










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.8 n.1 Pretoria Feb. 2014
RESEARCH
A study investigating sound sources and noise levels in neonatal intensive care units
J NeilleI; K GeorgeII; K Khoza-ShangaseI
IPhD; Department of Speech Pathology and Audiology, School of Human and Community Development, University of the Witwatersrand, Johannesburg, South Africa
IIBA (Speech and Hearing Therapy); Department of Speech Pathology and Audiology, School of Human and Community Development, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Exposure to noise in the neonatal intensive care unit (NICU) has the potential to affect neonatal auditory development, sleep patterns and physiological stability, thus impacting on developmental progress.
OBJECTIVES: This study aimed to identify noise sources in three NICUs in Johannesburg, South Africa, and to determine the sound levels to which neonates in incubators are exposed at various positions in the NICU. These findings were then compared with the standards recommended by the American Academy of Pediatrics (AAP).
METHODS: A prospective, repeated designs measure was adopted. Sound levels were recorded in five different areas of the NICUs at four different times of the day over the course of 3 days. Data were analysed using descriptive statistics.
RESULTS: Sound levels recorded in all the NICUs were considerably higher than those recommended by the AAP, placing vulnerable neonates at risk for developmental disorders. Significantly, most of the noise was human-generated, highlighting the need to develop awareness of the negative effects of noise in the NICU and to implement programmes to reduce noise.
CONCLUSION: The findings have important implications for neonatal care, and highlight the importance of noise reduction and monitoring strategies in the NICU.
Advances in neonatal care have resulted in the improved survival of premature infants locally and internationally.[1] Recent studies[2,3] suggest that 11.1% of all live births are premature, with premature births in Asia and sub-Saharan Africa accounting for 60% of the total. As a consequence of increased survival of premature infants, morbidity relating to disabilities and developmental delays has also increased.[4] Furthermore, although neonatal intensive care units (NICUs) provide the multidisciplinary support that vulnerable infants need, the high levels of stimulation in these environments place many neonates at risk of developing a range of long-term complications including cerebral palsy, cognitive impairment, hearing loss, visual impairment, language disorders, learning difficulties and behavioural disorders.[1,3,5,6] There is therefore a need to identify and evaluate environmental stressors in the NICU, and to develop protocols to minimise exposure to them.
One of the stressors that has been documented to have a negative effect on the premature infant is exposure to noise.[7] Noise exposure has the potential to influence the process of neural organisation, reinforcing inappropriate neural pathways and placing the neonate at risk of auditory processing disorders and future learning disabilities.[7] Because development of the sensory system occurs in a sequential order, with hearing and vision developing last,[7] these senses may be underdeveloped in premature neonates, yet are frequently reported to receive the most input in the NICU environment.[7] This is significant given the increasing chances of survival of infants born before 28 weeks' gestation,[3] since the human fetus is reported to respond to auditory stimulation from approximately 25 weeks, with auditory maturation occurring by 30 - 32 weeks.[7]
International and local research indicates that noise levels in the NICU range between 56 and 120 decibels (dB),[7,8] which has the potential to result in an overwhelming sensory overload and coupled with other sensory input may negatively affect the development of the central nervous system, specifically the auditory system.[7] The American Academy of Pediatrics (AAP) therefore recommends that the combination of mechanical and extraneous noise in incubators should be limited to no more than 45 dB.[5] High levels of noise in the NICU may cause sleep disturbances, physiological instabilities such as fluctuations in heart rate, oxygen saturation levels and blood pressure, and increases in intracranial pressure, as well as hearing impairment (especially when high-frequency noise is coupled with the use of ototoxic medications such as aminoglycosides).[9] Exposure to noise has the potential to affect hearing thresholds, frequency discrimination, sound pattern recognition and localisation of auditory input, and may lead to difficulties in discriminating between speech sounds in the presence of noise, all of which may affect the development of speech and language and consequently affect learning potential.[10] In view of these well-documented effects of exposure to noise in the NICU, efforts to identify sources of noise and to reduce exposure of vulnerable infants to such risks need to be intensified.
Objectives
To identify sources of noise >45 dB in three NICUs in Johannesburg, South Africa, and to determine the sound levels to which neonates in incubators are exposed at various positions in the NICU. These findings were then compared with the standards recommended by the AAP.[5]
Method
Ethical clearance was obtained from the Human Research Ethics Committee (Medical), University of the Witwatersrand (clearance certificate number M110340). NICUs in two private hospitals (A and B) and one tertiary-level state hospital (C) were studied. Sound-level readings were taken with a calibrated Quest Technologies 210 Sound Level Meter and measured in dB.
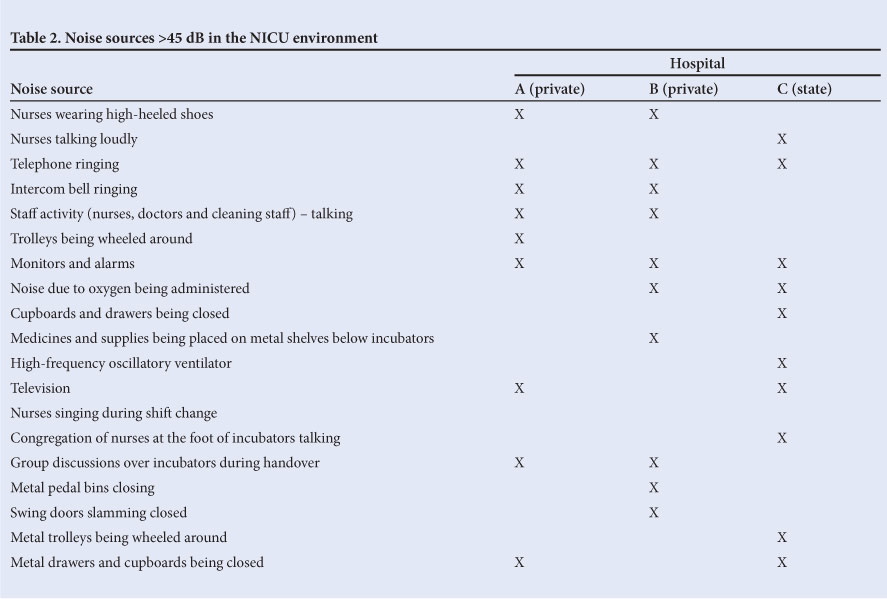
At each site, the layout of the NICU was recorded by a sketch documenting the location of the nurses' station and the position of the incubators (Figs 1 - 3). The nurse-to-patient ratio, occupancy of incubators and loudest source of noise were also documented (Table 1). Additional sources of noise >45 dB were identified and documented (Table 2).

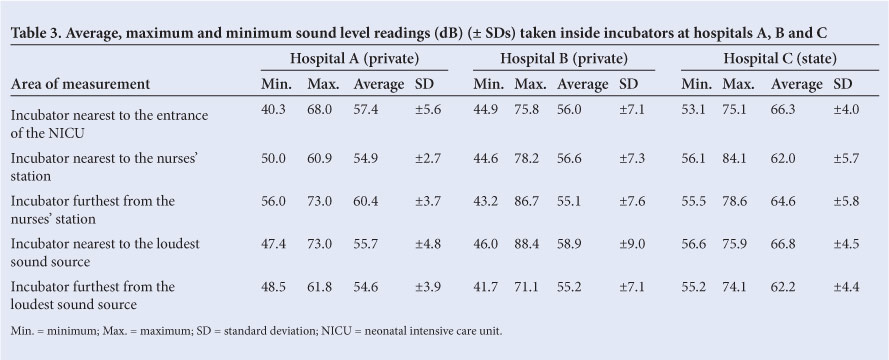
A prospective, repeated measures design was adopted and carried out over a period of 3 consecutive days at each site. Sound-level readings were measured in incubators at five different areas in each NICU at four times of the day (during shift changes, at feeding times, during visiting hours, and during 'quiet time' in hospitals that adopted this approach as a means to reduce noise levels), as depicted in Table 3. Measurements were taken with the neonate inside the incubator, with the sound-level meter situated next to the neonate's head. A total of five readings were taken in each incubator at each of the specified times on each day, averaged to determine the loudest and softest readings, and then averaged across the 3 days of data collection (Table 3). Averaged readings were compared with other readings obtained at other areas in the NICU, as well as across the three study sites.
Data were analysed using descriptive statistics by the authors and verified by a statistician. Ranges, means and standard deviations (SDs) were computed for each area of data collection at each site in order to obtain simple summaries of the sample and the measurements taken. This exploratory data analysis method was deemed appropriate, since it allowed for comparison with the recommended AAP levels.[5]
Results
Floor plans, numbers of incubators and nurse-to-patient ratios were found to vary between the units. All the sound sources >45 dB, with the exception of a high-frequency oscillatory ventilator (hospital C), were identified as human-generated noise. The loudest sound sources were an air vent (hospital A), a nurses' tea room (hospital B), and sounds generated at the entrance to the NICU (hospital C) (Table 1).
These sounds ranged from 14.8 dB to 22.6 dB above the standards recommended by the AAP.[5] However, when these sounds were combined with other mechanical sounds, as well as sounds generated by the baby in the incubator, sound levels in incubators rose to as much as 88.4 dB (Table 3) - 43.4 dB above the standards recommended by the AAP.[5]
Furthermore, a considerable variation existed between the minimum and maximum sound levels obtained inside the incubators in each hospital (Table 3), all of which were greater than those recommended by the AAP.[4] Hospital B had both the lowest minimum sound levels and the loudest maximum sound levels, resulting in the greatest SDs.
Discussion
Noise levels in studies of NICU environments are significantly higher than those recommended by the AAP,[5] placing vulnerable neonates at risk of a variety of developmental complications.[1,3,6] While little has been published on sources of noise and documented noise levels in the NICU environment, our results appear to be consistent with previous local and international findings.[7,8] Although we found variations in occupancy rates, nurse to-patient ratios and individual treatment regimens, no clear patterns emerged regarding differences between the NICUs in this study.
Consistent with other studies investigating noise levels in the NICU,[8] the majority of noise sources identified were human-generated and can therefore be targeted in an attempt to minimise exposure of vulnerable neonates to stressful situations. Strategies to decrease human-generated noise levels are relatively simple and need not involve major costs. They include decreasing the levels of staff conversations, using rubber-soled shoes, turning down volumes of telephones and alarms, creating rubber barriers on filing cabinets and drawers, and muting the volume on the television. Audiologists therefore need to establish and implement noise assessment and monitoring programmes, and to engage in awareness and prevention campaigns with NICU staff. Such protocols are consistent with occupational hearing programmes in the NICU setting, and should be extended to include regular assessment and control of noise levels, regular hearing screening and personal exposure monitoring for each neonate, and implementation of engineering and administrative controls. Furthermore, personal protective equipment such as hearing protection devices may be deemed necessary, depending on the infant's length of stay in the NICU.
Although the findings of this study cannot be generalised to all NICUs in the South African context, they are consistent with another local study conducted in a state hospital.[8] They also provide insight into the positioning of incubators and sound sources, and may therefore help guide best practice in terms of limiting neonates to noise exposure.
Conclusion
Although our findings reflect unacceptably high noise levels in all three NICUs, the results should be interpreted with caution, taking into consideration the limitations imposed by the design of the study. Firstly, the NICU environments did not remain constant over the 3-day period, as new babies were admitted, while others were discharged or transferred to high care. Secondly, the incubators in which sound levels were recorded were observed to have different care environments, including neonates being placed on an oscillatory ventilator, and others receiving supplementary oxygen through nasal prongs. These variations should be taken into consideration in any noise-monitoring protocol. Lastly, readings taken over a short period may result in findings not being as representative as they could be, and averages should therefore ideally be taken over the period of a full day.
Further research implications include replication of the current study with larger sample sizes and careful consideration of the limitations identified, as well as monitoring of the physiological effects of noise in the NICU.
References
1. Ballot DE, Potterton J, Chirwa T, Hilburn N, Cooper PE. Developmental outcome of very low birth weight infants in a developing country. BMC Pediatr 2012;12:11. [http://dx.doi.org/10.1186/1471-2431-12-11] [ Links ]
2. Blencowe H, Cousens S, Oestergaard M, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications.
Lancet 2012;379(9832):2162-2172. [http://dx.doi.org/10.1016/S0140-6736(12)60820-4]
3. Smith PB, Ambalavanan N, Li L, et al. Approach to infants born at 22-24 weeks gestation: Relationship to outcomes of more-mature infants. Paediatrics 2012;129(6):e1508-e1516. [http://dx.doi.org/10.1542/peds.2011-2216] [ Links ]
4. Altuncu E, Akman I, Kulekci S, et al. Noise levels in neonatal intensive care unit and use of sound absorbing panel in isolette. Int J Pediatr Otorhinolaryngol 2009;73(7):951-953. [http://dx.doi.org/10.1016/j.ijporl.2009.03.013] [ Links ]
5. Lasky RE, Williams AL. Noise and Light Exposures for Extrememly Low Birthweight Newborns During Their Stay in the Neonatal Intensive Care Unit. 2007. http://pediatrics.aappublications.org/content/123/2/540.full.pdf (accessed 13 July 2011). [ Links ]
6. Vandenberg K. Individualized developmental care for high risk newborns in the NICU: A practice guideline. Jounal of Early Human Development 2007;83(7):433-442. [http://dx.doi.org/10.1016/j.earlhumdev.2007.03.008] [ Links ]
7. White-Taut R, Nelson M, Silvestri J, et al. Maturation of the cardiac response to sound in high-risk preterm infants. Newborn & Infant Nursing Reviews 2009;9(4):193-199. [http://dx.doi.org/10.1053/j.nainr.2009.09.011] [ Links ]
8. Nathan LM, Tuomi SK, Müller AM, Kirsten GF. Noise levels in a neonatal intensive care unit in the Cape Metropole. South African Journal of Child Health 2008;2(2):50-54. [ Links ]
9. Chen H, Chen C, Wu C, Huang H, Wang T, Hsu C. The influence of neonatal intensive care unit design on sound level. Pediatr Neonatol 2009;50(6):270-274. [http://dx.doi.org/10.1016/S1875-9572(09)60076-0] [ Links ]
10. Kellam B, Bhatia J. Sound spectral analysis in the intensive care nursery: Measuring high frequency sound. J Pediatr Nurs 2008;23(4):317-323. [http:// dx.doi.org/10.1016/j.pedn.2007.09.009] [ Links ]
 Correspondence:
Correspondence:
J Neille
(joanne.neille@wits.ac.za)


{kind=link}
{kind=link}