










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.8 n.1 Pretoria Feb. 2014
RESEARCH
Predictors of prolonged hospitalisation in childhood pneumonia in a rural health centre
B P KutiI; S A AdegokeI; O A OyelamiII; M O OtaIII
IMB ChB, FWACP; Department of Paediatrics and Child Health, Obafemi Awolowo University, Ile-Ife, Nigeria
IIMBBS, FWACP, FRCP (Edinburgh); Department of Paediatrics and Child Health, Obafemi Awolowo University, Ile-Ife, Nigeria
IIIMBBS, FWACP, PhD, MD; Medical Research Council, Gambian Unit, Atlantic Bouvelard, Fajara, The Gambia
ABSTRACT
BACKGROUND: Pneumonia is a major cause of morbidity and mortality in under-5 children. Caring for children with pneumonia, especially in the case of prolonged hospitalisation, is a daunting task in resource-poor countries where caregivers are required to pay for treatment 'out of pocket' at the point of care. These children are often discharged against medical advice with incomplete treatment, with a consequent high rate of re-admission and complications.
OBJECTIVE: To determine factors that predict prolonged hospitalisation among under-5 children with severe pneumonia admitted to a comprehensive health centre in rural Gambia.
METHODS: We prospectively assessed 420 consecutive under-5 admissions with severe pneumonia, diagnosed using World Health Organization criteria, for factors in patient history, examination or investigations that could predict a hospital stay longer than 5 full days.
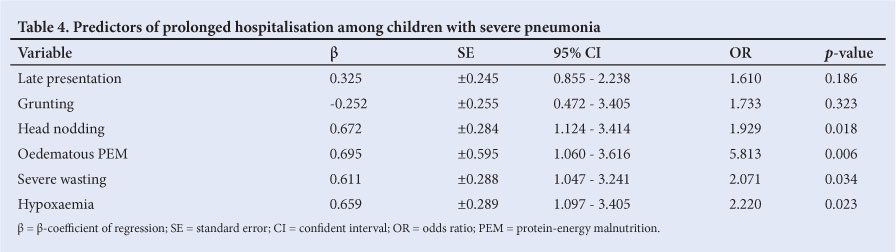
RESULTS: Over the 6-month study period, pneumonia accounted for 27.6% of the total number of under-5 admissions. The mean age of children with pneumonia was 18.0 months (standard deviation (SD) ±13.7), there was a male to female ratio of 1.2:1, and 40.0% of the children were infants. Their mean hospital stay was 4.5 (SD ±3.0) days and 105 (25.0%) of the children had a prolonged hospital stay. Head nodding (odds ratio (OR) 1.929; 95% confidence interval (CI) 1.124 - 3.414; p=0.018), the presence of oedematous protein-energy malnutrition (OR 5.813; CI 1.060 - 3.616; p=0.006), severe wasting (OR 2.071; CI 1.047 - 3.241; p=0.034) and hypoxaemia at presentation (OR 2.220; CI 1.097 - 3.405; p=0.023) were independent predictors of prolonged hospital stay.
CONCLUSION: Caregivers of children hospitalised with pneumonia and severe wasting, head nodding, oedema or hypoxaemia should be counselled at admission about the possibility of prolonged hospitalisation.
Childhood pneumonia is a leading cause of morbidity and mortality among under-5 children, especially in developing countries where the majority of people are low-income earners.[1,2] Pneumonia is responsible for approximately one-fifth of deaths among under-5s globally.[2] It is also a major reason for hospital admission among children, particularly in resource-poor areas.[1-3]
A prime goal of clinical assessment is the detection of severe disease episodes in children, on the assumption that these children will benefit from treatment and will be discharged from the health facility well and without sequelae.[4] It is commonly acceptable that death, as the most severe consequence of disease, is an important outcome.[5-8] Other major parameters for assessing the severity of pneumonia include prolonged hospitalisation,[8] which has an overbearing effect on the hospitalised child, as well as on the family.[8,9]
A report from the US Centers for Diseases Control and Prevention estimated that the average length of hospital stay for treatment of pneumonia in children aged <15 years (excluding neonates) is 5 days.[10] Any hospital stay exceeding 5 days is considered to be prolonged.[8,10] Caring for a child with pneumonia may be financially burdensome in resource-poor areas, particularly when in-hospital treatment is required for a prolonged period.[11-13] This is even more relevant in situations where caregivers have to pay 'out of pocket' for patient care.[9,11-13] Estimates show that the average daily cost of in-patient care for under-5s with severe pneumonia in health facilities in developing countries is beyond the reach of average low-income earners if unsubsidised.[11-13] Many a time, children are discharged against medical advice (DAMA), often for financial reasons, and sometimes due to burnout on the part of caregivers or a perceived lack of clinical improvement. [14] The caregiver may then opt to seek alternative, unorthodox and cheaper care elsewhere, which is often ineffective, with consequential high rates of re-admission, development of complications or mortality.[15-17]
There are a number of published studies on the predictors of childhood pneumonia-related mortality;[5-7] however, few were conducted in rural settings, and predictors of morbidity such as prolonged hospital stay were not considered in most. The simple predictors of prolonged hospital stay in childhood pneumonia may assist in counselling parents on the likely duration of hospitalisation. This will enable them to mobilise resources for the hospital care of the child and re-adjust to any disruption that the admission may cause. This may reduce the incidence of DAMA, thereby ensuring adequate management.
We set out to highlight features at presentation that could predict prolonged hospitalisation in under-5s with severe pneumonia admitted to a rural comprehensive health centre.
Methods
This was a prospective, observational study carried out at the paediatric ward of the Basse Major Health Centre, The Gambia, from November 2010 to April 2011. The Health Centre is a rural comprehensive health centre serving as a referral health facility for the 225 adjoining villages in Basse.[18]
Children recruited were those aged 2 - 59 months admitted with difficult or fast breathing, defined as a respiratory rate >50 cycles/min in the first year of life and >40 cycles/min in those aged 1 - 5 years. In addition to fast breathing, the children had at least one of: nasal flaring; lower chest wall in-drawing; cyanosis; altered sensorium; and inability to suck or feed.[4] Children with a cough persisting for >2 weeks as well as those with audible and/or auscultatory wheeze (rhonchi) were excluded to reduce the chances of recruiting children with pulmonary tuberculosis (PTB) and bronchiolitis/bronchial asthma, respectively.
We recorded the details including outcomes of all consecutive children aged 2 - 59 months admitted during the study period. Those who fulfilled the above inclusion criteria were active study participants.
Relevant sociodemographic data, including age and gender, were obtained from the study participants. The number of persons who co-habited and slept in the same room as the child was noted for the purpose of the study, and overcrowding was defined as having three or more persons sleeping in the same room with the child.[19] The immunisation status of participants (whether appropriately immunised for age based on the Gambian National Programme on Immunization schedule) was also noted.
The history of the presenting illness - e.g. fever, cough, fast or difficult breathing and duration - was noted. Associated symptoms such as an inability to suck or feed, diarrhoea, vomiting and convulsion were also noted. Those who presented for treatment within 3 days of the onset of symptoms were classified as early presenters, while those who presented after 3 days were late presenters.
Study participants were examined for weight and height, and their nutritional status was classified using the Wellcome Trust Working Party Classification of Childhood Protein Energy Malnutrition[20] and the World Health Organization (WHO)/National Center for Health Statistics (NCHS) classification of childhood under-nutrition. Patients were also examined for pallor, cyanosis, nasal flaring, and head nodding, as well as for the presence of pedal oedema. The axillary temperature of each participant was also taken at presentation using a digital thermometer.
All participants had their peripheral oxygen saturation (Osat) levels recorded at presentation using a pulse oximeter (NellcorTM -200, USA) with an appropriately sized paediatric probe attached to the finger or toenail bed. The oximeter reading was recorded after stabilisation for 1 min. Hypoxaemia was defined as an Osat <90%. A chest radiograph was also performed at admission which was read in digital format following the WHO guidelines for the interpretation of chest radiographs for epidemiological studies.[21] Enlarged heart (cardiomegaly) was defined as a cardiothoracic ratio >0.55 in a well-taken chest radiograph[22] Blood culture and malaria rapid diagnostic tests were done for all study participants using automated Bactec machine and optimal kits, respectively, while cerebrospinal fluid (CSF) analysis was done for those who presented with additional features to suggest central nervous system infections.
All children received intravenous antibiotics in line with the hospital's standard protocol. Fluid and calorie balance was ensured, oxygen therapy was administered when indicated, and children with associated congestive heart failure, pleural effusion and other complications were appropriately treated. The children were monitored closely until the end of hospitalisation and the outcome of each participant was documented. Admitted patients were discharged home 24 hours after the resolution of all symptoms and signs. Children who stayed for longer than 5 full days in the hospital were classified as having undergone prolonged hospitalisation.
Ethics
Ethical clearance for the study was obtained from the Joint Gambian Government/Medical Research Council ethical committee. Informed consent was obtained from the caregiver of all study participants.
Data analysis
Data were analysed using SPSS (version 17.0). Means and standard deviations (SDs) were determined for normally distributed continuous variables and medians and interquartile ranges (IQRs) for non-normally distributed variables. Proportions and percentages were determined for categorical variables. Differences between continuous variables were determined using Student's t-test for normally distributed variables and the Mann-Whitney U-test for non-normally distributed variables, while the differences between categorical variables were determined using Pearson's X2 and Fisher's exact tests as appropriate (with Yate's correction where applicable). The level of significance at a 95% confidence interval (CI) was set at p<0.05.
Associations between dependent (prolonged hospital stay) and independent variables (risk factors) were initially assessed by uni-variate analysis. Those that gave significant results were used in the multivariate analysis to determine their independent effects on dependent variables. Results were interpreted with odds ratios (ORs) and 95% CIs. Statistical significance was established when the CI did not embrace unity.
Results
During the 6-month study period, 1 517 under-5s were admitted to the paediatric ward of the Basse Major Health Centre; 420 (27.6%) fulfilled the criteria for severe pneumonia, as previously defined by the WHO, and formed the basis of further data analysis.
Sociodemographic characteristics
The majority of the participants were infants (168; 40%) with a slight male preponderance (1.2:1 male to female ratio) and an age range of 2 - 59 months (median 14.0; interquartile range (IQR) 17.0 - 19.0). In terms of residence overcrowding, 36 (8.6%) of the 420 children lived in overcrowded rooms, while the remainder (384; 91.6%) lived in non-crowded rooms. In terms of immunisation status, 344 (81.9%) of the patients were appropriately immunised for age according to the Gambian National Programme on Immunization (Table 1).
Clinical presentation and investigations
Two-hundred and forty-five (58.3%) of the children presented to the health centre within 3 days of noticing symptoms (early presenters), while 175 (41.7%) presented more than 3 days after the onset of symptoms (late presenters).
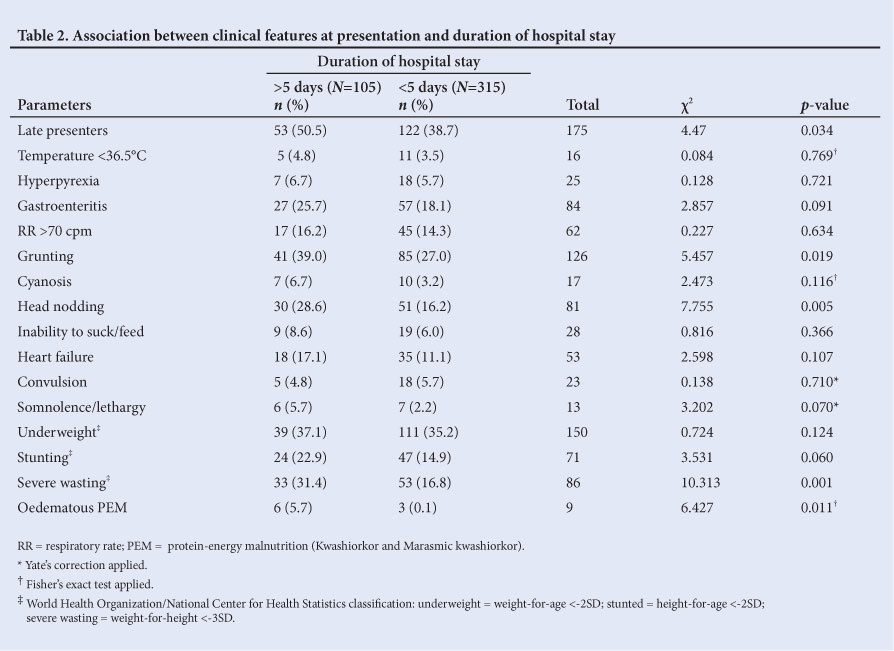
In addition to severe pneumonia, gastroenteritis and convulsion were observed in 84 (20%) and 23 (5.5%) patients, respectively; and 53 (12.6%) had features of cardiac decompensation, viz. significant tachycardia, tachypnoea and enlarged, tender liver. Other features at presentation are highlighted in Table 2.
The axillary temperature of the patients ranged from 34.8°C to 40.8°C (mean 38.3; SD ±1.1). Eighty-five (20.2%) participants did not have fever at presentation, while 15 (3.6%) had subnormal temperatures and one even had hypothermia (0.2%). The mean weight of the recruited patients was 8.1 kg (SD ±2.6; range 2.5 - 18.5) and the mean height was 75.7 cm (SD ±12.1; median 74.8; range 49.8 - 110.0). In terms of nutritional status, 145 (41.7%) patients were wasted, 150 (35.7%) were underweight and 71 (16.9%) had features of chronic malnutrition manifesting as stunting. Nutritional oedema was present in 9 (2.2%) patients at presentation (Table 2).
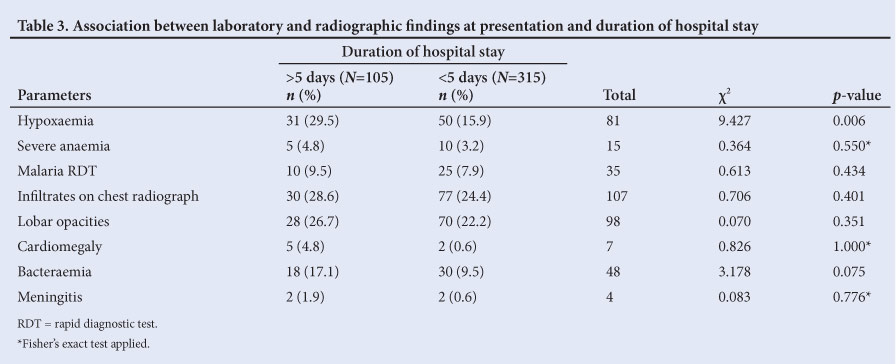
About one-half of the patients (204; 48.6%) had normal chest radiographs at presentation. There were more infiltrates (107; 25.5%) than other abnormal findings in the chest radiographs, followed by classical homogenous opacities (98; 23.3%) (Table 3).
The mean Osat at presentation was 92.6% (SD ±7.0; median 94; range 35 - 100). Approximately one-fifth of the patients (81; 19.3%) were hypoxaemic; the remaining 339 (80.7%) had a normal Osat of >90%.
Of the 105 children who had a prolonged hospital stay, 96 (91.4%) were discharged home well, seven (6.7%) were DAMA and two (1.9%) were referred. No mortality was recorded among the children with a prolonged hospital stay.
Predictors of prolonged hospitalisation
No statistically significant relationship was found between the duration of hospital stay and age, gender, immunisation status or living in an overcrowded home (Table 1). No significant difference was found between the median age of children who had, and those who did not have a prolonged hospital stay (13.0 months (IQR 15.0 - 17.0) v. 14.0 months (IQR 18.0 - 20.0), respectively; Mann-Whitney U-test 15 123.500; p=0.190).
Fifty-three (30.3%) of the 175 late presenters had a prolonged hospital stay compared with 52 (22.2%) of the remaining 245 who presented early. This was statistically significant (p=0.034). Likewise a greater proportion of children who presented with grunting respiration (41/126; 32.5%) had a prolonged hospital stay than children without grunting (64/294; 21.7%) (p=0.019) (Table 2). Also, significantly more children who presented with head nodding had a prolonged hospital stay than those without head nodding (p=0.005). Furthermore, a significantly greater proportion of infants displayed head nodding than children of the other age groups (72.8% v. 27.2%; x2=45.094; p<0.001); in general, children who displayed head nodding were significantly younger than those without head nodding (Mann-Whitney U-test 6 206.000; p<0.001).
Children with lethargy, oedematous protein-energy malnutrition (PEM) as well as those who were underweight and severely wasted at presentation were found to stay longer in the hospital than those without such features (statistically significant; p<0.05) (Table 2).
Hypoxaemia at admission was significantly associated with prolonged hospitalisation in children with severe pneumonia (38.3% v. 21.8%, df=1; p=0.006). The association between other investigative findings and the duration of hospital stay is shown in Table 3.
In summary, children who presented after 3 days of illness (late presenters) (p=0.034), those with grunting respiration (p=0.019), head nodding (p=0.005), the presence of oedematous PEM (Kwashiorkor and Marasmic kwashiorkor) (p=0.011), severe wasting (p=0.001) and hypoxaemia at presentation (p=0.006) were significantly likely to stay longer than 5 days in hospital, according to Pearson's X2 test of association (p<0.05) (Tables 1 - 3). With further analysis using multiple logistic regression, head nodding (OR 1.929; 95% CI 1.124 - 3.414; p=0.018), the presence of oedematous PEM (OR 5.813; 95% CI 1.060 - 3.616; p=0.006), severe wasting (OR = 2.071; 95% CI 1.047 - 3.241; p=0.034) and hypoxaemia at presentation (OR 2.220; 95% CI 1.097 - 3.405; p=0.023) were independent predictors of the need for a prolonged hospital stay in childhood pneumonia (Table 4).
Discussion
Prolonged hospitalisation was observed in 25% of the study patients admitted and managed for severe pneumonia. The independent predictors of prolonged hospital stay were head nodding at presentation, the presence of oedematous PEM (Kwashiorkor and Marasmic kwashiorkor) and hypoxaemia.
Head nodding usually occurs in young infants in severe respiratory distress who employ accessory muscles of respiration including the sternocleidomastoid muscles to facilitate respiratory excursion and enhance gaseous exchange. In situations with severe lung consolidation and impaired gaseous exchange, these accessory muscles or respiration are used to increase tidal volume.[23] Given that these muscles are attached on the neck and chest walls, their increased usage leads to exacerbated movements of the chest wall and the neck. [23] Head nodding implies a higher degree of pneumonia severity in young children, and has also been associated with the presence of hypoxaemia and an increased need for oxygen therapy to aid ventilation.[23,28] Hence, infants and young children with pneumonia who head nod are more likely to stay longer in the hospital than those who do not head nod.
Malnourished children, especially those with severe wasting and oedematous PEM, were found to stay longer in hospital than their counterparts who were well nourished. This finding is in keeping with reports from India by Tiewsoh et al.[8] where a lack of breastfeeding - a major precipitant of under-nutrition - was reported as a significant risk factor for prolonged hospitalisation among a cohort of children with severe pneumonia.
Severe childhood under-nutrition is often associated with depressed cellular, and to a less extent humoral, immunity in malnourished children, rendering them prone to infections, with increasing difficultly to recover.[24] An increased titre of aflatoxins has been reported in the lungs of children who died from oedematous PEM compared with their counterparts who were well nourished.[25] An increased tissue aflatoxins titre denotes depressed antioxidant contents, poor handling of toxins and increased tissue destruction, hence poor recovery from illness is often noticed in undernourished children.[25] Severely under-nourished children also have an impaired capacity to eliminate pathogens due to poor and ineffective mucociliary activities, atrophy of the recticulo-endothelial organs, impaired phagocytic functions of alveolar macrophages and associated micronutrient-deficient states.[26,27] These make recovery from infections including pneumonia difficult and many undernourished children often die easily from such infections.[27] Many workers also reported severe under-nutrition as a major determinant of significant morbidity and increased mortality in childhood pneumonia.[5-8]
Hypoxaemia was also found to be an independent predictive factor of prolonged hospitalisation in childhood pneumonia. A hypoxaemic child has impaired gaseous exchange, usually from ventilation-perfusion mismatch as a result of increased death space created by lung consolidation.[23] The presence of hypoxaemia in an ill child usually signifies severe disease and the need for close monitoring and appropriate supportive therapy including oxygen administration.[28] Severe disease often requires prolonged hospitalisation, as corroborated by the findings in this study. Hence, prompt recognition and management of hypoxaemia is desirable in the management of children with severe pneumonia.[28]
We recognise that our findings may have been limited by the fact that retroviral screening was not routinely done to detect HIV infection, and that such infection may have affected the length of hospitalisation. The prevalence of HIV-seropositivity at the study site was reportedly low, given as <1.0%,[29] thus routine retroviral screening would not have been cost-effective. Also, further investigations were not done to rule out PTB; however, our exclusion of children with cough of a prolonged duration (>2 weeks) and those with audible and/or auscultatory wheeze, together with the good response of study participants to antibiotics, was assumed to have assisted greatly in excluding children with PTB and bronchial asthma.
Conclusion
The counselling of caregivers of children hospitalised for severe pneumonia, especially children with severe under-nutrition, head nodding or hypoxaemia, should encompass the expected prolonged hospital stay. This is even more relevant in resource-poor settings where caregivers are often required to pay 'out of pocket' for treatment. This may enable caregivers to prepare adequately to mobilise enough resources to see the hospitalisation through, thereby reducing the incidence of incomplete treatment, DAMA and its consequences.
Acknowledgments
We acknowledge the clinicians, nurses, X-ray technicians and fieldworkers for their contributions to this work.
References
1. Rudan I, Tomaskovic L, Boschi-Pinto C, Campbell H. Global estimate of the incidence of clinical pneumonia among children under five years of age. Bull World Health Organ 2004;82:895-903. [ Links ]
2. Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of worldwide distribution of child deaths from acute respiratory infections. Lancet Infect Dis 2002;2:25-32. [ Links ]
3. Greenwood BM, Greenwood AM, Bradley AK, et al. Deaths in infancy and early childhood in a well-vaccinated, rural West African population. Ann Trop Paediatr 1987;7:91-99. [ Links ]
4. World Health Organization. Acute Respiratory Infections in Children: Case Management in Small Hospitals in Developing Countries. Report no. 5. Geneva: WHO, 1990. [ Links ]
5. de Francisco A, Morris J, Hall AJ, Armstrong Schellenberg JR, Greenwood BM. Risk factors for mortality from acute lower respiratory tract infections in young Gambian children. Int J Epidemiol 1993;22(6):1174-1182. [ Links ]
6. Johnson WBR, Osinusi K, Aderele WI, et al. Etiologic agents and outcome determinants of community acquired pneumonia in Urban children. A hospital based study. Afr J Med Sci 2008;100(4):370-385. [ Links ]
7. Mtango FD, Neuvians D, Broome CV, Hightower AW, Pio A. Risk factors for deaths in children under 5 years old in Bagamoyo district, Tanzania. Trop Med Parasitol 1992;43:229-233. [ Links ]
8. Tiewsoh K, Lodha R, Pandey RM, et al. Factors determining the outcome of children hospitalized with severe pneumonia. BMC Pediatrics 2009;9:15 [ Links ]
9. Mulholland Ek, Smith L, Carneiro I, Becher H, Lehnman D. Equity and child survival strategies. Bull World Health Organ 2008;86(5):399-407. [ Links ]
10. Hall MJ, De Frances CJ. National hospital discharge survey. http://www.cdc.gov/nchs/data/ad/ (accessed 18 February 2012). [ Links ]
11. Chola L, Robberstad B. Estimating average inpatient and outpatient costs and childhood pneumonia and diarrhoea treatment costs in an urban health centre in Zambia. Cost Eff Resour Alloc 2009;7:16. [http://dx.doi.org/1186/1478-7547-7-16Links ] Arial, Helvetica, sans-serif" size="2">]
12. Ayieko P, Akumu AO, Griffiths UK, English M. The economic burden of inpatient paediatric care in Kenya: Household and provider costs for treatment of pneumonia, malaria and meningitis. Cost Eff Resour Alloc 2009;7:3. [ Links ]
13. Hussain H, Waters H, Khan AJ, Omer SB, Halsey NA. Economic analysis of childhood pneumonia in Northern Pakistan. Health Policy Plan 2008;23(6):438-442. [ Links ]
14. Eke GK, Opara PI. Discharge against medical advice amongst patients admitted into the Paediatric wards of the University of Port Harcourt Teaching Hospital. Niger J Paed 2013;40(1):40-44. [ Links ]
15. Choi M, Kim H, Qian H, Palepu A. Readmission rates of patients discharged against medical advice: A matched cohort study. PLoS ONE 2011;6(9):e24459. [http://dx.doi.org/10.1371/journal.pone.0024459] [ Links ]
16. Ekpe EE, Akpan MU. Poorly treated broncho-pneumonia with progression to empyema thoracis in Nigerian children. TAF Prev Med Bull 2010:9(3):181-186. [ Links ]
17. Moïsi JC, Gatakaa H, Berkley JA, et al. Excess child mortality after discharge from hospital in Kilifi, Kenya: A retrospective cohort analysis. Bull World Health Organ 2011;89:725-732. [ Links ]
18. Basse Demographic Data Base. The Gambia. http://www.accessgambia.com/information/basse-santa-su.html (accessed 10 May 2012). [ Links ]
19. Park K. Environment and Health. In: Park JE, Park K, eds. Park's Textbook of Preventive and Social Medicine. Jabalpur: Banarasidas Bhanot and Company, 2006:521-536. [ Links ]
20. Wellcome Trust Working Party. Classification of infantile malnutrition. Lancet 1970;2:302-303. [ Links ]
21. Cherian T, Mulholland EK, Carlin JB, et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull World Health Organ 2005;83:353-359. [ Links ]
22. Philbin EF, Garg R, Danisa K, et al. The relationship between cardiothoracic ratio and left ventricular ejection fraction in congestive heart failure. Arch Intern Med 1998;158(5):501-506. [ Links ]
23. Bennett NJ, Steele RW. Pediatric Pneumonia. http://emedicine.medscape.com/article/overview (accessed 14 May 2012). [ Links ]
24. Blössner M, de Onis M. Malnutrition: Quantifying the Health Impact at National and Local Levels. Environmental Burden of Disease Series, No. 12. Geneva: World Health Organization, 2005. [ Links ]
25. Oyelami OA, Maxwell SM, Adelusola KA, Aladekomo TA, Oyelese AO. Aflatoxins in the lungs of children with Kwashiorkor and children with miscellaneous diseases in Nigeria. J Toxicol Environ Health 1997;51:623-628. [ Links ]
26. Rivera J, Martorell R. Nutrition, infection and growth. Part II: Effects of malnutrition on infection and general conclusions. Clin Nutr 1988;7:163-167. [ Links ]
27. Tupasi TE, Mangubat NV, Sunico ES, et al. Malnutrition and acute respiratory tract infections in Filipino children. Rev Infect Dis 1990;12:S1047-S1054. [ Links ]
28. Kuti BP, Adegoke SA, Ebruke BE, Howie S, Oyelami OA, Ota M. Determinants of Oxygen Therapy in Childhood Pneumonia in a Resource-Constrained Region. ISRN Pediatrics 2013:435976. [http://dx.doi. org/10.1155/2013/435976] [ Links ]
29. United Nations Children's Fund. 2009 State of the World's Children. New York: UNICEF, 2009. http://www.unicef.org (accessed 16 November 2010). [ Links ]
 Correspondence:
Correspondence:
B P Kuti
(kutitherapy@yahoo.com)


{kind=link}
{kind=link}
{kind=link}
{kind=link}