










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.11 no.4 Pretoria Dez. 2017
http://dx.doi.org/10.7196/sajch.2017.v11i4.1236
RESEARCH
doi:10.7196/sajch.2017.v11i4.1236
Association between HIV and proven viral lower respiratory tract infection in paediatric intensive care unit patients at Inkosi Albert Luthuli Central Hospital, Durban, South Africa
N P MajoziI; N NkwanyanaII; S ThulaIII; A CoutsoudisIV
IMB ChB, FC Paeds; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIMSc (Statistics); Department of Public Health Medicine, Faculty of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIIMB ChB, FC Paeds; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IVPhD;Department of Paediatrics and Child Health, Faculty of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND. Acute viral respiratory infections are common within the paediatric population. Nucleic acid amplification tests can identify a wide range of respiratory viruses. Virally infected patients can now be diagnosed early and more accurately in the acute phase of illness.
OBJECTIVES. To examine the association between HIV status and mortality in children with viral lower respiratory tract infection (LRTI) and to delineate the profile of identified viruses.
METHODS. We conducted a retrospective review of charts of children aged from birth to 10 years of age who were admitted to the paediatric intensive care unit at Inkosi Albert Luthuli Central Hospital with a viral LRTI between December 2010 and May 2015. Only patients who had a positive respiratory viral multiplex test were eligible for entry into the study. Patients were grouped according to their HIV status and mortality was assessed.
RESULTS. A total of 338 records were analysed in this study. Sixty-five patients tested HIV-positive (19.2%) and 80.8% were HIV-negative (n=273). There were 55 mortalities: 12 were among the 65 HIV-positive patients (18.5%) and 43 among the 273 HIV-negative patients (15.8%). The difference in mortality according to HIV status was not statistically significant (p=0.595). Respiratory syncytial virus was the most prevalent virus identified overall, with adenovirus being most prevalent in the HIV-positive group.
CONCLUSION. The results showed that patients with viral LRTIs who required respiratory support had a similar mortality regardless of HIV status.
Acute viral respiratory infections are common within the paediatric population, irrespective of HIV status, and are a common cause of admission to hospital in developed countries as well as a major cause of death in developing countries[1] These viral infections are responsible for a large number of lower respiratory tract infections (LRTIs), including bronchiolitis, croup, acute exacerbations of asthma or wheezing and pneumonia.[2] It is estimated that viral respiratory infections contribute between 40 and 80% of respiratory morbidity.[3]
Virally infected patients may present with fever, myalgia, fatigue, cough, rhinitis and pharyngitis. Generally, the viruses causing respiratory illness have a short incubation period and are spread from person to person by direct contact with contaminated secretions or aerosolised droplets.
Viruses that have been identified as causing respiratory illness include respiratory syncytial virus (RSV), influenza A and B, adenovirus, rhinoviruses and parainfluenza viruses 1, 2 and 3.[2] In the 2000s, more viruses were discovered to cause respiratory infection.[1] These new viruses include human metapneumovirus, severe acute respiratory syndrome corona virus, parainfluenza 4, avian influenza viruses and enterovirus.[1] Rare causes include Epstein-Barr virus, cytomegalovirus, varicella-zoster virus, herpes simplex virus and measles. These pathogens generally have overlapping signs and symptoms, which makes it very difficult for attending physicians to make a distinction of the causative viral pathogen based on signs and symptoms alone without laboratory assistance.[1] It is also rather difficult to distinguish infection secondary to viral infection versus bacterial infection based on clinical presentation alone - this leads to a large number of patients being treated inappropriately with antibiotics for viral infections. Management is mainly symptomatic and supportive care and there are only a few antiviral agents available for use against specific viruses.
There are various ways of identifying viral respiratory infections, including identification of the virus by an immunofluorescence assay (IFA), serology tests which use the patient's serum to detect virus-specific antibodies, and viral antigens using an enzyme-linked immunosorbent assay (ELISA).[5] These tests are of little use in the acute phase of the illness as a four-fold increase in viral titre is required to detect infection.[6]
A second test involves the isolation of virus by cell culture from patient samples and identification of the virus by immunofluorescence assays (IFA).[5] However, cultures require a long incubation time and special incubation media, which makes them costly.[6]
Previously, viral isolation and serology were the mainstay of laboratory diagnosis of respiratory viral infections.[1] However, nucleic acid amplification tests emerged in the 1980s and have now been developed for a wide range of illnesses, including those caused by respiratory viruses. These tests can detect very low levels of viral nucleic acids and have increased laboratory sensitivity for diagnosing viruses.[3] Respiratory samples used for diagnosis include endotracheal aspirates, broncho-alveolar lavage, nasopharyngeal swabs and aspirates, throat swabs, as well as sputum and tissue samples from lung biopsy. Infected patients can now be diagnosed early and more accurately in the acute phase of illness when they may still be shedding low levels of the virus. This earlier and more accurate diagnosis is helpful in a number of ways. It allows the patient to receive more appropriate therapy earlier, where indicated, it allows for infection control measures to be instituted and it allows public health officials to be aware of what pathogens are circulating in the community and hospitals. The multiplex polymerase chain reaction (PCR) tests are of even greater benefit as they test for a wide range of viruses simultaneously.
KwaZulu-Natal Province (KZN) has the highest prevalence of HIV infection in South Africa (SA), with a prevalence of 41.3% in 2013. The national HIV prevalence rate among antenatal women was estimated at 29.7% in 2013.[7] In January 2015, the SA government introduced the Option B+ approach to reduce mother-to-child transmission of HIV during pregnancy, delivery and the postnatal period.[8] Despite these improved interventions and low recently reported figures of transmission rates in KZN (1.3%),[9] the paediatric intensive care unit (PICU) at Inkosi Albert Luthuli Central Hospital (IALCH) still receives a sizeable number of HIV-infected patients.
The PICU at IALCH has in the past few years instituted respiratory viral multiplex PCR testing for children admitted with a respiratory disease in order to diagnose viral respiratory infection.
The aim of this study was to examine the association between HIV infection and viral LRTI in paediatric patients requiring intensive care. The primary outcome examined was mortality, as an association between HIV status and outcome of respiratory viral infection may assist physicians in the medical management of patients. A secondary aim of the study was to delineate the frequency of viruses associated with respiratory illness in our setting.
Methods
The study was approved by the University of KwaZulu-Natal Biomedical Research Ethics Committee (ref. no. BREC REF:515/14) and was conducted at the IALCH (Durban, KZN, SA), which is a tertiary referral hospital with a 14-bed PICU.
The study involved a retrospective review of records of children aged from birth to 10 years who had been admitted to the PICU at IALCH with a viral LRTI between December 2010 and May 2015.
Demographics of study participants
The majority of the patients were males (58.9%; n=199/338). The participants' age at presentation was classified into age range intervals ranging from 0 days to 10 years. The majority of the 338 patients (Fig. 1) in the study were within the age range 'birth to 3 months of age' and 13% (n=44) of all the study participants were born premature (<37 weeks' gestation). In total, 292 of the study participants had their birth weight documented, which ranged from 900 g to 4 900 g, with a median birth weight of 2 800 g: 10.6% (n=31/292) weighed <1 500 g and were classified as very low-birth-weight infants, and 34.9% (n=102/292) were low-birth-weight infants, with a birth weight of <2 500g. The World Health Organization (WHO) weight-for-age Z-scores were assigned to 303 patients who had their weights documented on admission. Of the 303 patients, 65.3% (n=198) had normal weight-for-age; 15.2% (n=46) were underweight for their age; 14.9% (n=45) were severely underweight for their age; and 4.6% (n=14) were overweight for age.

Clinical characteristics of the study participants
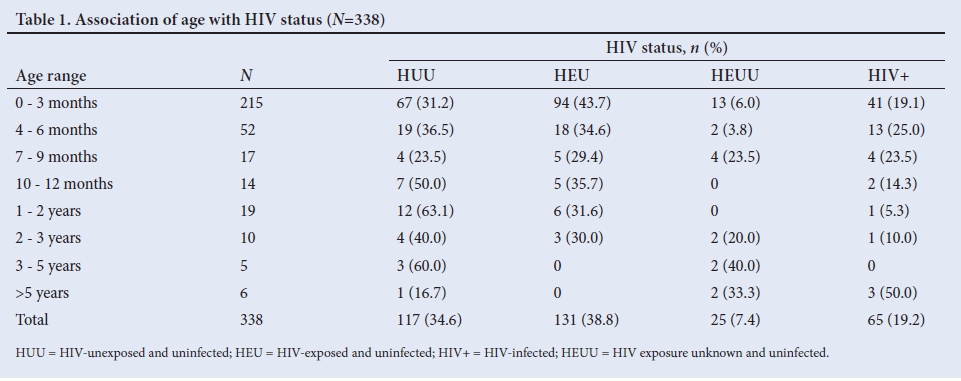
In total, 19.2% (n=65/338) of the patients tested HIV-positive and 80.8% (n=273/338) tested HIV-negative. Of the HIV-negative patients, 131, 117, and 25 were born to HIV-infected mothers, HIV-uninfected mothers and mothers with unknown HIV status, respectively. Details of the age categories of the different HIV status groups are shown in Table 1.
We examined those who had been exposed to maternal HIV (58.0%; n=196) to determine how many had participated in the prevention of mother-to-child transmission (PMTCT) programme. As there was no register to confirm who was part of the PMTCT programme, we accepted any documentation in the chart that the patient had received PMTCT and also included those paediatric patients who received either nevirapine (NVP), zidovudine (AZT) or NVP and AZT in the first 6 weeks of life as having been part of the programme. Of the HIV-positive patients, 47.7% (n=31/65) had not received PMTCT according to their records, 18.5% (n=12/65) received PMTCT and 33.8% (n=22/65) had no documentation of PMTCT. Of the HIV-negative patients, 48.0% (n=131/273) were HIV-exposed and 69.0% (n=89/131) of them had received PMTCT; however, it was not possible to distinguish patients that followed the entire PMTCT programme from those that only partially participated.
The majority of the HIV-positive patients were diagnosed for the first time in the PICU. This meant that they were not on highly active antiretroviral therapy (HAART) when they acquired the viral LRTI. Only 10.8% (n=7/65) were on HAART at the time of admission to the PICU. CD4% values were documented for 53 (n=53/65) patients and absolute CD4 counts for 51 (n=51/65) patients. Only 43 (n=43/65) patients had previously had a viral load test done.
Mortality and clinical outcomes
Overall, 16.3% (n=55) of the patients died and 83.7% (n=283) were discharged. There was no significant difference in the mortality rate based on gender, with the females having a slightly higher mortality rate compared with the males (18.0% v. 15.1%, respectively; p=0.476). Although the mortality rate was highest (29.0%) among the very low-birth-weight infants (<1 500 g), the association between mortality and birth weight was not significant (p=0.174).
The poorest outcome was found in the 'severely underweight-for-age' group, with a mortality rate of 26.7%, followed by the 'underweight-for-age' group, with a mortality rate of 19.6%. This association between mortality and weight-for-age was not significant (p=0.12).
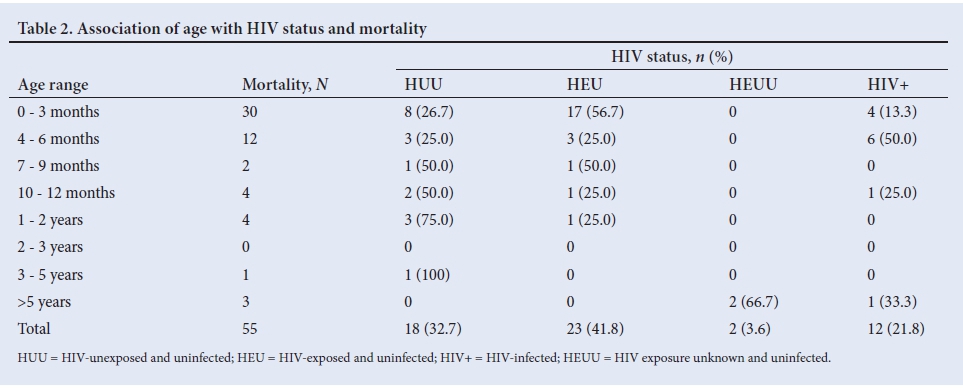
There were 55 mortalities: 18.5% (n=12/65) of the HIV-infected patients and 15.8% (n=43/273) of the HIV-uninfected patients had died. The difference in mortality according to HIV status was not statistically significant (p=0.595). A breakdown of the 55 deaths based on age and HIV status is shown in Table 2. Of the 55 deaths, 21.8% (n=12/55) were in HIV-infected children (HIV+); 41.8% (n=23/55) were in HIV-exposed but uninfected children (HEU); 32.7% (n=18/55) were in HIV-unexposed infants (HUU); and 3.6% (n=2/55) were in the HEUU group.
Feeding options were examined in patients who were <1 year of age (n=298). Of these 298 patients, feeding options were only documented for 55.4% (n=165/298). Of these 165 patients, 50.9% (n=84/165) were exclusively breastfed, 41.2% (n=68/165) were exclusively formula-fed and 7.9% (n=13/165) were mixed-fed. Feeding practice was only documented in 40.0% (n=22/55) of the deceased patients. The mortality rate was highest in the mixed-fed group (30.7%; p=0.192).
Most patients spent between 8 and 14 days in the PICU. The length of stay in the PICU was not affected by birth weight, feeding practice, nutritional status or HIV status.
Profile of viral infections
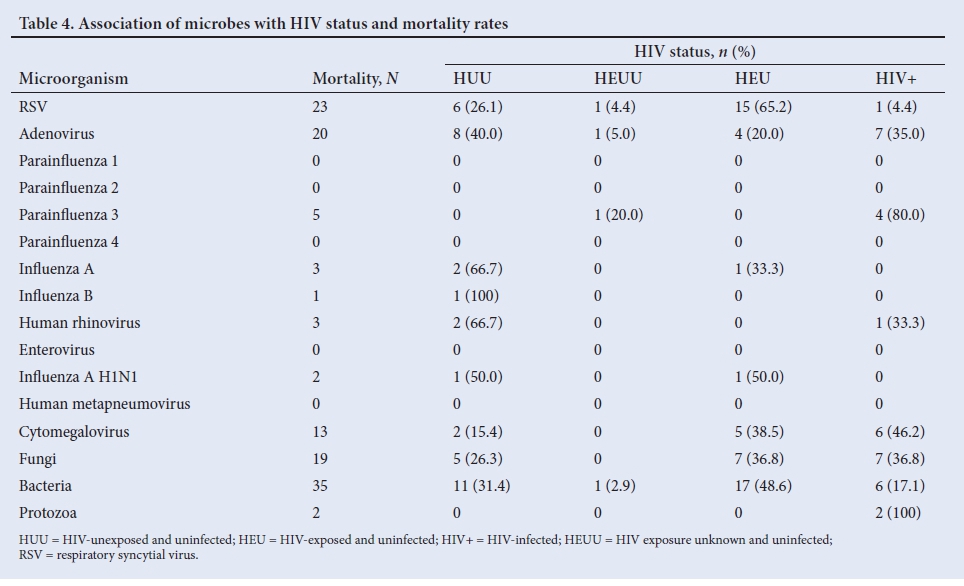
In total, 11 different viruses were identified by the respiratory viral multiplex PCR test. Ten patients had more than one virus identified. RSV was the most commonly identified virus (44.7%), followed by adenovirus , which accounted for 26.7% of all isolates. Other viruses included parainfluenza (types 1, 2, 3 and 4), influenza A and B, influenza A H1N1 (a subtype of the influenza A virus), human rhinovirus and enterovirus. Other microbes identified by various other methods included bacteria, fungi and Pneumocystis jirovecii pneumonia (PCP) and cytomegalovirus (CMV) (Table 3).
Although RSV was the most commonly identified virus, the mortality rate owing to RSV infection was only 14.7% (n=23/156). The highest mortality rate was in patients from whom influenza A H1N1 virus had been isolated - there were only 4 patients in this category but the mortality rate was 50.0% (n=2/4). Adenovirus had a mortality rate of 21.5% (n=20/93), followed by influenza A with a mortality rate of 18.8% (n=3/16). The mortality rate in patients with concomitant infections was as follows: CMV infection 16.3% (n=13/80; p=0.995); fungal infection 43.2% (n=19/44) (p=0.0); and bacterial infection 23.3% (n=35/150; p=0.002).
Discussion
LRTIs remain a significant cause of morbidity and mortality in the paediatric community. Mortality in childhood pneumonia is highest in children <2 years of age[4] and is responsible for 45% of under-5 mortality globally.[10] Forty-four percent of under-5 deaths occur during the neonatal period owing to preterm birth complications, pneumonia and intrapartum-related complications.[10] A systematic review of the literature by Slogrove et al.[11] found that HEU infants were at a greater risk for infectious morbidity and mortality compared with HUU infants with more severe manifestation of disease and more frequent hospitalisation. The greatest relative difference between HEU and HUU infants in morbidity and mortality occurs beyond the neonatal period, as it wanes by the second year of life.
With the resource limitations and inadequate ICU bed availability in KZN, it is often challenging for medical personnel to decide ethically on which patients should be prioritised for respiratory support in PICUs. HIV-infected patients may present with various infections, recurrent infections and prolonged infections. However, this study has shown that viral LRTIs are common in both immunocompetent and immunocompromised patients and that patients may require respiratory support regardless of their immune status. Furthermore, it may be expected that HIV-infected patients harbour a viral infection for longer with a longer period of viral shedding; however, this study showed that the overall length of stay in the PICU and the duration of respiratory support was between 8 and 14 days and 4 to 7 days, respectively, irrespective of HIV status.
Additionally, the mortality rate in patients with viral LRTIs was shown to be similar in HIV-positive patients and HIV-negative patients requiring respiratory support.
Our study confirmed that RSV is the most common cause of viral LRTI in SA, where a 2-fold increase in the annual incidence of hospitalisation and a higher case fatality ratio was found in HIV-infected children who were not on antiretroviral treatment and had severe RSV-associated acute LRTI. This increased risk was greatest during infancy. Even with HIV treatment, the case fatality ratio in SA remains higher in HIV-infected children compared with HIV-uninfected children.[12]
CD4 cell counts and viral loads are surrogate markers of disease progression in children and adults. The normal absolute CD4 cell count varies widely with age, therefore CD4% is preferred in children <5 years of age. Both CD4% and viral load are independent predictors of clinical progression, although CD4% is the stronger predictor.[6] Only 9 of the 12 deaths that occurred in the HIV-positive group had documented CD4 cell counts and viral loads. As expected, more than half of them had CD4% values of <25.0% and viral loads of >10 000 copies/mL. Although these numbers are too small to be statistically significant, the immune status of these patients most likely played a role in their outcome.
Study limitations
One of the limitations of the study was that we only looked at viruses identified by the viral multiplex PCR test and therefore some of the viruses that cause significant respiratory morbidity and mortality were not included in this study. Measles has been described as causing more severe illness in immunocompromised patients but this virus is not detected by the multiplex PCR test. CMV has also been shown to be an opportunistic infection in immunocompromised patients with significant mortality but it is tested for using a different molecular test.
In this study we did not differentiate patients with only a viral infection from those who were co-infected with other microbes or had superimposed bacterial infection. Overall, HIV-positive patients were found to have a higher incidence of co-infection with other microbes.
A major limitation of the study was that this was a purposive retrospective sample of patients during a defined time period and as such may not have had the required power to show statistically significant differences between the HIV-infected and HIV-uninfected patients in terms of associations between mortality, birth weight and weight-for-age category.
Conclusion
Owing to resource constraints, viral multiplex PCR testing is not widely available in our public hospitals and therefore diagnosing viral infections in paediatric patients remains a clinical diagnosis in most parts of KZN. Although this study was a retrospective observational study of a small population, it showed that patients with viral LRTI who require respiratory support have a similar outcome regardless of HIV status. Also of note, was the observation that 89.2% of the HIV-infected children were admitted without being on HIV treatment, which highlights the importance of increasing efforts to ensure adherence to the new SA guidelines of testing all HIV-exposed infants at birth and starting treatment for those that test HIV-positive immediately.[8]
Acknowledgements. The authors would like to acknowledge Dr KE Letebele, medical manager at IALCH, for giving us permission to conduct this research at the hospital. We would also like to acknowledge the National Health Laboratory Service for providing us with essential information for this project to proceed.
Author contributions. NPM: Developed the initial draft, collected the data and worked on the project to completion. AC: Reviewed every draft and assisted with writing and editing; approved the final manuscript. ST: Conceptualised the project and assisted with editing. FN: Performed the statistical analysis and assisted with writing the final article.
Funding. None.
Conflicts of interest. None.
References
1. Mahony JB. Detection of respiratory viruses by molecular methods. Clin Microbiol Rev 2008;21(4):716-747. https://doi.org/10.1128/cmr.00037-07 [ Links ]
2. Pavia AT. Viral infections of the lower respiratory tract: Old viruses, new viruses, and the role of diagnosis. Clin Infect Dis 2011;52(S4):S284-S289. https://doi.org/10.1093/cid/cir043 [ Links ]
3. Kitchin OP. The role and management of viruses in hospital and community aquired pneumonia. Paediatric Focus 2013;4(4):5-7. [ Links ]
4. Zar HJ. Childhood Pneumonia in Africa - a major challenge for child health. S Afr Respir J 2013;19(4):114-116. [ Links ]
5. National Health Laboratory Service (NHLS). Clinician's Handbook. Durban: NHLS, 2014. [ Links ]
6. Ozeas G, Ricardo FL, Bruno GB. Update on viral community-aquired pneumonia. Revista da Associacao Medica Bradileira 2013;59(1):78-84. [ Links ]
7. National Department of Health (NDoH). The 2013 National Antenatal Sentinel HIV Prevalence Survey South Africa. Pretoria: NDoH, 2015. [ Links ]
8. NDoH. National Consolidated Guidelines for PMTCT and the Management of HIV in Children, Adolescents and Adults. Pretoria: NDoH, 2015. [ Links ]
9. Mhlongo OB, Moyo F, Mazanderani AF, Sherman GG. HIV PCR testing at birth in KZN, South Africa - one year post introduction of the largest neonatal HIV testing programme. Abstract, Eighth International Workshop on Paediatrics. Durban, South Africa 15 - 16 July 2016. Rev Antiviral Ther Infect Dis 2016. http://www.infectiousdiseasesonline.com/wp-content/uploads/2016/07/8th-HIVPediatrics_abstractbook [ Links ]
10. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 2015;385(9966):430-440. https://doi.org/10.1016/s0140-6736(14)61698-6 [ Links ]
11. Slogrove L, Goetghebuer T, Cotton F, Singer J, Bettinger J. Pattern of infectious morbidity in HIV-exposed uninfected infants and children. Front Immunol 2016;7:Article 164. https://doi.org/10.3389/fimmu.2016.00164 [ Links ]
12. Moyes J, Cohen C, Pretorius M, et al. Epidemiology of respiratory syncytial virus- associated acute lower respiratory tract infection hospitalizations among HIV- infected and HIV-uninfected South African children, 2010-2011. J Infect Dis 2013;208(Suppl 3):S217-S226. https://doi.org/10.1093/infdis/jit479 [ Links ]
 Correspondence:
Correspondence:
N P Majozi
sitholenp@gmail.com
Accepted 10 May 2017


{kind=link}
{kind=link}
{kind=link}
{kind=link}