










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.8 no.1 Pretoria Fev. 2014
RESEARCH
Whose child is dying? Household characteristics and under-5 mortality in Nigeria
C Izugbara
BSc, MSc, BA; Human Economy Programme, University of Pretoria, South Africa
ABSTRACT
BACKGROUND: Over 2 000 under-5-year-olds die daily in Nigeria from vaccine-preventable diseases, placing the country as the third largest contributor to the global under-5 mortality rate. Nigeria is at serious risk of not meeting the Millennium Development Goal (MDG) of reducing child mortality by two-thirds (i.e. from an under-5 mortality rate of 93/1 000 in 1990 to 31/1 000 in 2015).
OBJECTIVE: To examine the association between household-level variables and under-5 mortality in Nigeria.
METHODS: Data were drawn from the 2008 Nigeria Demographic and Health Survey, which elicited information on demographic and health indicators at the national and state levels. A nationally representative sample of 36 800 households was selected. Data were collected from 33 385 women of reproductive age (15 - 49 years) and who had given birth to at least one live infant in the 5 years preceding the survey. Data were analysed using a multilevel-model approach.
RESULTS: In total, there were 104 808 live births; 18 121 (17.29%) children died as under-5s and 86 687 (82.71%) survived. Poverty, number of children ever born in a household, number of under-5s in the household, place and region of residence, maternal and paternal age, and maternal and paternal education level were critical determinants of under-5 mortality.
CONCLUSION: The rate of under-5 mortality remains high in Nigeria. This will not be resolved until household-focused interventions are implemented using a tailored framework, and the need to improve maternal education in the country is addressed.
Globally, Nigeria is the second largest contributor to under-5 mortality.[1-3] Currently, over 2 000 under-5s die daily in the country (about four million annually) from vaccine-preventable diseases, despite advances in universal immunisation and oral rehydration therapy (ORT) for diarrhoeal disease.[4] This places Nigeria as one of the largest contributors to the under-5 mortality rate in the world. Recent trends show that Nigeria is making progress in slowing its under-5 mortality rate, but the pace of reduction remains far too slow to achieve the 2015 Millennium Development Goal of reducing child mortality by two-thirds. This assertion is made evident by a recent study[6] indicating that Nigeria is 28.6% away from the target of reducing under-5 mortality from 93/1 000 in 1990 to 31/1 000 in 2015.
Though various reforms and policies have been put forward by the Nigerian government to address wide-ranging issues in the healthcare system, these are yet to yield expected results, and the majority are yet to be implemented at local government level.[2] Data from the POLICY project[9] indicate that the healthcare system in Nigeria is weak, as evidenced by a lack of coordination, a fragmentation of services, a dearth of resources including medicines and supplies, inadequate and decaying infrastructure, inequity in resource distribution, poor access to care and the deplorable quality thereof.
Existing research on the predictors of under-5 mortality has paid little attention to household-level factors, while great emphasis has been placed on factors such as diarrhoea, malaria, measles, acute respiratory infections, whooping cough, tuberculosis, bronchopneumonia, dirty feeding bottles and utensils, inadequate disposal of household refuse and poor storage of drinking water.[10-14] A number of studies have shown that under-5 mortality rates vary according to socioeconomic and biodemographic characteristics. For instance, women with little or no education,[15-18] women in a lower wealth quintile,[19,20] women who reside in rural areas,[20] women in polygamous unions,[21] women who have poor or no access to electricity,[20] women who delay initiation of breastfeeding,[22] and women who did not complete child immunisation[20] tend to have children with a higher under-5 mortality rate. Nigerian studies have overemphasised the influence of individuallevel factors in under-5 mortality,[23-26] and several studies have been largely hospital-based.[27-32] In this study the levels and influences of contextual determinants of under-5 mortality in Nigeria were explored using a multilevel-model approach. Specifically, the associations between household-level variables and under-5 mortality were explored.
Methods
Data were drawn from the 2008 Demographic and Health Survey in Nigeria,[35] which represents the most comprehensive of demographic and health surveys conducted in the country. The survey was conducted from June to October 2008 by the National Population Commission (NPC), with financial support from the United States Agency for International Development (USAID) and the United Nations Population Fund (UNFPA). Technical assistance was provided by ICF Macro International. Questionnaires were administered on a nationally representative sample of 36 000 households drawn from all 36 states and the Federal Capital Territory.[36]
The 2008 Demographic and Health Survey elicited information on demographic and health indicators at the national and state levels.[35] A nationally representative sample of 36 800 households was selected. Data were collected from 33 385 women of reproductive age (15 - 49 years) and who had given birth to at least one live infant in the 5 years preceding the survey (2003 - 2008). For the purposes of the study, under-5 mortality was defined as the number of deaths in infants and children under the age of 5 years per 1 000 live births.[37]
Statistical analysis
Univariate analyses were performed and bivariate associations were examined between under-5 mortality and individual-, household-, and community-level variables. Household characteristics and sociodemographic variables considered were: maternal and paternal age, maternal and paternal education level, household wealth index, age and gender of the household head, family size, and which parent was the household decision-maker. Associations were determined by computing odds ratios (ORs) with 95% confidence intervals (CIs). Variables that were significant at this level were entered into a multivariate logistic regression model to estimate adjusted ORs (AORs) and corresponding 95% CIs. Three models were developed: the first examined the net relationship between individual-level factors associated with under-5 mortality; the second combined selected household- and community-level factors; and the third combined selected individual- and household-level factors.
Results
Of a total of 104 808 live births in the 5-year period surveyed (2003 - 2008), 86 687 children reportedly survived (82.71%) and 18 121 (17.29%) died under the age of 5 years.
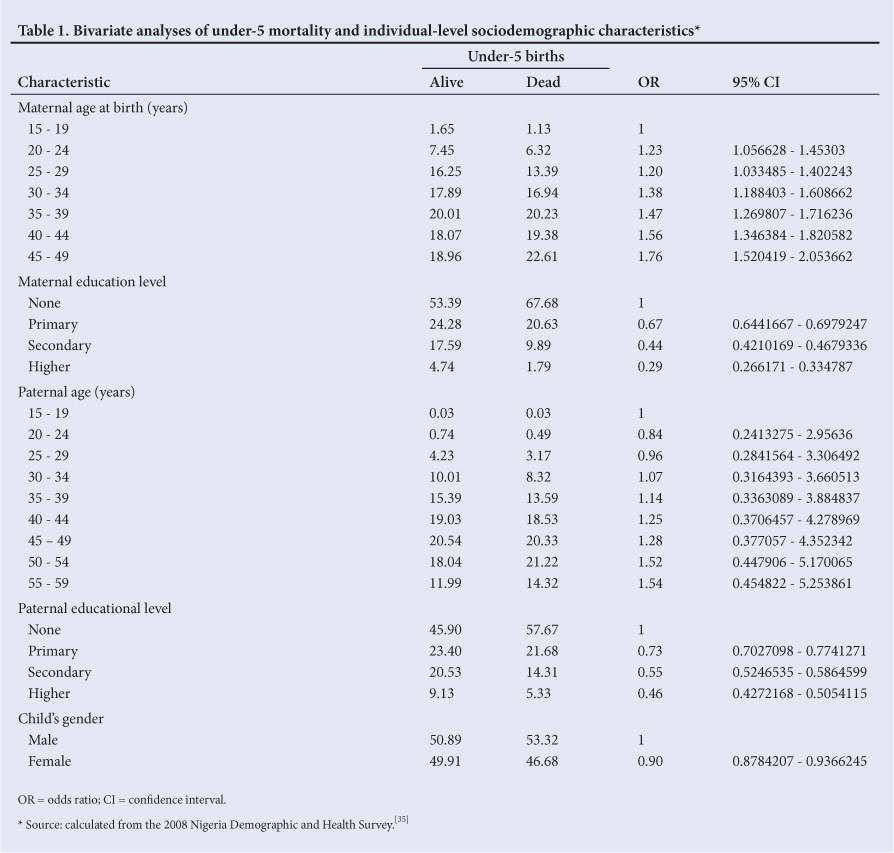
In the bivariate analysis of under-5 mortality and sociodemographic variables at the individual level (Table 1), the occurrence of under-5 deaths varied significantly with maternal and paternal age, maternal and paternal educational level, and child gender. Women aged >45 - 49 years experienced the highest rate of under-5 mortality among their children (1.76 times more likely to experience such mortality than those aged 15 - 19 years). Under-5 mortality was also higher among children of older fathers. Higher levels of maternal education were associated with a lower likelihood of reporting under-5 deaths in children; 67.68% of child deaths were experienced by women who had no form of education, and only 1.79% were experienced by women with a higher education level (OR 0.29; 95% CI 0.266 - 0.335). Similarly, with regard to paternal education level, under-5 mortality was highest among children whose fathers had no form of education, with an OR of 0.46 (95% CI 0.427 - 0.505) for under-5 mortality in children of fathers with academy- or university-level education. In terms of child gender, a higher rate of mortality (53.32%) was reported for male under-5s than for female under-5s (46.68%; OR 0.9; 95% CI 0.878 - 0.937).
An analysis of variables at the household level revealed that the age and gender of household heads, the number of under-5 children in the household and the number of children ever born (CEB) were significantly associated with under-5 mortality (Table 2). Female-headed households were less likely to experience under-5 mortality than male-headed households (OR 0.81; 95% CI 0.761 - 0.865). Households with a higher number of under-5s were more likely to experience under-5 mortality, and the higher the number of CEB to a household, the more likely the household was to experience such mortality.
Type of floor, place and region of the household residence were significantly associated with under-5 mortality (Table 3). Households with cement floors were less likely to experience under-5 mortality than those with earth or sand floors. Rural households were more likely to experience under-5 mortality than their urban counterparts (OR 1.5; 95% CI 1.427 - 1.579).
In terms of wealth status, households in the lowest wealth quintile had the highest rate of under-5 mortality. Those from the richest quintile had an OR of 0.32 (95% CI 0.306 - 0.351). The northwest geopolitical zone of Nigeria experienced the highest rate of mortality among under-5 children (Table 3).
Multivariate analysis
When all variables at the individual, household and community levels were controlled simultaneously, household wealth index, region of residence, number of under-5s in the household, number of CEB, number of living children, child gender and maternal and paternal education level were significantly associated with under-5 mortality (Tables 4 -6). Female children were also less likely to die before the age of 5 years than male children.
Discussion
This study focused on household-level factors associated with under-5 mortality in Nigeria. Using bivariate analysis to examine the level of the relationship between the dependent and independent variables, the findings confirmed that maternal and paternal age were significantly associated with under-5 mortality. With regard to parental education level, under-5 mortality occurred more frequently in households whose fathers or mothers had no form of education. Analysis of the variables at the household level revealed that age and gender of the household head, number of under-5 children in the household and number of CEB were factors significantly associated with under-5 mortality. Households headed by older adults reported higher rates of under-5 mortality than households headed by younger adults. Female-headed households were less likely to experience mortality among under-5 children than male-headed households. Place and region of residence were significantly associated with under-5 mortality. Households with a cement floor were less likely to experience under-5 mortality than households with residence floors comprised of earth or sand. Rural households were more likely to experience under-5 mortality than their urban counterparts. Households of the lowest wealth quintile reported the highest rate of under-5 mortality compared with all other quintiles. Households with three or more under-5 children were more likely to experience under-5 mortality than households with fewer than three under-5s.
Results emerging from the multivariate logistic regression analysis show that maternal and paternal education, number of under-5 children in the household, number of CEB, socioeconomic status of the household, age of the household head, and region and place of residence had the greatest effect on under-5 mortality.
The relationship between maternal education level and childhood mortality (infant and under-5s) has received considerable attention.[40,41] The findings of this study add to this body of extant literature. Results from both the bivariate and multivariate regression analyses show that education generally acts to reduce mortality among under-5s. Not only was maternal education shown to have a significant association with under-5 mortality in our study, but paternal education also proved to be associated with a considerably lower risk of this mortality in households where the level of paternal education obtained was at the university or college level. This supports previous studies showing that maternal and paternal education are among the most important factors associated with infant survival.[33,42]
The findings also showed higher mortality rates among under-5s in rural areas and the northwest geopolitical zones. This supports Antai's[33] argument that cities and towns tend to have lower mortality rates than rural areas, possibly because people residing in rural areas are less educated than their urban counterparts and the distribution of amenities is lopsided in favour of the urban areas.[33] The results of this study showed that household wealth quintile was a significant predictor of under-5 mortality. Earlier studies showed a higher incidence of malnutrition and thus of morbidity and mortality among children of a lower wealth quintile than among children of the wealthiest quintile.[45,46]
Study limitations
Mortality studies are generally faced with data limitations, particularly in developing countries. Death is regarded as a sad event that respondents are reluctant to recall: 'Mothers may be reluctant to talk about their dead children either because it brings back sad memories or because their culture discourages mention of the dead.[36] The study drew on a cross-sectional secondary dataset; as a result, there was a tendency for child deaths to be underreported. As can the omission of deaths affect mortality data, so can the misreporting of age at death (heaping or avoidance) distort the age pattern of such data. Also, because data on child births and deaths were collected retrospectively, the number of births and child deaths might have been underreported due to memory lapse. Nonetheless, it is not envisaged that the data limitations posed a serious challenge to this study.
Conclusions and recommendations
The findings of this study have expanded on earlier research that implicated malnutrition, infection, dehydration and diarrhoea in under-5 mortality in Nigeria. The study calls for attention to household-focused interventions tailored alongside the need to improve maternal education to address the scourge of childhood mortality. Older adult parents should be encouraged to seek medical attention whenever the need arises in their under-5 children. There is also a need for further, more in-depth studies into household-level factors associated under-5 mortality.
References
1. Rutherford ME, Mulholland K, Hill PC. How access to health care relates to under-five mortality in sub-Saharan Africa. Top Med Int Health 2010;15(5):508-519. [http://dx.doi.org/10.1111/j.1365-3156.2010.02497.x] [ Links ]
2. US Central Intelligence Agency. The World Fact Book. https://www.cia.gov/library/publications/the-world-factbook/geos/ni.html (accessed 1 June 2013). [ Links ]
3. UNICEF. The State of the World's Children. New York: UNICEF, 2011. [ Links ]
4. World Bank. World Bank Development Indicators Database. http://www.data.worldbank.org (accessed 6 September 2011). [ Links ]
5. Palma-Solís MA, Alvarez-Dardet Díaz C, Franco-Giraldo A, et al. State downsizing as a determinant of infant mortality and achievement of Millennium Development Goal 4. Int J Health Serv 2009;39(2):389-403. [ Links ]
6. United Nations. Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat, World Population Prospects: The 2010 Revision. Geneva: UN, 2010. http://esa.un.org/unpd/wpp/index.htm (accessed 1 June 2013). [ Links ]
7. Ekenze SO, Anyanwu KK, Chukwumam DO. Childhood trauma in Owerri (South Eastern) Nigeria. Niger J Med 2009;18(1):79-83. [ Links ]
8. World Health Organization. Protecting, Promoting and Supporting Breastfeeding: The Special Role of Maternity Services; A Joint WHO/UNICEF Statement. Geneva: WHO, 2012. [ Links ]
9. POLICY Project/Nigeria. Reproductive Health in Nigeria, Situation, Response, and Prospects: Key Issues. Abuja: POLICY Project, 2011. [ Links ]
10. Ogunjuyigbe P. Under-five mortality in Nigeria: Perception and attitudes of the Yorubas towards the existence of 'Abiku". Demographic Research 2004;11(2):43-56. [ Links ]
11. Rodgers GB. Income and inequality as determinants of mortality: An international cross-section analysis. Int J Epidemiol 2002;31:533-538. [ Links ]
12. Hargreaves S. Time to right the wrongs: Improving basic health care in Nigeria. Lancet 2002;359(9322):2030-2035. [http://dx.doi.org/10.1016/S0140-6736(02)08826-8] [ Links ]
13. Anyamele OD. Urban and rural differences across countries in child mortality in sub-Saharan Africa. J Health Care Poor Underserved 2009;20(Suppl 4):90-98. [ Links ]
14. Berger U, Fahrmeir L, Klasen S. Dynamic Modelling of Child Mortality in Developing Countries: Application for Zambia. Munich: Ludwig-Maximilians-Universität, 2002:386. [ Links ]
15. Kanjala C, Alberts M, Byass P, Burger S. Spatial and temporal clustering of mortality in Digkale HDSS in rural northern South Africa. Global Health Action 2010;3(Suppl 1):59-63. [ Links ]
16. Schell CO, Reilly M, Rosling H, Peterson S, Ekstrom AM. Socioeconomic determinants of infant mortality: A worldwide study of 152 low-, middle-, and high-income countries. Scan J Public Health 2007;35:288-297. [http://dx.doi.org/10.1080/14034940600979171] [ Links ]
17. Griffiths P, Madise N, Whitworth A, Mathew Z. A tale of two continents: A multilevel comparison of the determinants of child nutritional status from selected African and Indian regions. Health Place 2004;10:183-199. [ Links ]
18. Sastry N. What explains rural-urban differentials in child mortality in Brazil? Soc Sci Med 1997;44(7):989-1002. [ Links ]
19. Harttgen K, Misselhorn M. A multilevel approach to explain child mortality and undernutrition in South Asia and sub-Saharan Africa. Ibero-America Institute for Economic Research Papers 2006;156:1-38. [ Links ]
20. Wang L. Determinants of child mortality in LDCs: Empirical findings from demographic and health surveys. Health Policy 2003;65:277-299. [ Links ]
21. Omariba DWR, Boyle MH. Family structure and child mortality in sub-Saharan Africa: Cross-national effects of polygyny. Journal of Marriage and Family 2007;69:528-543. [http://dx.doi.org/10.1111/j.1741-3737.2007.00381.x] [ Links ]
22. Grais RF, Dubray C, Gerstl S, et al. Unacceptably high mortality related to measles epidemics in Niger, Nigeria, and Chad. PLoS Med 2007;4(1):e16. [http://dx.doi.org/10.1371/journal.pmed.0040016] [ Links ]
23. Anyamele OD. Urban and rural differences across countries in child mortality in sub-Saharan Africa. J Health Care Poor Underserved 2009;20(Suppl 4):90-98. [ Links ]
24. Nwokocha EE, Awomoyi AO. Factors influencing mothers' role in convulsion treatment among under-five children in Ibadan, Nigeria. World Health Popul 2009;11(2):15-29. [ Links ]
25. Ekenze SO, Anyanwu KK, Chukwumam DO. Childhood trauma in Owerri (South Eastern) Nigeria. Niger J Med 2009;18(1):79-83. [ Links ]
26. Okoro PE, Igwe PO, Ukachukwu AK. Childhood burns in south eastern Nigeria. Africa J Paeditr Surg 2009;6(1):24-27. [ Links ]
27. Akinbami FO, Hamzat TH, Orimadegun AE, et al. Body mass composition: A predictor of admission outcomes among hospitalized Nigerian under 5 children. Asia Pac J Clin Nutr 2010;19(3):295-300. [ Links ]
28. Adeboye MA, Ojuawo A, Ernest SK, Fadeyi A, Salisu OT. Mortality pattern within twenty-four hours of emergency paediatric admission in a resource-poor nation health facility. West Afr J Med 2010;29(4):249-252. [ Links ]
29. Babalola S, Fatusi A. Determinants of use of maternal health services in Nigeria - looking beyond individual and household factors. BMC Pregnancy Childbirth 2009;9(1):43. [ Links ]
30. Brown BJ, Bamgboye EA, Sodeinde O. Causes of death in childhood cancer at the Department of Paediatrics, University College Hospital, Ibadan. Africa J Med Sci 2008;37(1):7-13. [ Links ]
31. Udo JJ, Anah MU, Ochigbo SO, Etuk IS, Ekanem AD. Neonatal morbidity and mortality in Calabar, Nigeria: A hospital-based study. Niger J Clin Prac 2008;11(3):285-289. [ Links ]
32. Oniyangi O, Awani B, Iregbu KC. The pattern of paediatric HIV/AIDS as seen at the National Hospital Abuja, Nigeria. Niger J Clin Prac 2006;9(2):153-158. [ Links ]
33. Antai D. Inequalities in under-5 mortality in Nigeria: Do ethnicity and socioeconomic position matter? J Epidemiol 2011;21(1):13-20. [ Links ]
34. Antai D, Moradi T. Urban area disadvantage and under-5 mortality in Nigeria:-The effect of rapid urbanization. Environ Health Perspect 2010;118(6):877-883. [http://dx.doi.org/10.1289/ehp.0901306] [ Links ]
35. National Population Commission (NPC), ORC Macro. Nigeria 2008 Demographic and Health Survey 2008: Key Findings. Calverton, Maryland: NPC and ORC Macro, 2009. [ Links ]
36. National Population Commission (NPC), ORC Macro (2012). [ Links ]
37. United Nations Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat. World Population Prospects: The 2010 Revision. http://esa.un.org/unpd/wpp/index.htm (accessed 1 June 2013). [ Links ]
38. Becher H. Analyses of mortality clustering at member HDSSs within the INDEPTH Network - an important public health issue. Global Health Action 2010;3(Suppl 1):3-7. [ Links ]
39. Antai D. Regional inequalities in under-5 mortality in Nigeria: A population-based analysis of individual- and community-level determinants. Popul Health Metr 2011;9(6):1-27. [ Links ]
40. Hammer GP, Some F, Muller O, Kynast-Wolf G, Kouyate B, Becher H. Pattern of cause-specific childhood mortality in a malaria endemic area of Burkina Faso. Malar J 2006;5:47. [ Links ]
41. Zanini RRB, Moraes AJ, Giugliani ER, Riboldi J. Infant mortality trends in the State of Rio Grande do Sul, Brazil, 1994 - 2004: A multilevel analysis and community risk factors. Cad Saude Publica 2009;25(5):1035-1045. [ Links ]
42. Rutstein S. Effect of Birth Intervals on Mortality and Health - Multivariate Crosscountry Analyses with Additional Information for Nigeria. Washington: USAID, 2001. [ Links ]
43. Dike N, Onwujeke O, Ojukwu J, Ikeme A, Uzochukwu B, Shu E. Influence of education and knowledge on perceptions and practices to control malaria in southeast Nigeria. Soc Sci Med 2006;63(1):103-106. [ Links ]
44. Whitworth A, Stephenson R. Birth spacing, sibling rivalry and child mortality in India. Soc Sci Med 2002;55:2107-2119. [ Links ]
45. Wall L. Dead mothers and injured wives: The social context of maternal morbidity and mortality among the Hausa of northern Nigeria. Studies in Family Planning 1998;29(4):341-359. [ Links ]
46. Uthman AO. A multilevel analysis of individual and community effect on chronic childhood malnutrition in rural Nigeria. J Trop Pediatric 2009;55(2):109-115. [ Links ]
 Correspondence:
Correspondence:
C Izugbara
(cizugbara@yahoo.com)


{kind=link}
{kind=link}
{kind=link}