










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Child Health
versión On-line ISSN 1999-7671
versión impresa ISSN 1994-3032
S. Afr. j. child health vol.8 no.3 Pretoria sep. 2014
RESEARCH
Blood pressure profile in children aged 3 - 5 years: Relationship to age, weight, height, gender and body mass index
P N C ManyikeI; C O OkikeII; J M ChinawaIII; I E ObiIV; U C UkohV
IMBBS, FWACP; Federal Teaching Hospital, Abakaliki, Nigeria
IIMBBS, FWACP; Federal Medical Centre, Asaba, Nigeria
IIIMBBS, FMCPaed; Department of Pediatrics, College of Medicine, University of Nigeria/University of Nigeria Teaching Hospital (UNTH), Ituku-Ozalla, Nigeria
IVMBBS, FMCPH; Department of Community Medicine, College of Medicine, University of Nigeria/University of Nigeria Teaching Hospital (UNTH), Ituku-Ozalla, Nigeria
VMBBS; Federal Teaching Hospital, Abakaliki, Nigeria
ABSTRACT
BACKGROUND: Blood pressure measurement is not commonly done in children. Most of the studies done in Nigeria so far on blood pressure and hypertension are in older children.
OBJECTIVES: To determine the blood pressure profile in children aged 3 - 5 years, establish the relationship between their blood pressure and age, body mass index (BMI), height, weight and gender, and compare the results with available values.
METHODS: A total of 603 apparently healthy nursery school children aged 3 - 5 years were randomly recruited from three nursery schools: two in Abakaliki, Ebonyi State, and one in Asaba, Delta State. Their blood pressure, height and weight were measured and their BMI calculated.
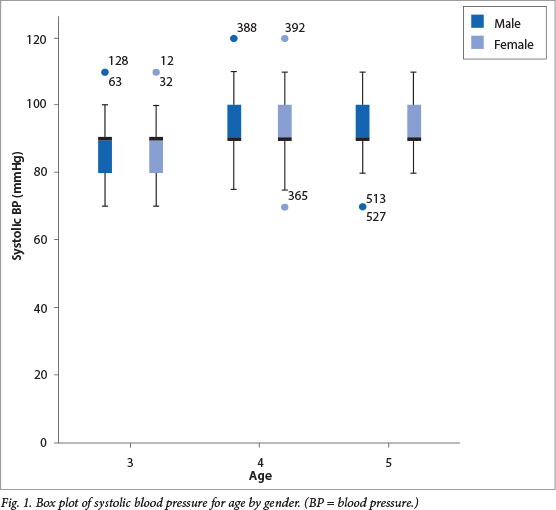
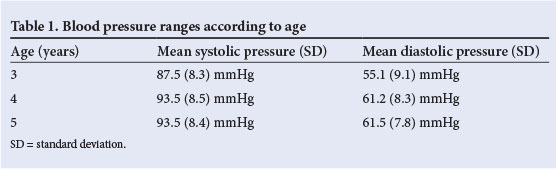
RESULTS: Of the 603 pupils, 311 (51.6%) were males and 292 (48.4%) were females. Blood pressure ranged from 70/40 to 120/90, with mean (standard deviation) systolic values for pupils aged 3 years 87.5 (8.3) mmHg, aged 4 years 93.5 (8.5) mmHg and aged 5 years 93.5 (8.4) mmHg, and mean diastolic values for pupils aged 3 years 55.1 (9.1) mmHg, aged 4 years 61.2 (8.3) mmHg and aged 5 years 61.5 (7.8) mmHg. No gender difference was found, but age, height and weight all correlated positively with blood pressure. The values found in this study were similar to those in the literature.
CONCLUSION: The mean systolic and diastolic blood pressures of the age group studied were 91.3 (8.9) mmHg and 59.0 (9.0) mmHg. The blood pressure values obtained in this study were similar to published values in the literature.
Blood pressure (BP) measurement is a necessary part of the physical examination of children.[1,2] The most obvious statement about children's BP is that it is not taken seriously.[3] There is a lack of awareness of hypertension in children,[4] with a common belief that measurement of BP in infants and children is difficult and time consuming, with results usually normal.[3] However, measurement of BP in children merely requires patience, practice and an appropriate cuff size of 3 - 13 cm wide.[3] BP varies with age,[4,5] height[6] and sex,[7] progressively increasing from infants to adolescents.[8,9]
The prevalence of hypertension in childhood is probably between 1% and 3%,[8] but the majority of children will have mild increases in BP and can be regarded as having primary (essential) hypertension.[9] Primary hypertension in childhood is being increasingly recognised, is found to cluster in families and is associated with obesity.[9] The prevalence of hypertension increases progressively with increasing body mass index (BMI); some studies have detected hypertension in over 30% of obese children (BMI >95th percentile)[10-12]
In infants and young children, systemic hypertension is uncommon, but when present, it is usually indicative of an underlying disease.[4] The American Heart Association and the American Academy of Pediatrics recommend that children have their BPs checked regularly from 3 years old onwards.[13] The normal auscultatory method can be carried out over the age of 3 years but is more difficult in younger children, in whom sedation may be necessary.[14]
Very few studies have been done in Nigeria on BP in this particular age group (3 - 5 years old), hence the reason for this study.
Method
This is a multicentre, cross-sectional, descriptive study done between July 2012 and December 2012. Nursery school children between the ages of 3 years and 5 years from a random selection of schools comprised the study population. Those below 3 years and those above 5 years were not recruited.
Consent was obtained from the school authority, who informed the parents of the children about the study; the parents' consent was also obtained. Ethical clearance for the study was obtained from the Research and Ethical Committee of Ebonyi State University.
Children who cried or refused to participate were not recruited. The BP, weight and height of randomly selected, cooperative children were measured. An aneroid sphygmomanometer with standardised calibrations (Hospital and Home Care; CEO197 certified) was used to measure the BP. The cuff covered two-thirds of the right upper arm. Phase 1 and phase 5 of the Korotkoff sounds were used to determine the systolic and the diastolic BPs, respectively. The children's BP was taken in the school setting with the children relaxed and in the sitting position. BP measurements were done in the morning. Three consecutive readings were taken and the average BP calculated. Weight and height were measured with a stadiometer, with the children's shoes off. BMI was calculated using the formula: BMI = weight (kg)/height2 (m).
Data were analysed with SPSS software, version 20 (California, US).
Results
Of a total of 603 children aged 3 - 5 years included in the study, 311 (51.6%) were males and 292 (48.4%) were females. The children ranged in height from 78 cm to 121 cm, with a mean of 103.4 cm. Weight ranged from 10.0 kg to 32.0 kg, with a mean of 17.4 kg, and BMI ranged from 11.2 to 32.9, with a mean of 16.3.
BP ranged from 70/40 mmHg to 120/90 mmHg, with a mean (standard deviation (SD) systolic pressure of 91.3 (8.9) mmHg (range 82.4 - 100.1 mmHg) and a mean diastolic pressure of 59.0 (9.0) mmHg (range 50.0 - 68.0 mmHg) (Table 1). Figs. 1 and 2 show box plots of systolic and diastolic pressures by gender and age.
A positive correlation between BP (systolic and diastolic) and age, BMI, height and weight was observed. There was no positive correlation between BP and gender with p>0.05.
Tables 2 - 5 show the percentiles constructed for systolic pressure and diastolic pressure by gender, height, weight and BMI.
Discussion
In this study, we used a calibrated, certified aneroid sphygmomanometer for the BP measurements. Shah et al.,[15] working in America, noted that mean mercury and aneroid systolic and diastolic BPs were highly correlated. For the entire group, there was no significant difference in mean systolic BP using the aneroid device.
In our study, the mean systolic BP was 91.28 (8.86) mmHg (range 82.42 -100.14 mmHg), with a mean diastolic of 59.00 (9.03) mmHg (range 49.97 - 68.03 mmHg). These data are similar to Aderele and Seriki's,[16] who studied 100 children aged 3 - 7 years and obtained mean systolic and diastolic BPs of 89 mmHg and 55 mmHg, respectively. Similarly, Rosner et al.[17] found mean systolic and diastolic BPs of 93.4 mmHg and 53.6 mmHg, respectively, for 5-year-old black males, and 93.1 mmHg and 54.2 mmHg for 5-year-old black females. These do not differ significantly from the values measured in our 5-year-old participants.
We noted no gender difference in BP from our study. Abdurrahman and Ochoga[18] also noted no gender difference with BP in their study. Similarly, Hamidu et al.,[9] in their study on children aged 5 - 6 years, observed no gender difference in mean systolic BPs, but reported a mean diastolic BP of 97 (5) mmHg (higher than systolic) in the females. In their study, they found that BP increased with age, and that gender did not influence BP, which is in agreement with our study.
Goss[13] noted that the upper limit for normal systolic pressure in children aged 3 - 5 years ranged from 104 mmHg to 116 mmHg, depending on height and gender, while the upper limit for diastolic pressure ranged from 63 mmHg to 74 mmHg. Huff[19] noted a systolic BP of 99 mmHg and a diastolic BP of 65 mmHg. Ogunkunle et al.,[20] in their study on children aged 36 - 47 months, found that gender did not affect the BP, but age, height and weight all correlated positively with BP, also in agreement with our study. In addition, 3.2% and 1.7% of their study population had systolic and diastolic hypertension, respectively, while our study recorded 0.3% for systolic hypertension and 2.7% for diastolic hypertension, which brings the total prevalence to 3%. These proportions do not differ significantly from published values.[7,8]
We obtained a mean height of 78 cm and mean weight of 10 kg in our study, which showed stunting and wasting, respectively, in some of our 3-year-old participants. This is not surprising as malnutrition is still a public health issue in Nigeria. This is buttressed by the fact that nearly 20 million children are severely acutely malnourished worldwide, mostly in south Asia and in sub-Saharan Africa.[21]
Primary or essential hypertension in childhood is being increasingly recognised, is found to cluster in families and is associated with obesity.[9] Recent studies have also inferred that because of more frequent routine BP recordings in children, mild essential or primary hypertension is being increasingly diagnosed, and is stated to be the most common cause of high BP in children.[22]
Conclusion
The values in our study and other studies cited are normal and range between the published 50th and 90th age-specific percentiles of BP in children aged 1 - 13 years.[7]
Routine BP measurement should be a key aspect of physical examination of children since they are not immune from essential hypertension. This will allow for early detection of essential or primary hypertension and proper follow-up, especially considering that childhood hypertension can track into adulthood.
References
1. Balu HA. Clinical Methods in Pediatric Diagnosis. Delhi: CBS Publishers, 1990:69. [ Links ]
2. Frese EM, Fick A, Sadowsky HS. Blood pressure measurement guidelines for physical therapists. Cardiopulm Phys Ther J 2011;22(2):5-12. [ Links ]
3. Gill D, O'Brien N. Paediatric Clinical Examination Made Easy, 5th ed. Edinburgh: Churchill Livingstone, 2007:108. [ Links ]
4. Bernstein D. Diseases of the peripheral vascular system: Hypertension. In: Kliegman B, Jenson S, eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia: Saunders, 2007:1988-1995. [ Links ]
5. Obika LF. Pattern of paediatric blood pressure in rural, semi-urban and urban communities in Ilorin, Nigeria. Afr J Med Med Sci 1995;24(4):372-377. [ Links ]
6. Luma GB, Spiotta RT. Hypertension in children and adolescents. Am Fam Physician 2005;5:1-11. [ Links ]
7. Din-Dzietham R, Liu Y, Bielo MV, Shamsa F. High blood pressure trends in children and adolescents in national surveys, 1963 to 2002. Circulation 2007;116(13):1488-1496. [ Links ]
8. Odetunde OI, Neboh EE, Chinawa JM, Okafor HU, Odetunde OA, Ezenwosu, Ekwochi U. Elevated arterial blood pressure and body mass index among Nigerian preschool children population. BMC Pediatrics 2014;14:64. [http://dx.doi.org/10.1186/1471-2431-14-64] [ Links ]
9. Hamidu LJ, Okoro EO, Ali MA. Blood pressure profile in Nigerian children. East Afr Med J 2000;77(4):180-184. [ Links ]
10. Sorof J, Daniels S. Obesity hypertension in children: A problem of epidemic proportions. Hypertension 2002;40(4):441-447. [ Links ]
11. Freedman DS, Dietz WH, Srinivasan SR, Berenson GS. The relation of overweight to cardiovascular risk factors among children and adolescents: The Bogalusa Heart Study. Pediatrics 1999;103(6 Pt 1):1175-1182. [ Links ]
12. Graf C, Rost SV, Koch B, et al. Data from the StEP TWO programme showing the effect on blood pressure and different parameters for obesity in overweight and obese primary school children. Cardiol Young 2005;15(3):291-298. [ Links ]
13. Goss HV. Normal Blood Pressure Range for Children. http://www.livestrong.com/article/22730 (accessed 30 November 2013). [ Links ]
14. Forfar JO. History taking, physical examination and screening. In: Campbell AGM, Neil M (eds). Forfar and Arniel's Textbook of Pediatrics, 4th ed. Edinburgh: Churchill Livingstone, 1992:22. [ Links ]
15. Shah AS, Dolan LM, D'Agostino RB Jr, et al. Comparison of mercury and aneroid blood pressure measurements in youth. Pediatrics 2012;129(5);1205-1210. [http:dx.doi.org/10.1542/peds.2011-3087] [ Links ]
16. Aderele WI, Seriki O. Hypertension in Nigerian children. Arch Dis Child 1994;49(4):313-317. [ Links ]
17. Rosner B, Prineas R, Daniels SR, Loggie J. Blood pressure differences between blacks and whites in relation to body size among US children and adolescents. Am J Epidemiol 2000;151(10):1007-1019. [ Links ]
18. Abdurrahman MB, Ochoga SA. Casual blood pressure in school children in Kaduna, Nigeria. Trop Geogr Med 1978;30(3):313-324. [ Links ]
19. Huff R. Normal blood pressure values in children. http://www.ehow.com/about5571920 (accessed 30 November 2013). [ Links ]
20. Ogunkunle O, Odutola A, Orimadegun A. Pattern of blood pressure in apparently healthy Nigerian children aged 1 - 5 years. Niger J Paediatr 2007;34(1&2):14-23. [ Links ]
21. Collins S. Changing the way we address severe malnutrition during famine. Lancet 2001;358(9280):498-501. [http://dx.doi.org/10.1016/S0140-6736(01)05630-6] [ Links ]
22. Kaplan NM, Devereux RB, Miller HS. Task Force 4: Systemic hypertension. J Am Col Cardiol 1994:24(4);885-888. [ Links ]
 Correspondence:
Correspondence:
JM Chinawa
(josephat.chinawa@unn.edu.ng)

