










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.7 n.3 Pretoria Jan. 2013
CASE REPORT
An unusual case of Milroy disease
N R Schamroth
MB BCh. Knysna Provincial Hospital, Knysna, Western Cape, South Africa
ABSTRACT
The interesting case of an infant who presented with congenital lymphoedema with features of Milroy disease is presented. The infant's clinical findings were marked and somewhat atypical. Lymphoscintigraphy demonstrated features consistent with the diagnosis.
A 6-month-old female infant was brought to Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa, in August 2012 by her parents, who came from a rural village in Lesotho. According to her mother, the baby had been born with a 'swollen body. Her face, upper limbs and right leg were most affected. Although the swelling had decreased over time, it persisted in the upper limbs and right leg. The infant was growing well and had not had any episodes of acute illness, and her milestones were appropriate for her age. Her mother was a primigravida and had had 2 previous miscarriages at 1 month and 3 months, respectively. She reported no prenatal problems and had given birth vaginally at a rural clinic. The baby was born at term with a weight recorded as 3 060 g, and her mother reported no postnatal complications.
Neither of the parents had any illnesses, and there was no history of other family members with a similar condition to that of the child. There was no history of travel to areas endemic for conditions causing lymphoedema.
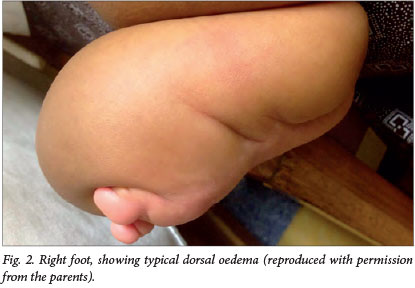
The baby was active, mobile and curious. Her anthropometry was appropriate for her age and she appeared well with no dysmorphic features. She had mild peri-orbital oedema and striking, non-pitting brawny oedema of the upper limbs and right leg (Fig. 1). The oedema was marked at the palm and dorsum of the hands and foot with sparing of the distal digits (Fig. 2). The oedema of the arms tapered above the level of the biceps. The oedema of the limbs was non-tender but firm. There was no evidence of lymphadenopathy, ascites or cardiac failure. She had no other dermatological stigmata and had full movement of all her limbs with good power.

The primary diagnosis was congenital lymphoedema, consistent with features of Milroy disease. This diagnosis was confirmed on lymphoscintigraphy, which showed a patent peripheral left lower limb lymphatic system and a lack of tracer migration in the right lower limb and both upper limbs (Fig. 3).

Discussion
Other differential diagnoses include lymphoedema-distichiasis syndrome, Meige disease, hypotrichosis-lymphedema-telangiectasia syndrome, Turner syndrome, Noonan syndrome, and lymphoedema with yellow nails/yellow nail syndrome.[1]
Milroy disease is a congenital form of primary lymphoedema. It is an autosomal dominant condition inherited with variable expression and reduced penetrance. It is commonly (75% of cases) associated with the vascular endothelial growth factor receptor 3 mutation, which causes abnormal phosphorylation of a tyrosine kinase reception specific for lymphatic vessels.[2,3] This causes lymphatic dysfunction leading to lymphoedema.[4]
Milroy disease is more common in females than in males. Patients present with firm oedema and the right leg is classically the main limb involved, usually below the level of the knee. The main morbidity is associated with recurrent bouts of cellulitis and lymphangitis. Management is mainly supportive, and no surgical method has achieved lasting success.
This case is unusual, as the infant presented with involvement of three limbs: the right leg above the level of the knee and both arms to the level of the biceps. There was no family history of this condition, and it can therefore be assumed that it is either a sporadic mutation phenomenon or a case of reduced penetrance in a parent.
References
1. Brice G, Mansour S, Ostergaard P, Connell F, Jeffrey S, Mortimer P. Milroy disease. Hereditary lymphedema, type I: Milroy congenital lymphedema. In: Pagon RA, Bird TD, Dolan CR, et al, eds. Gene Reviews. Seattle: University of Washington, 1993. http://www.ncbi.nlm.nih.gov/books/NBK1239/ (accessed 7 August 2013). [ Links ]
2. Connell FC, Ostergaard P, Carver C, et al. Lymphoedema consortium: Analysis of the coding regions of VEGFR3 and VEGFC in Milroy disease and other primary lymphoedemas. Hum Genet 2009;124(6):625-631. [http://dx.doi.org/10.1007%2Fs00439-008-0586-5] [ Links ]
3. Irrthum A, Karkkainen MJ, Devriendt K, Alitalo K, Vikkula M. Congenital hereditary lymphedema caused by a mutation that inactivates VEGFR3 tyrosine kinase. Am J Hum Genet 2000;67(2):295-301. [http://dx.doi.org/10.1086%2F303019] [ Links ]
4. Mellor RH, Hubert CE, Stanton AW, et al. Lymphatic dysfunction, not aplasia, underlies Milroy disease. Microcirculation 2010;17(4):281-296. [http://dx.doi.org/10.1111%2Fj.1549-8719.2010.00030.x] [ Links ]
 Corresponding author: N R Schamroth (drnscham@gmail.com)
Corresponding author: N R Schamroth (drnscham@gmail.com)

