










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Crime Quarterly
On-line version ISSN 2413-3108
Print version ISSN 1991-3877
SA crime q. n.51 Pretoria Mar. 2015
http://dx.doi.org/10.4314/sacq.v51i1.2
Spare the rod and save the child assessing the impact of parenting on child behaviour and mental health
Catherine L WardI; Chandré GouldII; Jane KellyIII; Katya MauffIV
IDepartment of Psychology and the Safety and Violence Initiative at the University of Cape Town. catherine.ward@uct.ac.za
IISenior research fellow in the Governance, Crime and Justice Programme at the Institute for Security Studies. cgould@issafrica.org
IIIDoctoral student in the Department of Psychology at the University of Cape Town. janekelly88@gmail.com
IVConsultant in the Department of Statistical Sciences at the University of Cape Town at the time of this study. She is now a doctoral student in statistics at the University of Rotterdam. katya.mauff@gmail.com
ABSTRACT
Parenting has a considerable impact on children's behaviour and mental health. Improving child health and behaviour requires an understanding of the relationship between parenting practices; contexual factors such as parental mental health, intimate partner violence, substance abuse and poverty; and children's behaviour. In this article the authors report the findings of a survey of parenting and child behaviour in a small rural South African community. The findings show that corporal punishment, the stress of parenting and parental mental health are significantly associated with both children's internalising (depression and anxiety) and externalising (rule-breaking and aggression) symptoms. Intimate partner violence in the home was also associated with children's externalising symptoms. These findings imply that parent support and training, and an increase in services to address intimate partner violence and mental health problems, should be prioritised as part of a national violence reduction strategy.
Parenting can have profound effects on children's mental health and behaviour. Harsh, cold and inconsistent parenting increases the risk that children will develop both externalising disorders (behavioural problems such as aggression)1 and internalising disorders (anxiety and depression).2 Both types of disorder can have serious, lifelong consequences for the individual, family and society, since they affect survival, ability to succeed at education, and employability.3 In light of the high levels of violence, HIV infection, substance misuse and skills shortages in South Africa, preventing these problems is critical.4
Inconsistent discipline, poor monitoring and supervision, and harsh punishment (including corporal punishment) all increase the risk that children will develop a disorder:5
- Inconsistent discipline has been linked to aggression and other problem behaviours.6 When parents make and apply rules for children inconsistently, children And it difficult to understand the link between their behaviour and its consequences.7
- Failing to monitor a child's or adolescent's whereabouts, companions and activities is a very strong predictor of behavioural problems, probably because it removes the opportunity for parents to teach children how to manage their own behaviour and to choose friends wisely.8
- Corporal punishment has been shown in a number of studies to increase risk for behavioural problems.9
The specifics of these interactions are likely to change as children age. For instance, harsh parenting of a young child may be more likely to include spanking while harsh parenting of a teenager may include more psychological abuse - but harsh, inconsistent discipline at any age has been shown to promote bad outcomes.
On the other hand, positive parenting - when parents are warm and affectionate and have positive interactions with their children - promotes good outcomes for children.10
Many parents face a number of stressors that can undermine positive parenting. Single parenting, for instance, reduces social support for parents, and is likely to be associated with economic stress.11 Poverty affects parenting in a number of ways, largely through increasing the stress of parenting. Parents living in poverty are more likely to be depressed, which increases the likelihood of harsh, inconsistent parenting.12 They are also less likely to have the social support that may ease the stress of parenting,13 and are less likely to be warm towards their children or to monitor them sufficiently.14 Both single parenting and poverty are widespread in South Africa,15 as are other, related, problems - intimate partner violence, mental health problems and substance misuse16 - all of which make parenting more difficult. For instance, intimate partner violence increases the stress of managing parenting tasks, both because of the effect it has on the parent victim and because children's behavioural problems may increase when they are exposed to violence in the home, as they may model the abuser's behaviour.17 In addition, children of parents who are mentally ill may be affected both through direct exposure to distressing symptoms and through disruptions to parenting.18 Substance abuse also affects parenting, as it may reduce inhibitions in parents, making them more likely to be abusive to their children.19
Several studies have explored parenting and children's related problems in South Africa. One study has found that violence at home is associated with both the severity and early age of onset of offending,20 and another identified inadequate parenting in populations of young South African offenders.21 Poor parental supervision has been found to be associated with adolescent antisocial behaviour, while parental support has been found to protect against such behaviour.22
A study of a Johannesburg birth cohort found that corporal punishment was associated with children's behavioural difficulties, and contextual stressors were affecting parenting of young children.23 Finally, conflict between parents has been identified as affecting both externalising and internalising symptoms in South African children, both directly and via parenting.24
However, these studies either focus on young offenders, or have not been replicated elsewhere in South Africa, or do not examine both contextual stressors and parenting, or only examine one outcome in children (typically aggression). We sought, therefore, to explore parenting, and its association with children's externalising and internalising disorders, in an entire South African community.
Methods
This study was conducted in a small township in the rural Western Cape. The research process consisted of four phases: a door-to-door community audit conducted in June/July 2012; two surveys of all households in which there were children aged six to 18; and focus group discussions with community members after Survey 2. The community audit showed that there were 304 households in the township with children between the ages of six and 18. This age group was chosen as the measures of parenting and of child behaviour that we were using were all valid for this group.
Survey 1 was conducted in August 2012 and Survey 2 in March 2013. In this article, we report only on Survey 2, as focus group data indicated that it had greater validity.
Participants
We surveyed one caregiver in each household. Each caregiver was asked to answer questions only about the youngest child in the home aged between six and 18.
The study was approved by the Research Ethics Committee of the Faculty of Humanities at the University of Cape Town. Each caregiver gave informed consent for participation. Provision was made for participants to get help from local child protection agencies in the event that we identified a parent as abusive.
Measures
Parenting was assessed using the Alabama Parenting Questionnaire, designed to assess the kinds of parenting that can either reduce or increase the risk of aggression in children.25 Each response was assessed on a 5-point scale, so that parents were able to choose one of the answers 'never', 'seldom', 'sometimes', 'often', or 'always'. The Parenting Stress Index was used to assess how stressful the caregiver found the task of parenting.26 This scale has clinical cut-offs for the total score and one of the three subscales, Parent-Child Dysfunctional Interactions; the latter cut-off allows one to identify parents at risk of abusing their children.
Children's externalising (aggressive and rule-breaking behaviour) and internalising (anxiety and depression) were assessed using the Child Behavior Checklist.27 Parents were asked to respond to a statement about their child's behaviour (e.g., 'argues a lot') by choosing one of three options: 'not true', 'somewhat or sometimes true', or 'very true or often true'. Children's behaviour could then be assessed to determine whether it fell into a clinical range (a range that indicates that the attention of a mental health professional is necessary). The Child Behavior Checklist has been found to be reliable in a wide range of countries.28
Contextual variables that might affect parenting were also explored. These included the 28-item version of the General Health Questionnaire, an assessment of the caregiver's own anxiety and depression, which was used as a continuous score in the analyses but which also allows identification of clinical cases (i.e., that a mental health professional would be very likely to diagnose the respondent with a psychiatric disorder).29 The Alcohol, Smoking and Substance Involvement Test (ASSIST)30 assessed caregivers' substance misuse; scores were used as a continuous variable in the analysis, but the ASSIST allows categorisation of scores into low- or no-risk, moderate risk or high-risk use of a particular substance; these scores correspond, respectively, to those who need no intervention for substance misuse, those for whom a brief intervention is appropriate, and those who need an intensive intervention.31 Thirty-two items from the Revised Conflict Tactics Scale (CTS-2) were used to assess the caregiver's experience of intimate partner violence,32 and used as a continuous variable in the analysis. A variable indicating whether the caregiver was a single parent was also included.
Poverty was measured using a modified asset index approach, constructed using multiple correspondence analysis. In addition to a household inventory of assets,33 the following were included: sources of household income, employment status of respondent, and a hunger scale that explored whether family members had ever gone to bed hungry through lack of food.34 The first dimension of the multiple correspondence analysis was used as the poverty variable, explaining 51% of the variability in the data. Higher values of the composite measurement are indicative of greater wealth.
Other demographic variables included in the analysis were the child's age and gender, the caregiver's relationship to the child, and how many other children there were in the household. Questionnaires were translated into Afrikaans and isiXhosa, with translations checked by back-translation.
Procedure
To conduct the survey, we selected as fieldworkers community members associated with a respected non-profit organisation that provides youth development activities to the community's children. Fieldworkers were trained in ethics and in interviewing skills. All questionnaires were administered as interviews by fieldworkers because we expected a low level of literacy among caregivers. Interviews took about two hours, and were conducted in private. A small incentive (some biscuits) was provided to each caregiver interviewed. Fieldworkers provided respondents with a list of local organisations that provide support around parenting, intimate partner violence and substance misuse.
Five focus group discussions were held with 20 caregivers who had also completed the survey. Community members were recruited to participate in these through an announcement at a public meeting, and flyers were distributed throughout the community, inviting anyone who had been interviewed to attend. Only women volunteered to participate. A small incentive was offered: all participants were given a R50 voucher for a local clothing store. Three themes were explored in these discussions: what it had been like to complete the questionnaires; what methods of discipline were primarily used in the community; and what stressors affected parenting in the township. Participants gave separate informed consent to participate in the focus group discussions.
Data analysis
The focus group discussions were transcribed and analysed using thematic analysis. Thematic analysis involves identifying, analysing and reporting specific patterns (themes) across participants, where a theme refers to a coherent pattern that captures something important in relation to the research questions of the study.35
Before embarking on the quantitative analyses, the data was checked to see whether it met the requirements for regression. Cronbach's alphas for the Alabama Parenting Questionnaire subscales were very low, and Rasch analysis of the Alabama Parenting Questionnaire data (using the eRm module in R) revealed that the 5-point response options appeared to have been confusing for parents. For instance, it appeared that the distinctions between 'never' and 'seldom' had been difficult to make. We therefore collapsed the scores so that 'never' and 'seldom' became one response, and 'often' and 'always' also became one response. This meant that the answers to the Alabama Parenting Questionnaire were effectively reduced to three options: 'never' or 'seldom'; 'sometimes'; and 'often' or 'always'. Cronbach's alphas for the recoded parental involvement and positive parenting subscales were 0.860 and 0.873 respectively. However, Cronbach's alphas for poor monitoring and supervision, inconsistent discipline, and corporal punishment all remained below 0.7. For this reason, the first of these two subscales were not used in analyses and we treated corporal punishment as individual items. Mild forms of corporal punishment - spanking and slapping - were grouped separately from the third corporal punishment item, which dealt with beating a child with an object. For the purposes of regression analyses, these were recoded as dummy variables -'always spanks or slaps' and 'sometimes spanks or slaps', as a form of punishment.
Cronbach's alphas for all other scales were above 0.8. Both scales representing children's behaviour (internalising and externalising) were very skewed, so logarithmic transformations were used to improve the normality of the distributions. All the variables (except the two corporal punishment variables) were centred before being entered into the analysis. In all cases, except corporal punishment and gender, variables were used in their continuous form in the analyses.
Model building was done as follows (using SPSS v22): first the bivariate relationships between each variable and each of the children's behaviour were investigated, using Pearson correlations. Once relationships had been identified in significant bivariate models, regression was used to explore, in separate models, the relationships between parenting (the subscales of the Alabama Parenting Questionnaire) and child behaviour (internalising or externalising), as well as the effects of the contextual variables (poverty, the stress of parenting, parental mental health, parents' experiences of intimate partner violence, and parents' substance misuse). In each case, the child's age and gender were retained in the models, as these typically have strong relationships to children's externalising or internalising behaviour.36
In terms of the parenting variables, positive parenting, parental involvement and harsh corporal punishment ('You hit your child with an object') were not found to be significantly associated with either child externalising or internalising behaviour and so were excluded from the final models. We then ran a model with only the contextual variables (keeping child age and gender as constants) to see whether they were predictive of child outcomes: poverty, parental substance use and single parenthood were not significant predictors of child externalising and internalising behaviour and so were also excluded from the final models. At each stage where variables were removed from the models, models with and without those variables were compared using appropriate statistics (AIC, BIC and adjusted R-squared).
Next, the enter method of regression was used to develop a final model that explored relationships between all the variables that had been significantly associated with children's outcomes in the earlier models. Variables were entered into the regression model in the following blocks: first child age and gender, followed by parenting, followed by the contextual variables. Since 64 of the 220 respondents did not answer the questions about intimate partner violence, we ran one model for externalising behaviour that included intimate partner violence (and therefore reflected the subsample that answered these questions), and another that did not (and therefore reflected the full sample). Only one model was used to explore internalising behaviour, as bivariate analyses showed no relationship between intimate partner violence and internalising disorders.
The total number of cases included in each model was 220, and missing data were excluded, using listwise deletion. Influential outliers were excluded from all models. Influential outliers were identified by plotting Cook's distance against the standardised residual; this identified those cases that may influence models so much that the models then apply only to those individuals, rather than to most people in the township. In the externalising model that included intimate partner violence, one outlier was excluded; in the externalising model that excluded intimate partner violence two were excluded; and in the model for internalising disorders four cases were excluded.
Results
Description of the sample
In 71 homes we did not And a child in the age group 6-18, and in those cases the household was excluded. Fifteen caregivers surveyed in Survey 1 could not be followed in Survey 2 (six refused to participate and nine were not available), and two new caregivers were identified, leaving us with a sample of 220 caregivers and their children. The sample included 217 Afrikaans- and three isiXhosa-speaking caregivers.
Of the children included in the sample, 106 (49.8%) were female and 107 (50.2%) male; in seven cases, caregivers did not report either age or gender. Because this data was missing, these cases were excluded from the analyses. In terms of ages reported, children included in the study covered the full possible age range, from six to 18, with a mean reported age of 10.5 (standard deviation 3.2). Of the 216 caregivers who reported their relationship to the child, the majority (195; 90.3%) were the biological parent of the child. The remaining 21 caregivers were step-parents, grandparents and adoptive or foster parents. Most (187; 86.6%) households included one, two or three children, although some reported up to six children. The majority of caregivers (163; 75.5%) reported that another adult in the household assisted with childcare, although 59 (25.7%) reported that they were single. Nearly half (87; 40.3%) of the children's fathers were unemployed, and of those who were employed the majority (63; 54.3%) did unskilled manual labour. Similarly, 123 (56.9%) of the children's mothers were employed, 70 (59.3%) as domestic workers.
In Survey 2 we had 213 children for whom we were able to collect data on the Child Behavior Checklist. The possible range for scores on the externalising subscales was 0-64, and on the internalising subscales 0-74. Parents reported a maximum score of 56 for externalising (with a mean of 7.6 and a standard deviation of 8.4), and a maximum score of 47 for internalising (mean of 5.5, standard deviation of 6.4). These scores were broken down by gender, and by whether children were in need of attention from a mental health professional (Table 1). In total, 13 (6.1%) of the children fell into the borderline clinical range for internalising disorders (a range where the attention of a mental health professional may be helpful) and 26 (12.2%) of the children into the clinical range (a range that indicates that a mental health professional is likely to diagnose a formal mental health disorder). Slightly more children suffered from externalising disorders: 20 (9.4%) fell into the borderline clinical range, and 27 (12.7%) into the clinical range. Some children met criteria for the borderline or clinical range for both internalising and externalising disorders, so that a total of 21 children (9.9%) were identified as falling into either the borderline or clinical ranges for both disorders. If attention was restricted only to those who met the narrow criterion of being in the clinical range for either externalising or internalising disorders, 44 children (20.7%) were likely to have diagnosable mental health problems.

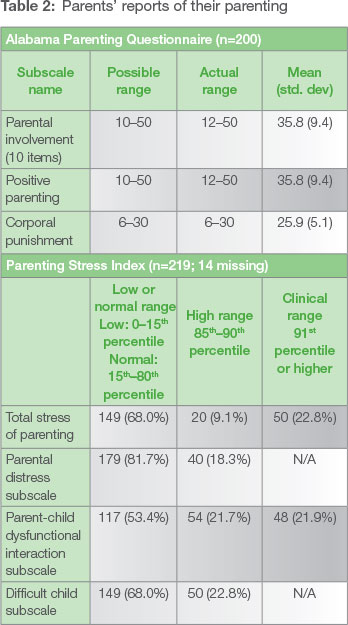
On the Alabama Parenting Questionnaire, parents reported, on average, involvement with their children a little more than 'sometimes'; positive parenting 'often'; and corporal punishment between 'never' and 'sometimes' (see Table 2 for details). Parents' reports on the Parenting Stress Index indicated that most parents did not find parenting particularly stressful (see Table 2 for details). However, over one-fifth of parents reported that they found dealing with their child difficult, and almost one-fifth that they were very stressed by parenting their child. Over one-fifth of parents reported such high levels of stress that they were in the clinical range for this; and one-fifth reported such high levels of dysfunctional interactions with their children that they could be regarded as being at risk of abusing their children. However, 68 (32.2%) of parents reported never spanking their children as a punishment, while 58 (27.5%) reported always using spanking or slapping as a punishment.
Contextual variables that could affect parenting - parents' mental health, experiences of intimate partner violence, and substance misuse - are reported in Table 3. Most parents reported good mental health, but using the clinical cut-off of a score of 5, as suggested by the developers of the 28-item General Health Questionnaire for identifying those with a diagnosable mental health problem,37 19 parents (8.6%) fall into this category.
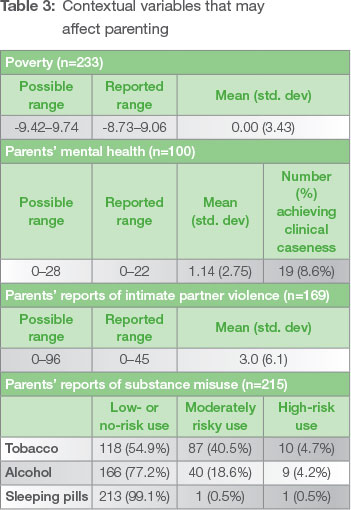
Only 169 parents answered the questions about intimate partner violence. On average, reported rates were very low, with the majority of parents (111; 47.6%) reporting no violence between them and their partners. The most frequent forms of violence that were reported included shouting and yelling between partners, partners insulting or swearing at each other, stomping out of the house during an argument, and pushing, shoving or slapping each other. However, some experiences of extreme violence were reported, in each case by only one person. These included one partner choking the other, one partner threatening the other with a knife or a gun, or one partner beating the other up.
In terms of substance misuse, tobacco was the most frequently reported substance used, followed by alcohol. Of the 215 parents who reported alcohol use, 49 (22.8%) reported using it at risky levels. Two parents (1%) also reported risky levels of use of sleeping pills, and 97 parents (45.2%) reported using tobacco at moderate or highly risky levels. Of the drugs that parents reported using, only alcohol is likely to be associated with difficulties in parenting,38 and so only their reported alcohol use was used in further analyses.
Focus group results
The focus group discussions explored three areas: stressors affecting parenting in the township; what is was like to complete the questionnaires; and methods of discipline used in the community. Data from these discussions showed that several stressors appeared to affect parenting in the township community, including low income, infidelity of intimate partners, and feeling unsupported (both emotionally and financially) by one's partner. For instance, one participant noted that in the community there were 'vaders wat nie support wil betaal nie. Hier is baie single moeders' [fathers that do not want to pay child support. Here there are a lot of single mothers]. The participants felt that this lack of emotional and financial support from fathers had a negative effect on their parenting.
The discussions also showed that some community members were concerned about how their personal information would be used after being surveyed. For example, one participant noted: Ek was n bietjie bekommerd' [I was a bit worried]. This concern may have contributed to higher reports of positive parenting and parental involvement - community members who feared what would be done with their survey information may have wished to create a good impression through emphasising their parenting abilities. It also may have inhibited some participants in answering certain questions, particularly those pertaining to their use of corporal punishment, their experiences with domestic violence, and their substance use and misuse. Indeed, participants from several groups reported that these questions could have made community members feel uncomfortable. As one participant said: Hulle sal nie daai vrae beantwoord nie, ek glo nie. Hulle sal stil biy' [They would not answer those questions, I don't believe. They would keep quiet].
This discomfort, coupled with the concern about what would be done with personal information, may have contributed to the under-reporting in the survey of corporal punishment, substance use and domestic violence in this community. The discussion by the focus group participants seemed to indicate that there were far more parents who used corporal punishment when disciplining their children, who used substances, and who experienced domestic violence, than might have been reported in the survey. When discussing forms of discipline one focus group participant said: Hier is hope wat die kinders slaan' [Here there are many who hit their children]. When talking about drinking and drug use one community member noted: 'Hier is baie mense wat drink' [here there are many people who drink], and another reported: 'Die plek is besmet van dwelms' [This place is infested with drugs]. And when discussing domestic violence, one participant noted: Dit gebeur maar baie' [It happens a lot].
Parenting and contextual variables and their effects on children
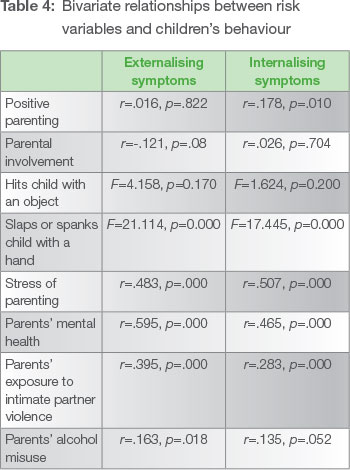
Bivariate relationships between the variables and children's behaviour are presented in Table 4. Relationships reported here are Pearson's correlations, with the exception of the corporal punishment variables where we used regressions that included only one variable as a predictor. Corporal punishment (slapping, spanking or hitting the child with an object), stress of parenting, intimate partner violence and parents' alcohol misuse were all positively associated with externalising symptoms. Positive parenting, slapping or spanking, stress of parenting, and parents' exposure to intimate partner violence were all positively associated with internalising symptoms. However, in the regression models that included child age and gender, positive parenting, parent involvement, hitting the child with an object, and parents' alcohol use were not found to be associated with children's externalising and internalising symptoms, and so were excluded from future models. The final models are shown in Tables 5 and 6.
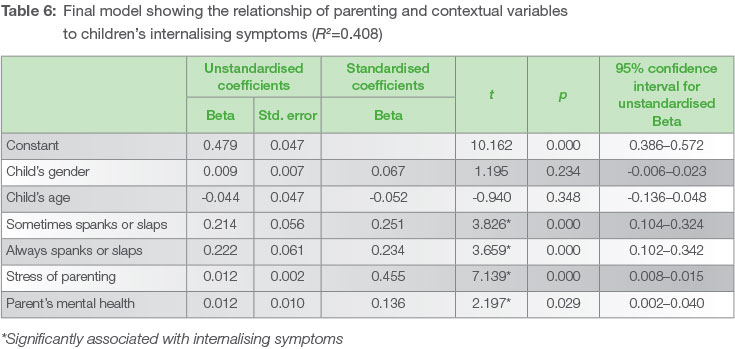
Neither child age nor child gender was significantly associated with externalising or internalising symptoms. In the model that included intimate partner violence, it was significantly associated with externalising symptoms. In both the models that included and excluded intimate partner violence, spanking or slapping (whether always or sometimes), stress of parenting, and parental mental health were all associated with externalising symptoms. With the exception of intimate partner violence, the same variables were associated with children's internalising symptoms.
Discussion
In summary, our community-wide survey found that spanking and slapping, stress of parenting, and parental mental health are significantly associated with both children's internalising and externalising symptoms. In addition, intimate partner violence in the home was associated with externalising symptoms in the subsample that responded to this question. The child's age and gender, positive parenting, parents' involvement with their children, the caregiver's status as a single parent, poverty and parental substance misuse were not significantly associated with children's symptoms. Based on the self-report of caregivers, the study also found that more than one-fifth of children living in the township would benefit from mental health treatment, as would more than one in 11 caregivers.
Children's mental health
In a large study assessing children's problems across 31 countries, including Ethiopia (the only African country included in the study), the means for both internalising and externalising were both 6.2, and did not differ significantly by age and gender.39 In the current study, children's mental health appears to follow similar patterns.40 It is not unusual that there were children who were in the clinical range for both internalising and externalising disorders: depression, for instance, is strongly related to behavioural problems, particularly in boys.41
The high rate of mental health problems among the township's children is cause for concern. This township is rural, and rates of mental health disorders tend to be lower in rural settings.42 In 2012, 54.6% of South African children lived in urban areas and may therefore have higher rates of mental health symptoms than children in the township where the survey was conducted.43 What is most interesting about children in this township, and what is likely to generalise to other areas of South Africa, is the relationship between children's symptoms, the parenting they receive, and the contextual stressors that also may affect those symptoms. This points the way both to interventions for those children who are currently suffering these problems and to interventions that may prevent them from occurring in other children.44
The effects of parenting on children's mental health and behaviour
Positive parenting and parental involvement are protective factors that are both consistently identified in the literature as reducing youth externalising45 and internalising disorders.46 It is therefore surprising that they were not identified as playing this role in the township where the survey was conducted. Parents did report high levels of positive parenting and involvement, alongside the use of corporal punishment. It may be that because most township parents reported using these positive strategies, these variables did not discriminate between children who had disorders and those who did not. This high rate of reporting of positive strategies may indeed reflect what parents were doing, or may reflect an element of social desirability in their responses to the questionnaire - that they gave answers they thought would show them in the best light, rather than accurate ones (as suggested by the focus group discussions). In addition, our difficulties with the psychometric properties of the Alabama Parenting Questionnaire may have meant that these variables did not accurately measure these strategies in the township. Future research should seek a measure that is robust for use in this context, seek methods that do not only rely on parent self-report (for instance, observational methods)47, and explore whether these parenting behaviours are protective in South African communities such as this township.
The strong association between slapping and spanking, and both externalising and internalising disorders, is also in line with the literature from around the world.48 Slapping and spanking are widely used in the township as a strategy for disciplining children. While it has been proposed in the literature that in such contexts corporal punishment may have weaker associations with children's behaviour,49 our data suggest otherwise, as has been found in other contexts where it is also widespread, such as Tanzania50 and Colombia.51
Our study reports on cross-sectional data, and as such we cannot infer that corporal punishment causes children's mental health and behavioural symptoms. While that is likely, based on the empirical literature,52 it is also possible that children's behaviour elicits corporal punishment from parents, and that corporal punishment increases as that behaviour becomes more difficult for parents.53 Nonetheless, corporal punishment is not an effective strategy for managing child behaviour, and whether elicited by children's behaviour or not, only increases the risk that the child will develop either externalising or internalising symptoms.54 The findings do suggest that strategies to reduce the use of corporal punishment and increase the use of positive discipline could have a positive impact on child behaviour and mental health.
Our data identifies the stress of parenting as having a significant role to play in children's symptoms, and this is underscored by one-fifth of the parents reporting that they had such dysfunctional interactions with their children that they were at risk of abusing their children. Together with the association between corporal punishment and child behaviour, this suggests that parents in the township who found parenting stressful may well have resorted to corporal punishment rather than more effective child management strategies. It also suggests that parenting programmes that teach effective parenting techniques may be helpful in reducing stress through changing parent behaviour and giving parents a sense of success in their parenting, hence reducing children's symptoms.55
Contextual factors, parenting and children's behaviour
Contextual factors influence whether parents And parenting stressful or not. Since our study found that neither being a single parent nor poverty was associated with children's behaviour, it appears that these did not play a role in this context - possibly because the experiences in the township are quite normative.
That substance misuse was not found to be associated with children's behaviour is most likely because it was under-reported: our focus group data suggests that this is highly likely to be the case. Parental substance misuse is typically associated with poor behaviour in children,56 and future studies of parenting in similar contexts should investigate ways to improve reporting on this important matter.
There is a robust literature pointing to the associations between intimate partner violence and mental health, and parenting and child behaviour.57 Our data show that these relationships also hold in this South African township - and since intimate partner violence appears to have been under-reported in our work, the relationships may be even stronger than we were able to detect in this sample.
Implications
Our study has several limitations: it is cross-sectional, and therefore conclusions about the direction of causality cannot be drawn. It also appears that there was a strong social desirability bias that led to underreporting of contextual factors such as substance misuse and intimate partner violence, which may well undermine parenting and affect children's behaviour. However, it does establish that there is a connection between contexts of parenting, parenting behaviour, and children's mental health and behaviour in this rural South African community, and that rates of children's problems in this community are high.
In terms of parents' mental health and experiences of intimate partner violence, our data implies that intimate partner violence and mental health interventions need to be made more widely available in communities. For instance, clinic visits (for children's or parents' illnesses or for other routine matters such as immunisation) should be used as an opportunity to screen parents for these problems, and refer them for help. Similar approaches have shown positive results for intimate partner violence in the developed world.58 In the mental health domain, recent analyses suggest that it is both possible and affordable to deliver services in rural areas, using a tiered model where mental health professionals supervise community health workers.59
One possible direct implication for parenting might be a ban on corporal punishment in all contexts, including the family, an approach which appears to have been successful in both Sweden60 and Germany.61 However, there are two reasons not to propose this approach for South Africa. Firstly, South Africa has many good violence prevention policies, but at present enforcement is wholly inadequate.62 While the Swedish ban on corporal punishment carries no criminal sanctions63 and was explicitly intended to change the norm around parenting in Sweden rather than to punish parents who hit their children, it is an open question as to whether such sanction-free legislation would have a similar effect in South Africa. Secondly, deeper examination of the context in which the ban was introduced in Sweden reveals that it was the culmination of a 70-year cultural shift towards making children's rights to physical integrity more explicit in Swedish law and central in national life.64 While South Africa has been moving to protect children's rights in policy, for instance, through the Children's Act 2005 (Act No. 38 of 2005), many South Africans appear to hold patriarchal views that objectify children rather than prioritise their nurturance and development.65 A focus on achieving a cultural shift away from corporal punishment and towards the use of positive discipline is likely to have a better chance of success than a legislative ban on the use of corporal punishment.
Indeed, our data suggests an alternative approach: equipping parents with effective skills that reduce the stress of parenting, improve children's behaviour and buffer children against adversity.66 Some parenting programmes have demonstrated effect in these areas,67 and although the data is equivocal about the relationship between parent training and parents' mental health,68 some studies suggest that parent training can have positive effects on parents' mental health. Several such programmes are currently in development in South Africa.69 In addition, the policy around child protection and family intervention seeks to enable an increase in parenting support and training; what is needed now is to ensure that programmes offered to parents work and are based on evidence; and to develop an effective strategy and system for reaching parents that need this support.
Acknowledgements
This project, and hence this publication, was supported by a grant from the Open Society Foundation for South Africa (OSF-SA), for which we are very grateful. We also thank the many fieldworkers who collected our data, and the residents of the township who so willingly answered our many questions.
Notes
1 CL Ward, Youth violence, in PD Donnelly and CL Ward (eds), The Oxford textbook of violence prevention: epidemiology, evidence and policy, Oxford: Oxford University Press, 2015, 27-34; [ Links ] DM Fergusson, Stability and change in externalising behaviours, European Archives of Psychiatry and Clinica Neuroscience, 248, 1998, 4-13. [ Links ]
2 LV Scaramella, RD Conger and RL Simons, Parental protective influences and gender-specific increases in adolescent internalizing and externalizing problems, Journa of Research on Adolescence, 9:2, 1999, 111-41. [ Links ]
3 DM Fergusson, Stability and change in externalizing behaviours, European Archives of Psychiatry and Clinica Neuroscience, 248, 1998, 4-13. [ Links ] TE Moffitt et al, Males on the life-course persistent and adolescence-limited antisocial pathways: follow-up at age 26 years, Development and Psychopathology, 14:1, 2002, 179-207; [ Links ] RC Kessler et al, Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization's World Mental Health Survey Initiative, World Psychiatry, 6, 2007, 168-76; [ Links ] S Nolen-Hoeksema, JS Girgus and MEP Seligman, Predictors and consequences of childhood depressive symptoms: a 5-year longitudinal study, Journal of Abnormal Psychology, 101:3, 1992, 405-22. [ Links ]
4 H Coovadia et al, The health and health system of South Africa: historical roots of current public health challenges, Lancet, 374, 2009, 817-34; [ Links ] A Kraak and K Press, Human resources development review 2008: education, employment and skills in South Africa, Cape Town: Human Sciences Research Council, 2008. [ Links ]
5 In this article use of the term 'parent' refers to primary caregivers notwithstanding their biological relationship to the child, e.g. members of the extended family, foster parents or adoptive parents.
6 PJ Fite, CR Colder and JWE Pelham, A factor analytic approach to distinguish pure and co-occurring dimensions of proactive and reactive aggression, Journal of Clinical Child and Adolescent Psychology, 35:4, 2006, 578-82; [ Links ] PJ Frick and E Viding, Antisocial behavior from a developmental psychopathology perspective, Development and Psychopathology, 21, 2009, 1111-31. [ Links ]
7 A Bandura, Social foundations of thought and action: a social cognitive theory, Englewood Cliffs: Prentice-Hall, 1986. [ Links ]
8 R Loeber and M Stouthamer-Loeber, Family factors as correlates and predictors of juvenile conduct problems and delinquency, Crime & Just, 7, 1986, 29-149. [ Links ]
9 ET Gershoff, Corporal punishment by parents and associated child behaviors and experiences: a meta-analytic and theoretical review, Psychological Bulletin, 128:4, 2002, 539 79; [ Links ] OA Barbarin and LM Richter, Mandela's children: growing up in post-apartheid South Africa, New York: Routledge, 2013. [ Links ]
10 MO Howard and JM Jenson, Causes of youth violence, in MO Howard and JM Jenson (eds), Youth violence: current research and recent practice innovations, Washington DC: National Association of Social Workers, 1999, 19-42. [ Links ]
11 VM Murry et al, African American single mothers and children in context: a review of studies on risk and resilience, Clinical Child and Family Psychology Review, 4:2, 2001, 133-55. [ Links ]
12 GH Elder et al, Inner-city parents under economic pressure: perspectives on the strategies of parenting, Journal of Marriage and Family, 57:3, 1995, 771-84. [ Links ]
13 GJ Duncan, J Brooks-Gunn and PK Klebanov, Economic deprivation and early child development, Child Development, 65:2, 1994, 296-318. [ Links ]
14 RH Bradley et al, The home environments of children in the United States part I: variations by age, ethnicity and poverty status, Child Development, 72:6, 2001, 1844-67. [ Links ]
15 K Hall et al, South African child gauge, Cape Town: Children's Institute, University of Cape Town, 2012. [ Links ]
16 H Coovadia et al, The health and health system of South Africa: historical roots of current public health challenges, Lancet, 374, 2009, 817-34. [ Links ]
17 AA Levendosky and SA Graham-Bermann, Parenting in battered women: the effects of domestic violence on women and their children, Journal of Family Violence, 16:2, 2001, 171-92. [ Links ]
18 M Smith, Parental mental health: disruptions to parenting and outcomes for children, Child and Family Social Work, 9, 2004, 3-11. [ Links ]
19 LM Richter and ARL Dawes, Child abuse in South Africa: rights and wrongs, Child Abuse Review, 17, 2008, 79-93. [ Links ]
20 F Souverein et al, Serious, violent young offenders in South Africa: are they life-course persistent offenders?, Journal of Interpersonal Violence (forthcoming). [ Links ]
21 T Mandisa, Home and family circumstances of young offenders: an examination of social workers' views, British Journal of Community Justice, 5:3, 2007, 63-80; [ Links ] P Burton, L Leoschut and A Bonora, Walking the tightrope: youth resilience to crime in South Africa, Cape Town: Centre for Justice and Crime Prevention, 2009. [ Links ]
22 P Burton, L Leoschut and A Bonora, Walking the tightrope: youth resilience to crime in South Africa, Cape Town: Centre for Justice and Crime Prevention, 2009; [ Links ] BK Barber et al, Parental support, psychological control, and behavioral control: assessing relevance across time, culture, and method, Monographs of the Society for Research in Child Development, 4:282, 2005, 70. [ Links ]
23 OA Barbarin and LM Richter, Mandela's children: growing up in post-apartheid South Africa, New York: Routledge, 2013. [ Links ]
24 K Bradford et al, A multi-national study of interparental conflict, parenting, and adolescent functioning, Marriage and Family Review, 35, 2003, 107-37. [ Links ]
25 CA Essau, S Sasagawa and PJ Frick, Psychometric properties of the Alabama parenting questionnaire, Journal of Child and Family Studies, 15:5, 2006, 595-614. [ Links ]
26 RR Abidin, Parenting stress index: a measure of the parent-child system, in CP Zalaquett and RJ Wood, Evaluating stress: A book of resources, Lanham, MD: Scarecrow Education 1997, 277-291. [ Links ]
27 TM Achenbach and C Edelbrock, Child behavior checklist, Burlington: University of Vermont, 1991, 7. [ Links ]
28 L Rescorla et al, Behavioral and emotional problems reported by parents of children ages 6 to 16 in 31 societies, Journal of Emotional & Behavioral Disorders, 15:3, 2007, 130-42. [ Links ]
29 P Goldberg and VF Hillier, A scaled version of the General Health Questionnaire, Psychological Medicine, 9:1, 1979, 139-45. [ Links ]
30 R Humeniuk et al, Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST), Addiction, 103:6, 2008, 1039-47. [ Links ]
31 R Humeniuk et al, The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) manual for use in primary care, Geneva: World Health Organization (WHO), 2010. [ Links ]
32 MA Straus et al, The revised Conflict Tactics Scales (CTS2) development and preliminary psychometric data, Journal of Family Issues, 17:3, 1996, 283-316. [ Links ]
33 JA McVeigh, SA Norris and T de Wet, The relationship between socio-economic status and physical activity patterns in South African children, Acta Paediactrica, 93, 2004, 982-8; [ Links ] ZA Sheppard et al, Approaches for assessing the role of household socioeconomic status on child anthropometric measures in urban South Africa, American Journal of Human Biology, 21, 2009, 48-54. [ Links ]
34 D Labadarios et al, The National Food Consumption Survey (NFCS): South Africa, 1999, Public Health Nutrition, 8:5, 2005, 533-43. [ Links ]
35 V Braun and V Clarke, Using thematic analysis in psychology, Research in Psychology, 3, 2006, 77-101. [ Links ]
36 L Rescorla et al, Behavioral and emotional problems reported by parents of children ages 6 to 16 in 31 societies, Journal of Emotional & Behavioral Disorders, 15:3, 2007, 130-42. [ Links ]
37 DP Goldberg and VF Hillier, A scaled version of the General Health Questionnaire, Psychological Medicine, 9, 1979, 139-45. [ Links ]
38 S Magura and AB Laudet, Parental substance abuse and child maltreatment: review and implications for intervention, Child and Youth Services Review, 18, 1996, 193-220; [ Links ] P Anderson, Alcohol and violence, in PD Donnelly and CL Ward (eds), The Oxford textbook of violence prevention: epidemiology, evidence and policy, Oxford: Oxford University Press, 2015, 291-6. [ Links ]
39 L Rescorla et al, Behavioral and emotional problems reported by parents of children ages 6 to 16 in 31 societies, Journal of Emotional & Behavioral Disorders, 15:3, 2007, 130-42. [ Links ]
40 Ibid.
41 HR Bird, MS Gould and BM Staghezz, Patterns of diagnostic comorbidity in a community sample of children aged 9 through 16 years, Journal of the American Academy of Child and Adolescent Psychiatry, 32:2, 1993, 361-8. [ Links ]
42 HM Connell, L Irvine, J Rodney, Psychiatric disorder in Queensland primary school children, Australian Paediatric Journal, 18, 1982, 177-80; [ Links ] DR Offord et al, Ontaria Child Health Study II: six-month prevalence of disorder and rates of service utilization, Archives of General Psychiatry, 44:9, 1987, 832-6. [ Links ]
43 Children's Institute, University of Cape Town, Housing and services - urban-rural distribution, 2014, http://www.childrencount.ci.org.za/indicator.php?id=3&indicator=13 (accessed 21 December 2014). [ Links ]
44 Fergusson. Stability and change in externalising behaviours, European Archives of Psychiatry and Clinical Neuroscience, 248, 1998, 4-13. [ Links ]
45 CL Ward, Youth violence, in PD Donnelly PD and CL Ward (eds), The Oxford textbook of violence prevention: epidemiology, evidence and policy, Oxford: Oxford University Press, 2015, 27-34. [ Links ]
46 LV Scaramella, RD Conger and RL Simons, Parental protective influences and gender-specific increases in adolescent internalizing and externalizing problems, Journal of Research on Adolescence, 9:2, 1999, 111-41. [ Links ]
47 F Gardner, Methodological issues in the direct observation of parent-child interaction: do observational findings reflect the natural behavior of participants?, Clinical Child and Family Psychology Review, 3:3, 2000, 185-98. [ Links ]
48 ET Gershoff, Corporal punishment by parents and associated child behaviors and experiences: a meta-analytic and theoretical review, Psychological Bulletin, 128:4, 2002, 539-79. [ Links ]
49 JE Lansford, The special problem of cultural differences in effects of corporal punishment, Law and Contemporary Problems, 73, 2010, 89-106. [ Links ]
50 T Hecker et al, Corporal punishment and children's externalizing problems: a cross-sectional study of Tanzanian primary school aged children, Child Abuse & Neglect, 38:5, 2014, 884-92. [ Links ]
51 MR Gonzalez, A Trujillo and N Pereda, Corporal punishment in rural Colombian families: prevalence, family structure and socio-demographic variables, Child Abuse & Neglect, 38:5, 2014, 909-16. [ Links ]
52 ET Gershoff, Corporal punishment by parents and associated child behaviors and experiences: a meta-analytic and theoretical review, Psychological Bulletin, 128:4, 2002, 539-79. [ Links ]
53 ET Gershoff, Corporal punishment, physical abuse, and the burden of proof: reply to Baumrind, Larzelere, and Cowan (2002), Holden (2002), and Parke (2002), Psychological Bulletin, 128:4, 2002, 602-11. [ Links ]
54 Ibid.
55 J Hutchings et al, Parenting intervention in Sure Start services for children at risk of developing conduct disorder: pragmatic randomised controlled trial, British Medical Journal, 334, 2007, 678-82; [ Links ] J Barlow et al, Individual and group-based parenting programmes for the treatment of physical child abuse and neglect, Cochrane Database of Systematic Reviews, 3, 2006; [ Links ] J Barlow et al, Group-based parent training programmes for improving parental psychosocial health, Cochrane Database of Systematic Reviews, 6, 2012. [ Links ]
56 S Magura and AB Laudet, Parental substance abuse and child maltreatment: review and implications for intervention, Child and Youth Services Review, 18, 1996, 193-220. [ Links ]
57 AA Levendosky and SA Graham-Bermann, Parenting in battered women: the effects of domestic violence on women and their children, Journa of Family Violence, 16:2, 2001, 171-92; [ Links ] M Smith, Parental mental health: disruptions to parenting and outcomes for children, Child and Family Social Work, 9, 2004, 3-11. [ Links ]
58 G Feder and L Sardinha, Preventing intimate partner violence through advocacy and support programmes, in PD Donnelly and CL Ward (eds), The Oxford textbook of violence prevention: epidemiology, evidence and policy, Oxford: Oxford University Press, 2015. [ Links ]
59 I Petersen et al and the Mental Health and Poverty Research Programme Consortium: A task-shifting approach to primary mental health care for adults in South Africa: human resource requirements and costs for rural settings, Health Policy and Planning, 27, 2012, 42-51. [ Links ]
60 JE Durrant, Evaluating the success of Sweden's corporal punishment ban, Child Abuse and Neglect, 23:5, 1999, 435-48. [ Links ]
61 K Bussmann, Evaluating the subtle impact of a ban on corporal punishment of children in Germany, Child Abuse Review, 13, 2004, 292-311. [ Links ]
62 WHO, Globa status report on violence prevention 2014, Geneva: WHO, 2014. [ Links ]
63 JE Durrant and GM Olsen, Parenting and public policy: contextualizing the Swedish corporal punishment ban, Journal of Social Welfare and Family Law, 19:4, 1997, 443-61. [ Links ]
64 Ibid.
65 LM Richter and ARL Dawes, Child abuse in South Africa: rights and wrongs, Child Abuse Review, 17:2, 2008, 79-93. [ Links ]
66 RD Conger and KJ Conger, Resilience in Midwestern families: selected findings from the first decade of a prospective, longitudinal study, Journa of Marriage and Family, 64, 2002, 361-373. [ Links ]
67 J Barlow et al, Individual and group-based parenting programmes for the treatment of physical child abuse and neglect, Cochrane Database of Systematic Reviews, 3, 2006; [ Links ] J Barlow, Preventing child maltreatment and youth violence using parent training and home visiting programmes, in PD Donnelly and CL Ward (eds), The Oxford textbook of violence prevention: epidemiology, evidence and policy, Oxford: Oxford University Press, 2015, 133-40. [ Links ]
68 J Barlow et al, Group-based parent training programmes for improving parental psychosocial health, Cochrane Database of Systematic Reviews, 6, 2012. [ Links ]
69 See, for instance, WHO, Violence and injury prevention, http://www.who.int/violence_injury_prevention/violence/child/plh/en/; The Parent Centre, http://www.theparentcentre.org.za/.


{kind=link}
{kind=link}