










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Child Health
versión On-line ISSN 1999-7671
versión impresa ISSN 1994-3032
S. Afr. j. child health vol.8 no.2 Pretoria may. 2014
CASE REPORT
Riga-Fede disease (Cardarelli's aphthae): a report of nine cases
R P S MohanI; S VermaII; N GillIII; U SinghIV
IMDS; Subharti Dental College, Meerut, India
IIMDS; Kothiwal Dental College and Research Centre, Moradabad, India
IIIMDS; College of Dental Sciences, Bopal, Ahmedabad, India
IVBDS; Kothiwal Dental College and Research Centre, Moradabad, India
ABSTRACT
We report nine cases of traumatic oral mucosal lesions (Riga-Fede disease or Cardarelli's aphthae) caused by natal teeth, and provide a brief review of the literature. Seven patients were treated with a conservative approach involving grinding of the sharp incisal edges, while extraction of the offending teeth was considered necessary in the other two cases. Triamcinolone was applied in all nine cases. At follow-up, all the lesions were healing and the infants had resumed painless feeding.
Traumatic oral granuloma, also known as Riga-Fede disease or Cardarelli's aphthae, is a rare, benign, ulcerative, granulomatous process that occurs as a result of repetitive trauma of the oral mucosal surfaces by the teeth.[1] The lesion is named after Antonio Riga, who first identified it in 1881,[2] and Fede, who later described more cases and performed histological studies.[3]
Natal teeth are present at birth, while neonatal teeth are those that erupt in the first month of life.[4] The teeth can either be prematurely erupting normal teeth (up to 95% of cases) or supernumerary teeth (5%).[5] Riga-Fede disease is frequently associated with natal and neonatal teeth, occurring in 6 - 10% of patients with natal teeth.[6] It may also occur in older infants after eruption of the primary lower incisors.[7] It is important to keep in mind that traumatic oral granuloma can be an initial presentation of a serious underlying medical problem such as Lesch-Nyhan syndrome or familial dysautonomia.[1]
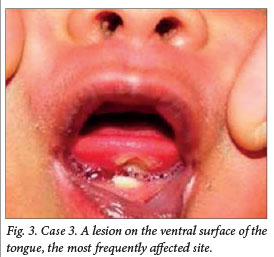
We report nine cases of Riga-Fede disease, recorded over a period of 10 years from 2002 to 2012. Five lesions occurred at the characteristic site in the oral cavity, the ventral surface of the tongue, and four at different sites (the internal mucosa of the lower lip, and the tip and lateral surfaces of the tongue). Here we discuss treatment and present a brief review of the literature.
Case reports
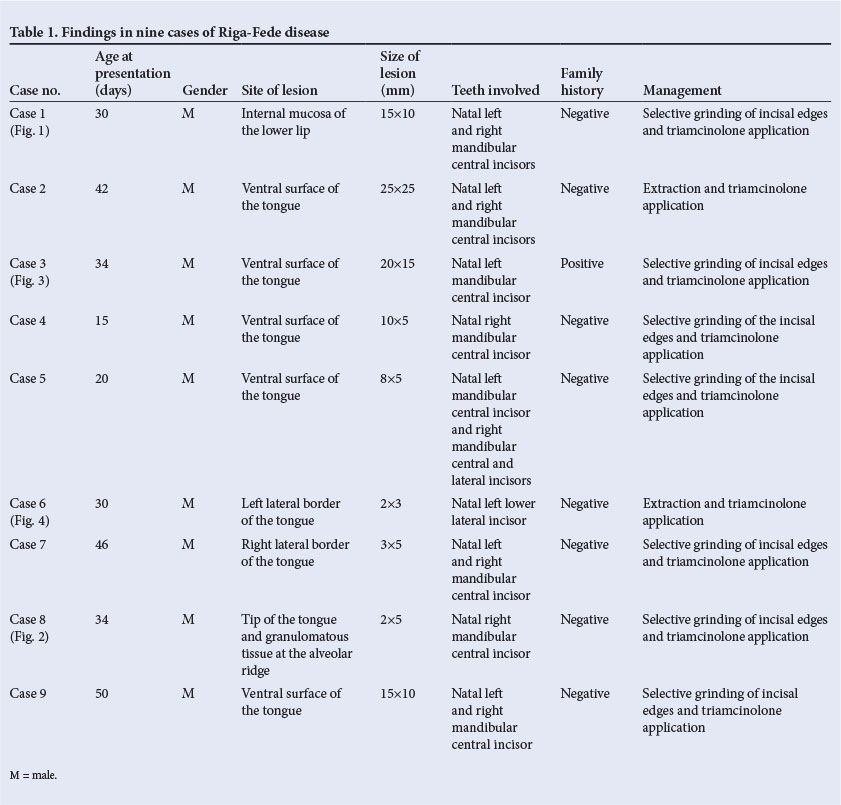
The findings in our nine cases are presented in Table 1. In all cases the natal teeth causing traumatic oral ulceration were mandibular incisors - these tend to be responsible because they are normally the irst teeth to erupt in the oral cavity.[8] Figs 1 - 4 illustrate the variable presentation of the ulcers. The labial inclination of the natal teeth in our first case resulted in development of a traumatic ulcer on the labial mucosa of the lower lip, sparing the tongue (Fig. 1). Granulomatous tissue at the alveolar ridge along with an ulcer at the tip of tongue was seen in another case (Fig. 2). In ive cases the lesion was on the ventral surface of the tongue, which is the most frequently affected site (Fig. 3). Two patients had ulceration on the lateral surface of the tongue, coinciding with the distally inclined crown of the lower incisor (Fig. 4).



Discussion
Riga-Fede disease is a rare disease characterised by traumatic ulceration that gives rise to a consistent, greyish, granulomatous plaque with well-defined borders, located on the ventral surface of the tongue or the internal mucosa of the lower lip.[1] The lesion is caused by repeated trauma by teeth, especially the lower incisors[9] together with the sucking reflex and the tendency for the infant's tongue to protrude.[7] Natal teeth have been reported to be more common in females, but Riga-Fede disease has a slight male predilection[8,10] All nine of our patients were males. A positive family history for natal teeth has been reported in 8 - 62% of cases,[8] but only one of our patients had such a history.
According to the classification proposed by Domingues-Cruz et al.,[9] Riga-Fede disease can be separated into the precocious type, caused by natal or neonatal teeth, and late disease, with onset after 6 - 8 months of age when the lower incisors erupt. Late Riga-Fede disease can be associated with neurological disorders,[9] whereas there is no relationship with neurological disease in the precocious type seen in the first 6 months of life. All nine of our cases were of the latter type, since the lesions were caused by natal teeth; also, all of our patients were aged <6 months, and none had associated neurological disorders.
It is important to recognise this condition, as it can be the first sign of severe neurological disorders related to self-mutilation such as familial dysautonomia (insensitivity to pain), congenital indifference to pain, Lesch-Nyhan syndrome or Tourette's syndrome. Neurological evaluation is therefore essential in affected children.[11] All of our patients were referred to a neurologist for assessment before treatment, but no abnormalities were found.
The differential diagnosis of Riga-Fede disease includes infectious diseases such as syphilis, tuberculosis or ulcerative candidiasis, and neoplasms such as lymphomas, sarcomas or granular cell myoblastomas[11,12] Biopsy is important to exclude some of the above if they are suspected. Histologically, Riga-Fede disease is described as mucosal ulceration with granulation tissue and mixed inflammatory infiltrate with a majority of eosinophils[11] We did not consider an invasive procedure such as a biopsy to be necessary in any of our patients in view of their age, the sites of the lesions, the typical clinical findings, and the fact that all improved after treatment.
Treatment of Riga-Fede disease aims to minimise trauma, and extraction is not generally indicated. Early extraction of a primary natal tooth can lead to overcrowding of the permanent teeth.[8] The preferred treatment is a conservative approach involving smoothing of the sharp incisal edges of the offending teeth or placing domes of composite resin over the incisal edges. Modifying the feeding method in order to reduce trauma is also effective. This can be achieved by using a bottle with a larger hole in the teat, or placing a nasogastric tube in patients with more extensive lesions.[13]
We treated seven of our patients by grinding the incisal edges, but opted for extraction in two, owing to the mobility of their natal teeth, which we thought could pose the risk of the teeth falling out during feeding and being swallowed or aspirated.[7] In all patients, symptoms were relieved with triamcinolone, to minimise the inflammatory process, and an emollient.
In conclusion, traumatic ulceration caused by natal or neonatal teeth is very unusual. Awareness of the condition is essential for proper diagnosis and management. Failure to diagnose these lesions may lead to deformity or mutilation of the tongue, dehydration and inadequate nutrient intake, with resulting medical sequelae.
References
1. Choi SC, Park JH, Choi YC, Kim GT. Sublingual traumatic ulceration. Riga-Fede disease: Report of two cases. Dent Traumatol 2009;25(3):e48-e50. [http://dx.doi.org/10.1111/j.1600-9657.2009.00773.x] [ Links ]
2. Hegde RJ. Sublingual traumatic ulceration due to neonatal teeth (Riga-Fede disease). J Indian Soc Pedod Prev Dent 2005;23(1):51-52. [http://dx.doi.org/10.4103/0970-4388.16031] [ Links ]
3. Baroni A, Capristo C, Rossiello L, Faccenda F, Satriano RA. Lingual traumatic ulceration (Riga-Fede disease). Int J Dermatol 2006;45(9):1096-1097. [http://dx.doi.org/10.1111/j.1365-4632.2004.02554.x] [ Links ]
4. Ghom AG. Textbook of Oral Medicine. 2nd ed. New Delhi: Jaypee Brothers, 2010:127-128. [ Links ]
5. Sureshkumar R, McAulay AH. Natal and neonatal teeth. Arch Dis Child Fetal Neonatal Ed 2002;87(3):227. [http://dx.doi.org/10.1136/fn.87.3.F228] [ Links ]
6. Buchanan S, Jenkins CR. Riga-Fede syndrome: Natal or neonatal teeth associated with tongue ulceration: Case report. Aust Dent J 1997;42:225-227. [http://dx.doi.org/10.1111/j.1834-7819.1997.tb00125.x] [ Links ]
7. Baghdadi ZD. Riga-Fede disease: Association with microcephaly. Int J Paediatr Dent 2002;12(6):442-445. [http://dx.doi.org/10.1046/j.1365-263X.2002.00396.x] [ Links ]
8. Leung AKC, Robson WLM. Natal teeth: A review. J Natl Med Assoc 2006;98(2):226-228. [ Links ]
9. Domingues-Cruz J, Herrera A, Fernandez CP, Garcia BB, Camacho F. Riga-Fede disease associated with postanoxic encephalopathy and trisomy 21: A proposed classification. Pediatr Dermatol 2007;24(6):663-665. [http://dx.doi.org/10.1111/j.1525-1470.2007.00564.x] [ Links ]
10. Rao RS, Mathad SV. Natal teeth: Case report and review of literature. J Oral Maxillofac Pathol 2009;13(1):41-46. [http://dx.doi.org/10.4103/0973-029X.44574] [ Links ]
11. Narang T, De D, Kanwar AJ. Riga-Fede disease: Trauma due to teeth or tongue tie? J Eur Acad Dermatol Venereol 2008;22(3):395-396. [http://dx.doi.org/10.1111/j.1468-3083.2007.02347.x] [ Links ]
12. Santos Cunha V, Zanol JDR, Sprinz E. Riga-Fede-like disease in an AIDS patient. J Int Assoc Provid AIDS Care 2007;6(4):273-274. [http://dx.doi.org/10.1177/1545109707304299] [ Links ]
13. Campos-Munoz L, Quesada-Cortes A, Corral-De la Calle M, et al. Tongue ulcer in a child: Riga-Fede disease. J Eur Acad Dermatol Venereol 2006;20(10):1357-1359. [http://dx.doi.org/10.1111/j.1468-3083.2006.01715.x] [ Links ]
 Correspondence:
Correspondence:
R P S Mohan
(sasan_ravi@rediffmail.com)


{kind=link}