










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.7 n.1 Pretoria Jan. 2013
CASE REPORT
An unusual case of neonatal meningococcal meningitis complicated by subdural empyema and hydrocephalus
Y RamsamyI; P MahabeerII; M ArcharyIII; R A BobatIV; Y M CoovadiaV
IMB ChB; National Health Laboratory Services and Department of Medical Microbiology, University of KwaZulu-Natal, Durban
IIMB ChB, FCPath (Microbiol); National Health Laboratory Services and Department of Medical Microbiology, University of KwaZulu-Natal, Durban
IIIMB ChB, FCPath (Microbiol); National Health Laboratory Services and Department of Medical Microbiology, University of KwaZulu-Natal, Durban
IVMB ChB, DCH (SA), FCPaed (SA), Cert ID (Paed) (SA); Department of Paediatrics, University of KwaZulu-Natal, Durban
VMB ChB, FCPaed (SA), Cert ID (Paed) (SA); Department of Paediatrics, University of KwaZulu-Natal, Durban
ABSTRACT
Neisseria meningitidis is a leading cause of pyogenic meningitis worldwide, as well as causing large epidemics in parts of Africa. With the dramatic decline in cases of Haemophilus influenzae B, N. meningitidis has emerged as one of the most common causes of acute bacterial meningitis in children and adults in South Africa. However, it remains an uncommon cause of meningitis in the neonatal period. Subdural empyema together with hydrocephalus has been infrequently described as a complication of meningococcal meningitis.
We report a rare case of neonatal meningococcal meningitis, complicated by subdural empyema and hydrocephalus. To the best of our knowledge only a few cases of neonatal meningococcal meningitis have been reported from South Africa, with none of these cases having the complication of subdural empyema.
Neisseria meningitidis remains an important cause of meningitis in children and adolescents worldwide.[1] Neonatal meningococcal meningitis is uncommon, with a prevalence of only 2/10 000 being reported by the Centers for Disease Control.[2] Subdural empyema development in the course of meningococcal disease in adults is rare, but seems to affect children more frequently.[3]N. meningitidis remains a major health problem despite effective antibiotics and vaccination.[4] A 10-year study at the Chang Gung Children's Hospital, Taipei, reported on the clinical spectrum of meningococcal infection in infants younger than 6 months of age; 7 of the 10 were neonates, and 4 of these had subdural empyema as a complication.[4] There has been 1 documented case of intra-uterine infection caused by N. meningitidis[5]
Case report
A 3-week-old male infant was admitted with a 2-day history of fever, lethargy and poor feeding. His mother was known to be HIV-infected; her CD4 count was 264 cells/µl, and she had been started on zidovudine during the pregnancy. The baby was born by normal vaginal delivery at term, weighing 3 610 g. The immediate postnatal period was uneventful and he was commenced on nevirapine prophylaxis at birth. The family lived in a small, overcrowded informal dwelling with three other families, including an 8-year-old school-going sibling.
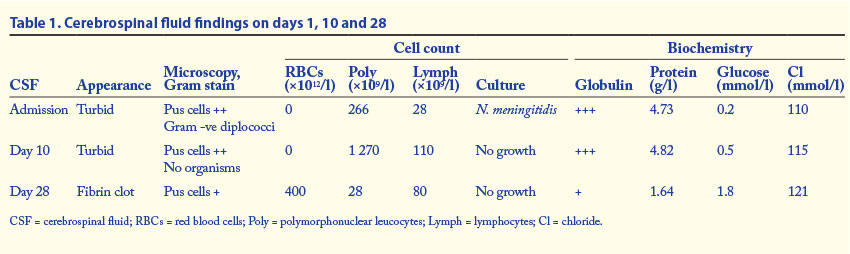
On examination the infant was poorly responsive with decreased tone, pallor and a temperature of 39°C. No skin rashes or petechiae were noted. Central nervous system examination revealed a full fontanelle but no focal neurological signs. Lumbar puncture was performed (Table 1), and other tests on admission included a full blood count, measurement of urea and electrolytes, liver function tests and measurement of C-reactive protein.
The polyvalent bacterial antigen test was positive for N. meningitidis, which was also confirmed on culture and identified as serotype W135 at the National Institute for Communicable Diseases.
The full blood count revealed a white cell count of 3.77x109/l (normal 5.5 - 18x109/l), a haemoglobin concentration of 7.8 g/dl (normal 11.5 - 16 g/dl) and a platelet count of 163x109/l (normal 150 - 400x109/l). The C-reactive protein level (295 mg/l) was markedly increased. Urea and electrolyte levels and the results of liver function tests were normal.
The infant was started empirically on intravenous ceftriaxone 500 mg daily, but developed generalised tonic seizures, with no loss of consciousness, 2 days after admission. The seizures were managed with lorazepam and phenobarbitone. A computed tomography (CT) scan of the brain showed dilatation of the ventricles in keeping with hydrocephalus as well as trans-ependymal fluid and rim-enhancing collections in both cerebral hemispheres compatible with empyema. A diagnosis of complicated meningitis with subdural empyema and hydrocephalus was made. On the basis of the cerebrospinal luid analysis after 10 days of ceftriaxone (Table 1), neurosurgical advice was to continue intravenous ceftriaxone for 28 days and review thereafter.
The patient continued to have seizures, increased tone, scissoring and opisthotonus, and the occipitofrontal circumference increased from 41 cm to 44 cm. A repeat CT scan revealed an active communicating hydrocephalus. A ventriculoperitoneal (VP) shunt was inserted, and a CSF specimen was obtained during the procedure (Table 1). The subsequent hospital stay and follow-up to 21 months was uneventful. The patient has delayed motor milestones with inability to walk. The VP shunt is still in place and functional, and the latest CT scan reveals ventriculomegaly but no hydrocephalus. His HIV test has remained negative at 18 months.
Discussion
Acute bacterial meningitis is particularly common during the neonatal period and is associated with high mortality and morbidity including long-term neurological sequelae.[5] Neonates are at increased risk of sepsis because of a relative deiciency in humoral and cellular immunity, as well as in phagocytic function. Infants born at less than 32 weeks' gestation receive little of the maternal immunoglobulin received by full-term infants.[6] Inefficiency in neonates' alternative complement pathway compromises their defence against encapsulated bacteria.[7] HIV-exposed uninfected infants are at higher risk of bacterial sepsis than HIV-unexposed infants as a result of deiciencies in innate immunity, incomplete maternal antibody protection, and increased environmental exposure to pathogens.[8-12]N. meningitidis, Haemophilus infuenzae B and Streptococcus pneumoniae are responsible for the majority of cases of meningitis in children, but are uncommon causes of neonatal meningitis owing to protection from maternally transferred antibodies to the neonate.[11]
N. meningitidis exists as normal flora of the upper respiratory tract and is transmitted by direct contact or via droplets.[13] Studies in the USA and the UK indicate that between 5% and 10% of the population carry N. meningitidis in the nasopharynx at any given time.[14] The risk of acquiring infection with N. meningitidis is directly related to the nature and duration of contact.'151 Household overcrowding, coexisting viral infection and exposure to tobacco smoke increase the risk '151 Our patient lived in a small, overcrowded dwelling, with three other families, and a positive contact could therefore not be excluded. The mother was not screened as a carrier.
Transient meningococcaemia is characterised by a short, febrile lu-like episode with a nonspecific rash.[16] When the bacteraemia is not cleared, clinically overt disease develops.
Meningitis is the most common clinical presentation of invasive meningococcal disease, but haemorrhagic skin lesions are present in 28 - 77% of patients and some present with severe persistent shock lasting for more than 24 hours or until death.[17]
Sub-Saharan Africa has a distinctive epidemiological pattern in which N. meningitidis occurs in yearly waves, and serogroup A has commonly been associated with these epidemics.[61] Other important clinical serogroups include B, C, X, Y, W-135 and Z. In South Africa, W135 was documented as the most predominant serogroup in 2011.[15] However children aged under 1 year were at greatest risk of disease caused by serogroups B, W135 and Y.[15]
Neurological complications of bacterial meningitis in children include subdural efusion or empyema, cerebral abscess, hydrocephalus, focal deicits and seizures, which are often seen during the acute stage of the disease.[5] Sequelae occur in approximately 10% of patients with meningococcal meningitis, and permanent neurological deicits include hearing loss.[4] Subdural empyema occurs relatively more frequently in children than adults.[3] Mortality is reportedly less than 10% if patients are alert at the time of admission, but increases dramatically to 75% if the patient is already comatose.[3]
H. infuenzae B used to be the commonest cause of subdural effusion, but has now been replaced by N. meningitidis because of the universal use of HIB conjugate vaccine.
No deinitive guidelines exist regarding the duration of treatment for subdural empyema, but most series report 2 - 6 weeks of intravenous antibiotics.[18] The type of surgical procedure has little impact on outcome, provided it is performed early and allows for complete evacuation of the pus.[18] The optimal duration of antimicrobial therapy for subdural empyema is uncertain. Parenteral antimicrobial therapy is recommended for at least 3 weeks after neurosurgery, followed by 3 weeks of oral therapy.[4]
Conclusion
With the dramatic decline in cases of H. influenzae B as a direct result of widespread vaccination with the HIB conjugate vaccine, N. meningitidis has emerged as one of the most common causes of acute bacterial meningitis in children. However, it remains an unusual cause of acute bacterial meningitis in the neonatal period, probably because of the protective efect of maternal antibodies. Neonatal meningitis is associated with high morbidity and mortality. Subdural empyema together with hydrocephalus as a complication of meningococcal meningitis has been infrequently described in the literature. Despite the use of ceftriaxone in appropriate doses, to which the organism was fully susceptible, our patient deteriorated and developed complications of subdural empyema and hydrocephalus. Establishing the aetiological diagnosis, as demonstrated in our patient, was vital for correct management of the meningitis and the associated rare complication of subdural empyema and hydrocephalus.
References
1. Falcao MC, de Andrade SB, Ceccon MEJR. Neonatal sepsis and meningitis caused by Neisseria meningitidis: A case report. Rev Inst Med Trop Sao Paulo 2007;49(3):191-194. [http://dx.doi.org/10.1590%2FS0036-46652007000300010] [ Links ]
2. Pinner RW, Gellin BG, Bibb WF, et al. Meningococcal disease in the United States, 1986. Meningococcal Disease Study Group. J Infect Dis 1991;164(2):368-374. [http://dx.doi.org/10.1093%2Finfdis%2F164.2.368] [ Links ]
3. Kawai Y, Gosling RD, Jones V, Hosein IK. An unusual case of meningococcal meningitis complicated with subdural empyema in a 3 month old infant: a case report. BioMed Central - Cases Journal 2009;2:6335. [http://dx.doi.org/10.4076/1757-1626-2-6335]. [ Links ]
4. Huang HR, Chen HL, Chu SM. Clinical spectrum of meningococcal infection in infants younger than six months of age. Chang Gung Med J 2006;29(1):107-112. [ Links ]
5. Kurlenda J, Agata KP, Grinholc M. Neonatal intrauterine infection with Neisseria meningitidis B. Clin Pediatr 2010;49(4):388-390. [http://dx.doi.org/10.1177/0009922809352376] [ Links ]
6. Volpe JJ. Bacterial and fungal intracranial infections. In: Kao A, ed. Neurology of the Newborn. 5th ed. Philadelphia, Pa: Saunders Elsevier; 2008:916-956. [ Links ]
7. Krebs VLJ, Costa GAM. Clinical outcome of neonatal bacterial meningitis according to birth weight. Arq Neuropsiquiatr 2007;65(4B):1149-1153. [http://dx.doi.org/10.1590%2FS0004-282X2007000700011] [ Links ]
8. Slogrove AL, Cotton MF, Esser MM. Severe infections in HIV-exposed uninfected infants: Clinical evidence of immunodeficiency. J Trop Pediatr 2010;56:75-81. [http://dx.doi.org/10.1093%2Ftropej%2Ffmp057] [ Links ]
9. Hygino J, Lima PG, Filho RG, et al. Altered immunological reactivity in HIV-1-exposed uninfected neonates. Clin Immunol 2008;127(3):340-347. [http://dx.doi.org/10.1016%2Fj.clim.2008.01.020] [ Links ]
10. Adhikari M, Kauchali S, Moodley A. Clinical profile and morbidity pattern of infants born to HIV infected mothers in Durban South Africa. Indian Pediatr 2006;43(9):804-808. [ Links ]
11. Lin HC, Wang SM, Wu CS, et al. Clinical and immunologic characteristics and therapeutic interventions in children born to human immunodeiciency virus-infected mothers in Southern Taiwan. J Microbiol Immunol Infect 2005;38(2):89-95. [ Links ]
12. de Moraes-Pinto MI, Almeida AC, Kenj G, et al. Placental transfer and maternally acquired neonatal IgG immunity in human immunodeficiency virus infection. J Infect Dis 1996;173:1077-1084. [http://dx.doi.org/10.2217%2FfVl.11.124] [ Links ]
13. Kuhn L, Meddows-Taylor S, Gray G, Tiemessen C. Human immunodeficiency virus (HIV)-specific cellular immune responses in newborns exposed to HIV in utero. Clin Infect Dis 2002;34(2):267-276. [http://dx.doi.org/10.1086%02F338153] [ Links ]
14. Manchanda V,Gupta S, Bhalla P. Meningococcal disease: History, epidemiology, pathogenesis, clinical manifestations, diagnosis, antimicrobial susceptibility and prevention. Indian J Med Microbiol 2006;24(1):7-19. [http://dx.doi.org/10.4103/0255-0857.19888] [ Links ]
15. Department of Health, Republic of South Africa. Guidelines for the Prevention, Management and Control of Meningococcal Disease in South Africa. Pretoria: Department of Health, 2011. http://www.doh.gov.za/docs/policy/2012/meningococcaldisease.pdf (accessed 6 January 2013). [ Links ]
16. van Deuren M, Brandtzaeg P, Jos W, et al. Update on meningococcal disease with emphasis on pathogenesis and clinical management. Clin Microbiol Rev 2000;13(1):144-166. [http://dx.doi.org/10.1128%2FCMR.13.1.144-166.2000] [ Links ]
17. Stephens DS, Greenwood B, Brandtzaeg P. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet 2007;369(9580):2196-2210. [http://dx.doi.org/10.1016%2FS0140-6736%2807%2961016-2] [ Links ]
18. Tummala RP, Chu RM, Hall WA. Subdural empyema in children Neurosurgery Quarterly 2004;14(4):257-265. [http://dx.doi.org/10.1097%2F00013414-200412000-00011] [ Links ]
 Correspondence: YRamsamy (yogandree@gmail.com)
Correspondence: YRamsamy (yogandree@gmail.com)


{kind=link}