










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Crime Quarterly
versión On-line ISSN 2413-3108
versión impresa ISSN 1991-3877
SA crime q. no.59 Pretoria mar. 2017
http://dx.doi.org/10.17159/2413-3108/2017/v0n59a1547
REVIEW ESSAY
Violence and injury observatories: Reducing the burden of injury in high-risk communities
Ardil JabarI; Richard MatzopoulosII
IPublic Health Specialist with a further specialisation in Disaster Medicine. He is currently completing his PhD research at the University of Cape Town's School of Public Health and Family Medicine. a.jabaroo@gmail.com
IISpecialist Scientist at the Medical Research Council's Burden of Disease Research Unit and an Honorary Research Associate at the University of Cape Town's School of Public Health and Family Medicine and its Centre for Occupational and Environmental Health. Richard.Matzopoulos@uct.ac.za
ABSTRACT
Violence has been recognised officially as a global health issue, with the World Health Organization (WHO) reporting that 1.6 million people die annually from violence. South Africa's injury burden is very high, particularly for homicide, which is six times the global average. The idea of an Observatory' has expanded recently, from its origins in astronomy to that of specialised informational repositories and knowledge-building centres, housing cross-referenced databases with advanced analytic and research capacities. This review essay provides information regarding the conceptual framework, historical background and various components of the violence observatory model, as well as evidence of effect. The intention is to provide information to stakeholders within the safety and security cluster by increasing awareness of the observatory models' application in high violence and injury settings such as South Africa.
Violence is now recognised as an important public health issue across the globe, with the World Health Organization (WHO) reporting that 1,6 million people die annually as a result of violence.1 The Global Burden of Disease Study predicts that interpersonal violence will remain a top five cause of premature death in sub-Saharan Africa by 2020.2 The 2012 National Burden of Disease Study found interpersonal violence to be the eighth leading cause of overall premature death in South Africa, while being the second leading cause of premature death for males, after HIV/AIDS.3 South Africa's injury burden is very high, particularly for homicide, which is approximately six times the global average.4
South Africa is a middle-income country that is burdened with a diverse spectrum of diseases, including infectious diseases, chronic and degenerative diseases, malnutrition and childbirth-related conditions, and a disproportionately large burden of injuries.5Interpersonal violence and road traffic collisions are the leading causes of injury in South Africa.6 In 2005 39% of all injury-related deaths resulted from interpersonal violence.7 Despite the reduction in political conflict in the post-apartheid era, interpersonal violence has continued to plague South Africa, and has in fact increased in the past 20 years.8
South Africa is one of the few places in the world where rates of intentional injury exceed the rates of unintentional injury.9 Of the 52 493 injury-related deaths recorded in South Africa for 2009, almost half (25 499) were intentionally inflicted.10 Homicide was the leading apparent manner of death, accounting for 36.2% of all external causes.11 Firearm injuries were a leading cause across several categories, accounting for 6 428 deaths, equivalent to 17.6 firearm-related deaths per day. Of these, 5 513 were attributed to homicides.12 Other categories included sharp force, blunt force, strangulation, burns, other and unknown.13 Homicide rates in the Western Cape were greater than the national average for both males and females. In Cape Town, the province's largest city and home to almost two-thirds of the provincial population, the highest homicide counts for the period 2015 to 2016 were recorded in the relatively impoverished sub-districts of Nyanga (279 homicides) and Khayelitsha (161 homicides).14
While the criminal justice system remains the primary tool for responding to violence and injury in South Africa, evidence-based interventions for prevention are becoming increasingly influential in the field of public health, assuming a more central role in policymaking.15 The public health approach to violence and injury prevention consists of three elements: assessing existing conditions; developing interventions; and evaluating programme effectiveness.16Key to this approach is a surveillance system capable of providing essential information for the assessment phase in order to develop appropriate interventions and programme evaluation methods.17
Injury surveillance is widely recognised as a critical prerequisite for effective injury prevention.
Ongoing surveillance can monitor the incidence of injury, identify risk factors and contribute to the planning and evaluation of injury prevention programmes.18 Furthermore, injury surveillance can comprise a variety of data sources, from mortality and hospital discharge data to emergency department registry data, surveys and police, fire and ambulance records.
This review suggests that violence and injury observatories are key to developing interventions that reduce the burden of injury in high-risk communities. We will use the term 'observatory' to denote a surveillance system that collects data from multiple sources, for example crime, clinical and forensic data, whereas injury surveillance systems almost exclusively focus on the use of injury data alone.
In this article we will substantiate the following claims:
• The observatories model is an internationally accepted tool that can provide a focused understanding of a particular issue or sub theme of violence.
• The integration of violence and injury data may allow a comprehensive view of the existing burden of violence and injury within a community.
• Observatories allow the opportunity to monitor current and prospective violence and injury interventions.
• Observatories are a viable intervention to support the prevention of violence.
We will first review the existing global efforts and examples of observatories, using case studies from Latin America where most of them are to be found, and where the socio-economic setting is comparable with South Africa. We will then review each function of a violence and injury observatory, its place within a national health reporting system, its structure and performance, and conclude with the current evidence of effect.
Observatories for violence and injury
The meaning of an observatory has recently expanded from its origins in astronomy to that of a specialised informational repository and knowledge-building centre, housing cross-referenced databases with advanced analytic and research capacities.19
An observatory is primarily a tool to support authorities in formulating effective responses to citizen safety and security issues.20 It is a centre dedicated to systematising information from different sources to produce periodic analyses or studies that show the development of crime and violence in a given area.21 According to research completed by the International Crime Prevention Centre, an observatory has at least three basic functions: collection of data, analysis of data and public dissemination, which is directed at preventing crime and violence at a local and regional level. The crime and violence observatories developed in Colombia aim to maximise inter-institutional cooperation, information sharing, analysis and security policy development initiatives to enhance governance.22 The model is similar to those proposed on a broader level by the International Scientific and Professional Advisory Council of the United Nations (UN) at the 11th UN Congress on Crime Prevention and Criminal Justice.23
Conceptual framework for the observatory model
The concept of an urban observatory (Figure 1) has been developed to address the obstacles presented by the complex network of health determinants in urban settings, and the often dispersed and uncoordinated nature of data at the local level.25 The observatories are intended to act as a focal point for urban monitoring by assembling, analysing and producing information on health outcomes and their broad range of determinants; and mobilising a network of actors or stakeholders to take action on the wider determinants of health through better informed policies.26 Their focus is on generating information and knowledge for evidence-based health policy and decision-making.27 They work to monitor health trends; identify gaps in health information; provide guidance on appropriate methods; assemble data from different sources; and integrate population-based data (e.g. vital statistics, censuses, and social demographic surveys) and institution-based data from both within and outside the health sector.28
The violence and injury observatory model was also developed within the framework of community-oriented policing and decentralisation.29 Community-oriented policing follows a conceptual and practical shift adopted from earlier European practices and adapted to North America during the early 1970s.30 It refers to systematic support for a more cohesive, responsive, interactive and user-friendly relationship between law enforcement agencies and communities, with a strategy that generally seeks to open lines of communication with the community, produce information-sharing initiatives and improve the quality of information obtained.32
Historical background to the violence and injury observatory model
Between 1993 and 1996 the mayoral administration of Cali, the third most populous city in Colombia, instituted a programme of development, security and peace, referred to as DESEPAZ.33This programme applied a public health perspective to issues of violence prevention and intervention, influenced by the mayor's background in epidemiology, and would establish the framework for the first ever observatory dedicated to the theme of violence and injury.34 The information was subsequently validated, supplemented and utilised in weekly meetings of the city's Security Council, whose primary focus was citizen security issues; additionally, the council also sought to improve coordination and efficiency in the use of resources.35
Following a thorough review of the data, further statistical analysis led to subsequent policy planning and coordinated intervention efforts by civil authorities.36 Concurrently, structural interventions to improve police functioning through the provision of pay increases, educational opportunities and housing construction incentives were implemented.37These initiatives would provide the initial framework for later developments with the violence and injury observatory model.
In the area of international violence prevention approaches there has been growing interest on the part of governments, municipalities, research centres, civil society organisations and international organisations in creating observatories or analytical tools for security-related problems, including, but not limited to, school violence, domestic violence, drug use, and social and gender violence.39
Structure and performance of the observatory model
To illustrate the structure and performance of the observatory model, Figure 3 shows the administrative structure of the Juarez municipal violence and injury observatory in Mexico, while Figure 4 describes an observatory's functions, information sources and management. The Juarez Observatory is cited as an example, as the city's population and socio-economic conditions, as well as its homicide rate, are comparable to municipalities within South Africa's four major cities. Additionally, the formation of the observatory within a resource-limited setting provides a blueprint for the establishment of observatories in similar settings in South Africa. Violence in Juarez, one of the largest cities in Mexico, increased significantly from 2007 to 2010, with the homicide rate increasing from 23 to 224 per 100 000 inhabitants.40 This situation triggered the creation of the Juarez Observatory in 2008, in a joint effort between the Juarez Municipal Government, the Autonomous University of Ciudad Juarez and the Pan American Health Organization (PAHO).42 From 2010 to 2015 the homicide rate dropped from 282 to 18 murders per 100 000 inhabitants.
Observatory function 1: collection, integration and storage of secondary data and information
A predefined list of data and indicators, such as the 22 Citizen Security Indicators agreed to by the Organization of American States (OAS), can be adapted from those used in international initiatives.43 Examples of indicators related to violence include homicide rate per 100 000 inhabitants, prevalence of intra-family/family and domestic violence, rate of criminal victimisation in people older than 18 years, and percentage of perceptions of insecurity in people older than 18 years.44 Data quality and completeness could vary between different administrative levels, geographical areas and specific systems, with the quality of information collected at the observatory depending on how the different sources have integrated and consolidated the information.45
Agreement on information sharing facilitates the systematic data flow between information sources and the observatory central management unit. A fully functioning observatory will allow for the accumulation of electronically stored data, thereby providing the capacity to build a historical database.46Textual information, databases, historical trends in data and indicators, profiles, reports and other sources may convert the observatory into a powerful information and knowledge management centre.47
Observatory function 2: data analysis
A range of multi-sectoral, multidisciplinary sources of information may be analysed, using quantitative and qualitative analysis methods for the purposes of (a) identifying patterns and trends over time in the incidence of violence, (b) monitoring and evaluating interventions and policies, (c) understanding the causes and determinants of violence, and (d) developing a set of common indicators and standardised definitions.48
Advanced data analysis methods for surveillance data include space-time clustering, time-series analysis, geospatial analysis, life tables, logistic regression, trend and small area analysis and methods for the forecast of epidemics based on surveillance data.49Statistical analysis can be performed by the observatory central team or by external groups such as those working in monitoring and surveillance, using user-friendly software such as Epi-Info or SPSS®. A Juarez study, using qualitative methodology, explored how families' economic, social and cultural capital had been disrupted by violence and how it affected children's well-being.50 The conclusions of the research was that social and economic capital declined significantly because of the violence and crime that families experienced, that violence made it more difficult to find and maintain employment, and decreased their interactions outside the home, with cultural capital diminishing as a result of the isolation.51
Observatory function 3: reporting on and disseminating information and knowledge
The objectives of the dissemination of information are to (a) inform stakeholders of important issues and trends, (b) influence public policy, (c) develop evidence-based interventions and policy recommendations, and (d) assist collaborating agencies and other stakeholders to improve their operations and understanding of the issue through provision of an up-to-date, reliable evidence base.52
The communication of information to contributors and users of surveillance data is integral to programme planning and decision-making. Examples of users include public health practitioners, health planners, epidemiologists, clinicians, researchers, policymakers, data collectors, members of the public, and the media.53 Different communication vehicles exist, including formal surveillance reports or bulletins, annual reports, teleconferences with partners, media conferences, media releases and public advisories.54 The experience of the Juarez Observatory has shown that even in complex situations it is possible for academic institutions, international organisations, and diverse governmental and non-governmental institutions and organisations to combine efforts and collaborate.55 This high spirit of co-operation and sharing and dissemination of data contributed to the decline of road accidents related to drunk driving over a three-year period from 2009 to 2011, and a decline in the homicide rate over a five-year period from 2010 to 2015.56
Observatory types and proliferation of the observatory model globally
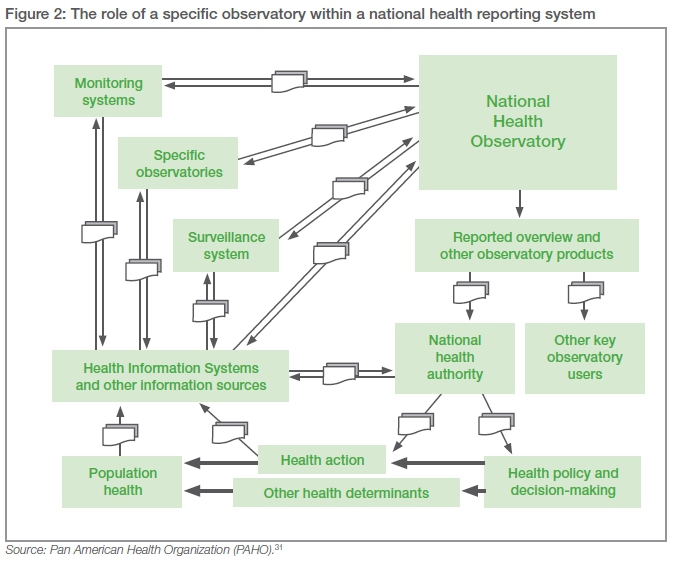
There are various types of observatories, such as governmental, university or combined models.57 Observatories can operate on different levels, including local, regional, national and international (Figure 2). There are also generalist observatories (for violence, security, crime, etc.) or thematic ones (for school violence, domestic violence, trafficking in goods, trafficking in persons, organised crime, etc.).58 There are also centres that perform the same work as an observatory but are not necessarily called observatories. Currently there are 27 global observatories (Table 1), disseminating research on best practices, policies and programming for democratic governance; numerous public health observatories, including an European Union observatory on health systems and policies; a global urban development observatory sponsored by the UN; as well as numerous local, regional, national and international observatories addressing crime and security measures.59
The Geneva Declaration on Armed Violence and Development, endorsed by more than 100 countries, commits signatories to 'support initiatives intended to measure the human, social and economic costs of armed violence, to assess risks and vulnerabilities, to evaluate the effectiveness of armed violence reduction programmes, and to disseminate knowledge of best practices'. This declaration describes a significant function of violence and injury observatories.60 Furthermore, the observatory model has been proposed at a broader level by the International Scientific and Professional Advisory Council of the UN at the 11th UN Congress on Crime Prevention and Criminal Justice.61
Several factors have contributed to the global growth and expansion of this model. One of the global outcomes of the Square Kilometre Array research project in South Africa, which is responsible for collecting and housing the largest database ever recorded in human history, is the reduction in costs of cloud computing when processing and analysing large datasets.62 Additionally, the growth of public health surveillance systems globally has been disseminated and supported by organisations such as the WHO, the Centers for Disease Control and Prevention in the US and the International Centre for the Prevention of Crime in Canada.63 Finally, the expansion of information and communications technology (ICT) infrastructure in the developing world has grown, including in South Africa, which, according to the 2013 Global Information Technology Report published by the World Economic Forum (WEF), ranks 50 out of 144 countries when it comes to ICT infrastructure and digital content.
Evidence of effect
Despite the proliferation of various observatory models, there is little published research on their effectiveness in producing or stimulating the production of demonstrable social change and decreasing levels of violence and crime.64 In 2012 Gutiérrez and colleagues illustrated that the implementation of a violence and injury observatory based on the Juarez Observatory could effectively reduce violence.65 In addition, several observational studies have shown a reduction of violence associated with the implementation of observatory/surveillance systems.66
To date, there has been no systematic analysis of the literature to present a succinct review of the evidence. With other colleagues, in 2015 we published the first systemic review protocol to investigate the effectiveness of observatories in reducing violence, 'Effectiveness of violence and injury observatories in reducing violence in an adult population'.67 This systematic review will seek to summarise the evidence from existing studies on the contribution of violence and injury observatories to violence prevention in adult populations.
Conclusions and further work
This article introduces the observatory model as an internationally accepted tool to study and prevent violence as a public health issue. The model can be applied to specific types of violence within different socio-economic settings. Furthermore, the integration of violence-related data from different data sources and stakeholders allows for routine services such as monitoring and evaluation, but also extends to the use of advanced analytical methods employing GIS, epidemiology and database mining. Within high-risk communities, such as those in the cities of Juarez in Mexico and Cali in Colombia, the observatory model serves as a viable intervention and tool to address the burden of injury. Based on these potential benefits and the public health imperative to address the high rate of violence and injury in South Africa, the Cape Town Violence, Injury and Trauma Observatory (VITO) is proposed as the first non-conflict observatory on the African continent.68
Notes
Funding
The PhD from which this review emanated was funded by the Medical Research Council (MRC) of South Africa under the MRC Clinician Researcher Programme.
1 M Peden, K McGee and E Krug, Injury: a leading cause of the global burden of disease, Geneva: World Health Organization (WHO) Publications, 2002, 1-2. [ Links ]
2 C Murray and A Lopez, Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study, Lancet, 349:9064, 1997, 1498-1504. [ Links ]
3 Ibid.; R Matzopoulos et al., Injury-related mortality in South Africa: a retrospective descriptive study of postmortem investigations, Bull World Health Organ, 93:5, 2015, 303-313. [ Links ]
4 Matzopoulos et al., Injury-related mortality in South Africa.
5 P Brysiewicz, Trauma in South Africa, Int J Trauma Nurs, 7:4, 2001, 129-132; [ Links ] J Goosen and E Al, Trauma care systems in South Africa, Injury, 34:9, 2003, 704-708. [ Links ]
6 Matzopoulos et al., Injury-related mortality in South Africa; Goosen and Al, Trauma care systems in South Africa; A Brooks, C Macnab and K Boffard, South Africa, Trauma Q, 14:3, 1999, 301-310; [ Links ] B Meel, Pre-hospital and hospital traumatic deaths in the former homeland of Transkei, South Africa, J Clin Forensic Med, 11:1, 2004, 6-11. [ Links ]
7 R Matzopoulos et al., The Injury Mortality Survey: a national study of injury mortality levels and causes in South Africa in 2009, Cape Town: WHO Publications, 2013, 303-313. [ Links ]
8 Ibid.; R Norman et al., The high burden of injuries in South Africa, WHO Bull, 85:9, 2007, 695-701. [ Links ]
9 WHO, World health statistics, Luxembourg: WHO, 2015, 110. [ Links ]
10 Matzopoulos et al., Injury-related mortality in South Africa.
11 Ibid.
12 Ibid.
13 Ibid.
14 South African Police Services, South African crime statistics 2015/16, https://www.saps.gov.za/services/crimestats.php <https://protect-za.mimecast.com/s/l1pRBnsmw3ZS2> (accessed 31 March 2017).
15 B Holtmann and C Domingo-Swarts, Current trends and responses to crime in South Africa, Johannesburg: Medical Research Council (MRC), 2008, 131-159. [ Links ]
16 EG Krug et al., World report on violence and health, Geneva: WHO Publications, 2002, 7-9. [ Links ]
17 Ibid.
18 C Macarthur and IB Pless, Sensitivity and representativeness of a childhood injury surveillance system, Inj Prev, 5, 1999, 214-216; [ Links ] T Driscoll, J Harrison and J Langley (eds), The scientific basis of injury prevention and control communications, Melbourne: IP Communications, 2004, 87-109. [ Links ]
19 MI Gutierrez-Martinez et al., The evaluation of a surveillance system for violent and non-intentional injury mortality in Colombian cities, Int J Inj Contr Saf Promot, 14:2, 2007, 77-84. [ Links ]
20 Organization of American States (OAS), Manuä for the creation of national public security observatories on crime and violence, Washington DC: OAS, 2009, 21. [ Links ]
21 Ibid.
22 Gutierrez-Martinez et al., The evaluation of a surveillance system for violent and non-intentional injury mortality in Colombian cities.
23 Norwegian Ministry of Foreign Affairs, Measuring and monitoring armed violence: goals, targets and indicators, Oslo Conference on Armed Violence, Background Paper, Geneva: UN Development Programme (UNDP), April 2010, 32. [ Links ]
24 WT Caiaffa et al., Developing a conceptual framework of urban health observatories toward integrating research and evidence into urban policy for health and health equity, J Urban Health, 91:1, 2014, 1-16. [ Links ]
25 Z Ross, T Matte and H Kitson, Taking the pulse of an urban world: mechanisms for characterizing urban health and urban health equity, Kobe: WHO, 2011, 4-6. [ Links ]
26 Caiaffa et al., Developing a conceptual framework of urban health observatories.
27 Ross, Matte and Kitson, Taking the pulse of an urban world; Pan American Health Organization (PAHO), Implementing national health observatories: operational approach and strategic recommendations, Chile: WHO, 2009, 1; [ Links ] D Vlahov and W Caiaffa, Healthy urban governance for population health in Belo Horizonte: participatory budgeting, London: Earthscan, 2012, 63-81. [ Links ]
28 Caiaffa et al., Developing a conceptual framework of urban health observatories.
29 Gutierrez-Martinez et al., The evaluation of a surveillance system for violent and non-intentional injury mortality in Colombian cities.
30 Ibid.
31 Pan American Health Organization (PAHO), Implementing national health observatories: operational approach and strategic recommendations.
32 Ibid.
33 Ibid.
34 Ibid.
35 Ibid.
36 Ibid.
37 BA Sklaver et al., The establishment of injury surveillance systems in Colombia, El Salvador, and Nicaragua (2000-2006), Rev Panam Salud Publica, 24:6, 2008, 379-389. [ Links ]
38 LA Gutierrez et al., Using evidence on violence and injury prevention for policy development and decision making in Ciudad Juarez, Mexico, Rev Panam Salud Publica, 31:5, 2012, 365-372. [ Links ]
39 Prince, Crime observatories.
40 LA Gutierrez et al., Using evidence on violence and injury prevention for policy development and decision making in Ciudad Juarez.
41 PAHO, Implementing national health observatories.
42 Norwegian Ministry of Foreign Affairs, Measuring and monitoring armed violence; Inter-American Development Bank (IADB), Citizen security and justice, http://www.iadb.org/en/topics/citizen-security/citizen-security-indicators,2666.html (accessed 6 March 2017).
43 IADB, Citizen security and justice.
44 PAHO, Implementing national health observatories.
45 Ibid.
46 Ibid.
47 Ibid.
48 IADB, Citizen security and justice.
49 BCK Choi, The past, present, and future of public health surveillance, Scientifica (Cairo), 2012, 1-19. [ Links ]
50 AA Hernandez and SE Grineski, Disrupted by violence: children's well-being and families' economic, social, and cultural capital in Ciudad Juarez, Mexico, Rev Panam Salud Publica, 31:5, 2012, 373-379. [ Links ]
51 Ibid.
52 Department for International Development, Tools for measurement, monitoring and evaluation: sources of conflict, crime and violence data, London: UK Aid, 2013, 22-24. [ Links ]
53 LW Chambers et al., Health surveillance: an essential tool to protect and promote the health of the public, Can J Public Heal, 97:3, 2006, 2-8. [ Links ]
54 Ibid.
55 Gutiérrez et al., Using evidence on violence and injury prevention for policy development and decision making in Ciudad Juarez, Mexico.
56 Ibid.
57 OAS, Manual for the creation of national public security observatories on crime and violence.
58 Ibid.
59 Gutierrez-Martinez et al., The evaluation of a surveillance system for violent and non-intentional injury mortality in Colombian cities. www.uclg.org; www.euro.who.int; www.unhabitat.org; http://www.unicri.it/in_focus/on/Urban_Security http://www.hsrgroup.org/.
60 E Gilgen and L Tracey, Contributing evidence to programming: armed violence monitoring systems, Geneva: UNDP, 2011, 9. [ Links ]
61 United Nations (UN), Eleventh United Nations Congress on Crime Prevention and Criminal Justice, Bangkok, 2005. [ Links ]
62 R Newman and J Tseng, Cloud computing and the Square Kilometre Array, Square Kilometre Array, Memo 1334, May 2011, https://www.skatelescope.org/uploaded/8762_134_Memo_Newman.pdf (accessed 6 March 2017).
63 IIADB, Citizen security and justice.
64 Gutiérrez et al., Using evidence on violence and injury prevention for policy development and decision making in Ciudad Juarez, Mexico.
65 Ibid.
66 Sklaver et al., The establishment of injury surveillance systems in Colombia, El Salvador, and Nicaragua; Gutiérrez et al., Using evidence on violence and injury prevention for policy development and decision making in Ciudad Juarez, Mexico.
67 A Jabar et al., Is the introduction of violence and injury observatories associated with a reduction of violence in adult populations? Rationale and protocol for a systematic review, BMJ Open, 5, 2015, 1. [ Links ]
68 A Jabar and R Matzopoulos, Rationale and design of the Violence, Injury and Trauma Observatory (VITO): The Cape Town VITO Study (the manuscript has been submitted and is currently under review at BMJ Open).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}