptions of clinic staff and mothers. S Afr Med J 1998;88(11):1424-1428. https://doi.org/10.4102/curationis.v28i4.1021 [ Links ]
16. Lakhani AD, Avery A, Gordon A, Tait N. Evaluation of a home-based health record booklet. Arch Dis Child 1984;59(11):1076-1081. https://doi.org/10.1136/adc.59.11.1076 [ Links ]
17. Ferson MJ. Immunisation state and its documentation in hospital patients. Arch Dis Child 1990;65(7):763-767. https://doi.org/doi.org/10.1136/adc.65.7.763 [ Links ]
18. Troude P, L'Hélias LF, Raison-Boulley AM, Castel C, Bouyer J, de La Rochebrochard E. Perinatal factors reported by mothers: Do they agree with medical records? Eur J Epidemiol 2008;23(8):557-564. https://doi.org/doi.org/10.1007/s10654-008-9268-9 [ Links ]
19. Troude P, L'Hélias LF, Raison-Boulley AM, Castel C, Bouyer J, de La Rochebrochard E. Apgar scores reported in personal child health records: vVYach D, Metcalf C, Lachman P, et al. Missed opportunities for measles immunisation in selected western Cape hospitals. S Afr Med J 1991;79(8):437-439. [ Links ]
20. Metcalf CA, Yach D, De Beer ZJ. Missed opportunities for immunisation at hospitals in the Western Cape - a reappraisal. S Afr Med J 1994;84(3):149-152. [ Links ]
21. Woldesenbet SA, Jackson D, Goga AE, et al. Missed opportunities for early infant diagnosis: Results of a national study in South Africa. J Acquir Immune Defic Syndr 2015;68(3):e26-32. https://doi.org/doi.org/10.1097/QAI.0000000000000460 [ Links ]
22. Eyharts, D, Daron A, Scott C. Audit on the use of Road to Health cards - RCWMCH August 2015. The Advocacy Committee, School of Child and Adolescent Health. Cape Town: University of Cape Town; 2014 (unpublished audit). [ Links ]
 Correspondence:
Correspondence:
JI Wiles
jodiwiles@gmail.com
Accepted 10 April 2018


{kind=link}
{kind=link}