










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEducation as Change
On-line version ISSN 1947-9417
Print version ISSN 1682-3206
Educ. as change vol.23 n.1 Pretoria 2019
http://dx.doi.org/10.25159/1947-9417/3757
ARTICLE
Risks and rewards in sexual and gender minority teaching and learning in a South African Health Sciences medical curriculum
Chivaugn GordonI; Veronica MitchellII
IUniversity of Cape Town, South Africa c.gordon@uct.ac.za https://orcid.org/0000-0002-9751-896X
IIUniversity of Cape Town, South Africa veronica.mitchell@uct.ac.za https://orcid.org/0000-0002-3436-5185
ABSTRACT
The wellbeing of sexual and gender minorities (SGM) is undermined by widespread homophobia that extends to health systems, and is exacerbated by medical curricula underrepresenting the health needs of this key population group. In 2012, under the auspices of the Department of Obstetrics and Gynaecology at the University of Cape Town in South Africa, a student-inspired curriculum intervention led to the introduction of interactive participatory workshops centred on the health needs of SGM. This paper describes the experiences of two of the workshop facilitators who embraced the risk of introducing an unchartered topic in a student-centred manner, which frequently led to unpredictable events that were challenging. Here, the authors reflect on their own vulnerabilities, which are considered alongside the value of moving through risk to transform present curricular practices and student attitudes, especially in a country like South Africa where prejudice against SGM patients by healthcare providers is well-documented.
Keywords: homophobia; sexual and gender minority health; LGBTI health; health discrimination; vulnerability; health professions education; medical undergraduate curriculum
Introduction
Studies have highlighted the effects of homophobia on the wellbeing of sexual and gender minorities (SGM) of all ages and ethnicities (Sandfort et al. 2013; Wilton 2000). Homophobia, the irrational fear and hatred of people who are attracted to the same sex, can lead to discrimination against and stigmatisation of SGM people, which in turn can lead to social exclusion (Wilton 2000). South Africa is one of many countries where intolerance of same-sex relationships is prevalent, and this is despite one of the most progressive and liberal constitutions in the world (Sandfort et al. 2013). Healthcare providers are not immune to the sociopolitical and legal environments in which they live and work: culture, curriculum and personal values influence healthcare workers' behaviours (HC3 2016; Kim and Motsei 2002).
Particular health risks to SGMs include a significant burden of mental health issues, HIV and sexually transmitted infections, gender-based violence, substance abuse, chronic diseases such as heart disease and hypertension, as well as the risks associated with hormone treatment and gender reassignment surgery (Muller 2013a; Republic of South Africa 2011; Royal College of General Practitioners 2015; UNAIDS 2016). These risks can lead to higher levels of morbidity and mortality as a result of infections, cancers, and heart disease (Brotman et al. 2002; Rich 2006). In the health system, compared with heterosexual and non-transgender socioeconomically matched peers, SGM individuals are more likely to face barriers accessing healthcare tailored to their needs (AAMC 2014; GLMA 2001). The problem of homophobia impacting on SGMs accessing healthcare is a global one and manifests in a variety of ways, depending on local customs and laws. For example, the criminalisation of homosexuality can make access to healthcare even more difficult (UNAIDS 2016).
This article addresses deep concerns about access to quality care for the SGM population, and looks towards the importance of training future healthcare professionals to better understand and address the health needs of this population. We describe an innovative curricular intervention focusing on the healthcare needs of SGM, and attitudes of medical students towards SGM at the University of Cape Town (UCT), in South Africa, the leading medical school on the African continent (Centre for World University Rankings n.d.). Included is a focus on the educators' reflective insights about the rocky shores of this unchartered territory. In this paper we choose the more inclusive term of SGM for this key population group in preference to LGBTI (lesbian, gay, bisexual, transgender and intersex), unless quoting directly from others.
Matters Relating to the Curriculum
After the fall of apartheid, UCT adopted an "ethical commitment to ... radical transformation of education" (Duncan et al. 2006; Mayers et al. 2006). In the early 2000s, a substantial reworking of the "pre-clinical" curriculum took place. A multiprofessional, student-centred, primary healthcare (PHC), problem-based learning approach was adopted. The curriculum content moved away from a purely biomedical model, in an attempt to create more social awareness and unite all healthcare professionals in working together towards social justice, human rights and patient-centred care (Hartman and Seggie 2001). The curriculum was designed in consultation with many stakeholders and professionals, including those from the social sciences-in particular, education specialists.
However, education is not neutral (Freire 2000). Curricular design emerges from the sociopolitical forces that influence institutional culture. Recent protests in South African higher education institutions highlight the urgent need to relook at institutional culture as well as curricular matters in terms of what is foregrounded and what knowledges are silenced. Silences on certain topics transmit an implicit message to students. In their work on the hidden curriculum, Hafferty and O'Donnell (2014, 237; italics in original) refer to the null curriculum as "that which is conveyed when things are not said or done."
What is not covered in most health professions curricula is SGM-specific health needs, as well as the complexities of different gender identities (Muller 2013b). Most healthcare providers do not know about these issues due to lack of training (Muller 2013a; 2013b; 2015). Research indicates that "providers feel unprepared to give quality care for LGBT patients" (Fallin-Bennett 2015, 550). The complexity and prevailing barriers to including SGM health matters in curricular content is noted by Davy, Amsler, and Duncombe (2015). These include the historical deficit approach and pathologisation of SGM health issues and the variation of educators' willingness to engage in these discussions, pointing out that teachers responsible for under- and postgraduate health sciences courses "may be either unable or unwilling to include LGBT curricula in complex ways in their courses" (Davy, Amsler, and Duncombe 2015, 140). This unwillingness or inability is due to perceived lack of curriculum time and space, what competencies are valued at the institution and by the professional board, and the degree of resistance from students and colleagues to including SGM matters in the curriculum (Davy, Amsler, and Duncombe 2015, 140). More broadly, political agendas also influence curricula in complex ways (Chisholm 2005). While these challenges remain, the need for improved SGM health provision has been explicitly recognised in numerous areas, and consequently, the need to train healthcare providers in this area is filtering through to institutions of higher education (Muller 2013b; Obedin-Maliver et al. 2011).
Matters Relating to the Healthcare Professional
While ignorance about SGM specific health needs on the part of healthcare practitioners resulting from curricular inadequacies is partly the reason for poor experiences of the healthcare system, a bigger challenge is that many SGM patients experience prejudice or frank homophobia at the hands of healthcare providers (HCPs) (Beehler 2001; Eliason and Schope 2001). This can manifest as frank hostility from the healthcare provider, refusal of care and/or being told to access care elsewhere, and verbal abuse such as mocking (Banks 2003; Harcourt 2006). These real or feared judgemental attitudes can alienate SGM people from the healthcare system, and significantly reduce health-seeking behaviour and the uptake of screening programmes (Bateman 2011; Brotman, Ryan, and Jalbert 2002; Cloete, Sanger, and Simbayi 2011; Lane et al. 2008; Muller 2013b; O'Hanlan et al. 1997; Rich 2006; Stevens 2012). Because of these fears, SGMs often do not disclose their sexual orientation to HCPs, potentially leading to suboptimal care; or at times they need to educate their HCP about their gender identity and/or sexual orientation (Wilton 2000).
Given that up to 10 per cent of the general population identify as SGM, and still more do not identify as homosexual but have same-sex sexual experiences (Herbenick et al. 2010), every doctor is likely to encounter patients with SGM health needs in the course of their career.
Moving Forward towards Equitable Healthcare
A critical first step towards achieving improved healthcare for the SGM population is to ensure that gender and sexuality teaching is systematically integrated into curricula for healthcare workers (Muller 2015; Obedin-Maliver et al. 2011). Currently, in the South African health sciences, the dominant pedagogical approach to sexuality is biomedical and developmental, and does not focus on the broader societal context of sexual orientation as a social determinant of health (Bennett and Reddy, 2009). Meyer (2001, 857) emphasises that an understanding of "[health] risks related to social conditions characterised by prejudice, discrimination, and rejection" is equally important to biomedical knowledge.
Several authors have noted the immense potential for strategically designed and integrated teaching about SGM health in HCP training courses, especially with respect to facilitating a critical interrogation of students' attitudes towards this population (AAMC 2007; Bennett and Reddy 2009). The AAMC (2007), amongst others, has recommended that SGM health be routinely integrated into medical school curricula, (AAMC 2007; Bennett and Reddy 2009; Muller 2015). Below we describe the development of our workshops at UCT as an example of moving from passive avoidance to active respondence to SGM health needs.
A Case Study at the University of Cape Town Health Sciences Faculty
A curriculum mapping exercise at UCT in 2012 highlighted the fact that the undergraduate MBChB (medical) and allied health sciences curricula do not adequately address SGM specific health issues, or the impact of homophobia and heteronormativity on access to healthcare. When the topic is taught, it is not systematically integrated throughout the programme (Muller 2013b). For example, only 10 academic educators taught some aspects of SGM health (e.g. HIV in men who have sex with men, HIV and STIs, terms and definitions, disorders of sexual development [e.g. intersex], and gender transitioning) within the MBChB programme, but these were scattered across disciplines and clinical years. There was no SGM health taught in any of the allied health degrees. Chronic diseases, safer sex for SGMs, mental health issues in SGMs as well as stigma, discrimination and social exclusion-crucial predictors of SGM people's health-were not covered in any of the curricula.
In what follows we describe an intervention in the Department of Obstetrics and Gynaecology (Dept O and G) that was initiated as a result of the curriculum mapping project described above. Together with colleagues, we, the authors of this paper, initiated SGM workshops in 2013, acknowledging that "the way to break cycles of implicit bias is to confront them" (Fallin-Bennett 2015, 551 citing the Implicit Bias Review 2014). Our intention was to create a robust pedagogical model with a focus on student-centredness, in the form of a student-led workshop. We chose the Pedagogy of Discomfort as an educational tool and a methodology.
Initially we had three facilitators, each one with a specific role: an academic with years of experience in the field of SGM who helped conceptualise the design by incorporating her content knowledge, and both authors of this paper who worked further with the pedagogical design and facilitated the workshops. The reflections presented in this paper were motivated by our challenges that included facilitating workshops without the content expert at times and as individuals who do not identify as members of the SGM community. Even though we are both experienced facilitators on human rights matters, we felt vulnerable in our relative lack of knowledge. However, the immense value of the workshops as reported by the students inspired us to continue.
Chivaugn is the fifth-year gynaecology course convener, with a passion for social justice and advocacy in her role as a medical doctor and educator. She contributed her expertise in mental health and health professions education, explaining:
I joined the Curriculum Review Task Team in 2012, when I started my teaching job. We had a serendipitous opening in our 5th year Gynaecology course seminar schedule, and thus grabbed the opportunity to workshop this underrepresented topic into our course curriculum. Our department is renowned to be innovative and holistic, and this seemed the perfect fit.
Veronica, with a background in physiotherapy, developed an interest in human rights education when she recognised the disparities between the reality of healthcare practice in South Africa and the very progressive and comprehensive policies and programmes supported by the South African Constitution. She explains:
My few years facilitating human rights workshops with students at several levels in the medical curriculum inspired me to continue treading into the mushy waters of human rights issues in healthcare. My current doctoral research and teaching centres around seeking opportunities and ways to develop socially just pedagogies in higher education.
Delving into Diversity Workshops
In 2013 we began a two-part series for each block of approximately 40 fifth-year medical students. At the introductory session, students were introduced to the topic of SGM health. Included in the programme was a questionnaire challenging heteronormative beliefs (Rochlin 1972) in which students confront their habits of belief.
From a pedagogical perspective, we asked students to write on a "Post-it note" a burning question they had about SGM health with the assumption that these questions would be answered and addressed in further discussions. In the introduction students are exposed to complex situations that illustrate how labelling and boxing people into categories during medical history-taking can be inappropriate in terms of sexual orientation and identity.
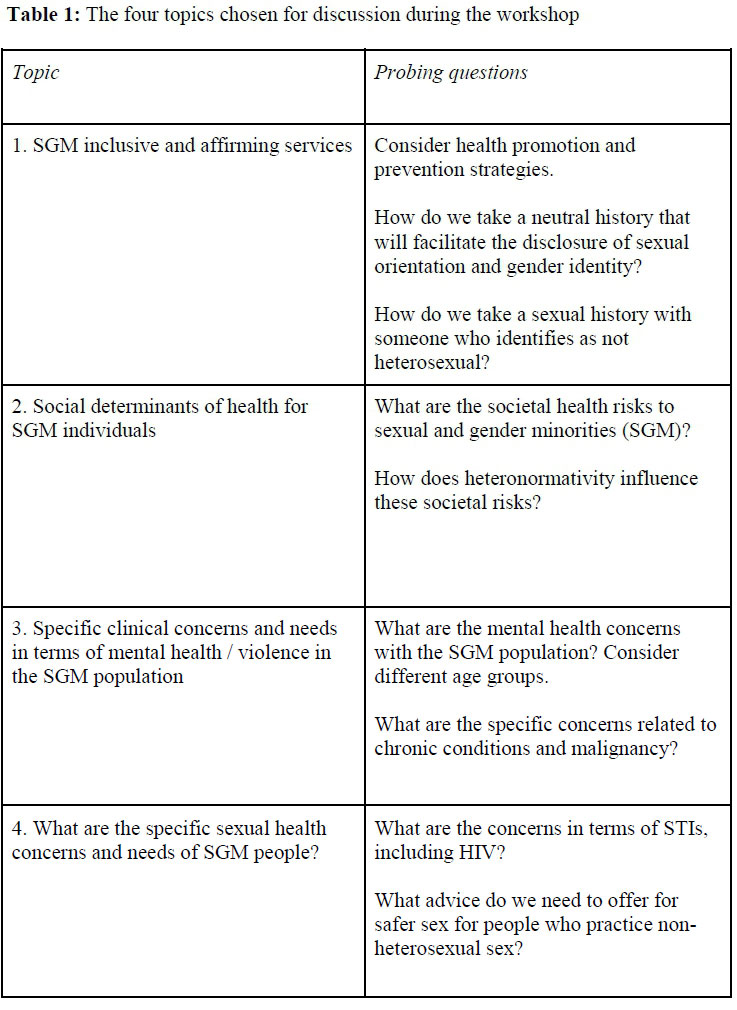
Four topics for discussion were specifically chosen due to their apparent absence in the curriculum. Probing questions on each topic were given to the small student groups (approximately 10 students) to go home and research and then present their learning to their peers at a participatory workshop five weeks later. The topics chosen (after much collaborative deliberation) included the following:
To add a touch of fun and entertainment to serious learning, students were encouraged to be creative in their presentations and to experiment with any technique in presenting their information and findings. In the weeks between the introduction and 15-minute presentation, they were expected to read up about SGM health and the associated information. In the two-hour workshop sessions, each presentation was followed by five minutes of class/expert discussion.
Different guests were invited from local health facilities who specialise in SGM health, such as the Ivan Toms Men's Health Centre, members of local non-governmental organisations such as Gender Dynamix and the Triangle Project, as well as others connected with the needs of SGMs who have been involved in making a difference and bringing about change. Recently, a senior student who openly self-identifies as being gay volunteered to help facilitate the workshops, willingly sharing his personal experiences of discrimination and his expertise in the topic of SGM health.
Below we reflect on aspects of these interventions that could be of interest to others wishing to replicate our workshops, then we move on to student feedback. First, we share our insights from pursuing these pedagogical interventions, second, the moments that glowed for us (MacLure 2010), reflecting the excitement experienced during these workshops that for some students became life-changing events, and third, the many and continued challenges that we have experienced.
Insights: Reflecting on Our Pedagogical Practices
Our student population in South Africa is very diverse in terms of demographics and belief systems. As white, privileged heterosexual women we recognised our limitations. We were conscious of not belonging to the SGM community, which may have compromised our understanding of the intersectionalities relevant to this topic. We did not feel discomforted by our own gender, however, for some students this may have impacted on the way our facilitation efforts were received. Below we consider four poignant questions that surfaced for us.
Why Did We Take on This Difficult Task That Others Avoid?
Despite SGM matters not being strictly under the banner of obstetrics and gynaecology, we decided to include this topic in our curriculum because we are both risk-takers, willing to break rules and not conform to the usual. What initially brought us together as co-facilitators was a creative excitement about the potential to fill a vast curricular gap. In terms of working with difficult topics which can lead to dissent and discomfort, Zembylas and McGlynn (2012, 57) claim that "not all teachers can do this kind of work." The SGM workshops have opened up a curricular space for a hidden topic area. They also opened us up to different pedagogical challenges where we encouraged and accepted discomfort and co-learning for both us and the students.
We came to realise how our past troubling experiences actually equipped us for this work. Chivaugn faced bullying at school as she was taller than her peers, had wild curly hair, was an "academic nerd" and was singularly incapable of any sporting activity. She has learnt to embrace her differentness as a strength in being and becoming a good teacher. Chivaugn's research interests follow a thread of social responsibility towards vulnerable populations, which naturally include SGM. In her teaching of undergraduate medical students in classrooms and clinics she emphasises empathic holistic care and frequently chooses to push students beyond their comfort zones as a way to foster transformative learning (Boler and Zembylas 2003).
Veronica lives with a visual impairment. Despite the consequent limitations, this situation also acts as a resource to find alternative and different ways for doing and being. In experimenting with different pedagogical tools as a PhD candidate in education she has found value in "staying with the trouble" using theoretical concepts that recognise the entangled relationships that are continually occurring in our becoming-with others (Haraway 2016).
Both our experiences of the workshop, and more importantly the uncovering of those vulnerabilities in front of the students provided a powerful alternative teaching approach that we felt could prepare students better for their own possible vulnerabilities in their future practice. Through our immersion with the students, we shared the experiences and the vulnerabilities with them.
Our Immersion in Discomfort
Our experiences in the workshops varied widely. We chose to avoid an overly pre-determined, structured curricular input with clear learning outcomes, rather enabling newness to emerge through students leading their own learning. This brought much uncertainty to us, which led to an additional level of vulnerability that is not reached in traditional teaching practices such as lectures and teacher-led initiatives.
Chivaugn reflected that:
Facilitating these workshops is intense and things can go wrong. As doctors we have the knowledge and authority to solve problems by finding solutions but in these workshops there are many questions that I cannot answer. But that in itself is a vital learning moment. By role-modelling that we understand the limits of our knowledge and experience and that we as "experts" make mistakes, we make vulnerability more acceptable; we acknowledge the value of working together in trusting relationships that make asking for help acceptable as opposed to avoidable.
When I was a student, it was not acceptable to not know, and I was left with the impression that Medicine must be a discipline of perfection; that no patients may ever die; that mistakes are an embarrassment. This sentiment was carried into my first years as a teacher. As a novice teacher, my initial responses to being asked a question to which I did not know the answer were of discomfort and/or defensiveness.
It took years in the profession before I was shown that it was acceptable to be vulnerable, and to not know. Hopefully I am successfully showing my students how to be and become vulnerable without harming themselves or others.
Bullough (2005, 23-4) describes the benefits that teachers may incur if they embrace their vulnerability, as expressed in the two quotes below.
[Vulnerability] is a mood born of a demanding and uncertain environment where teachers confront ever present and constant reminders of their limitations as reflected in the eyes of a disappointed pupil or made public by a grumbling and dissatisfied parent. To be vulnerable is to be capable of being hurt.
Vulnerability is not merely a part of teaching that must be managed, it is also a powerful motivating force behind human development, a determining factor of competence that is dependent upon the existence of the genuine possibility of failing, and, when connected to unpredictability in relationships, a source of much that is delightful and inspiring about teaching. Thus, the burden of vulnerability, when too heavy, may crush one's hopes and dreams or, in some forms, it may spur a reshaping then a realization of them.
Veronica's vulnerability in the intervention was also felt despite her years of experience as a human rights facilitator. She was constantly aware and concerned about the sensitivities that can be provoked in these SGM workshops, as reflected in her observation below:
We have such a range of student needs and positions. I am always conscious of my own vulnerability in possibly unintentionally causing dissent. This sense of holding back was evident from a student's feedback comment that I received. The student asked for more provocative discussions that could address the deep and relevant issues for some students who experience clashes between their religious beliefs and normalised behaviours in the SGM community.
Our vulnerability extended to the classroom presentations as each student session was a surprise for us. While most students went to an enormous amount of effort in their presentations (discussed below), some did not-for example, choosing rather to "hide behind" existing resources found online (such as videos), which left us feeling that they had engaged only very superficially. This revealed a limitation in the workshop design and instruction, which resulted in a change in the workshop structure at a later stage.
Judgemental attitudes were present and played out in a number of ways in student reflections; for example, some students felt the workshops were unnecessary and should not be compulsory; others wrote in their reflections that they would refuse to see members of the SGM population in clinical practice. Most harmfully, there were times when students voiced hurtful, discriminatory and/or judgemental comments or laughed about the SGM population during the workshops. As facilitators, we perceived our role as requiring us to challenge any misperceptions in a firm, compassionate, educational way that would protect any SGM students, but also not tear the "offending" student down, and thus losing a valuable teaching moment. Managing these conflicts was extremely difficult. At times, these incidents were under our radar and only emerged in the evaluations. Two students responded to the question "what did you not appreciate about the workshop?" in the following ways:
Laughter at things that shouldn't have be laughed at e.g. atrocious stories [with respect to the incidence of] gay violence.
Some students were still very negative and insensitive.
Some gay students expressed frustration at what they perceived to be the narrow-mindedness of their peers, or felt the workshop was too superficial. Students also despaired at some of their colleagues' misconceptions. One group of students interviewed other individual students on the health sciences campus about their knowledge of the SGM community, and one student in the group reflected that:
[I learned] how many misconceptions are out there AND still (emphasis student's own) taken up by those in medical school ... The misconceptions and myths seem so far from truth. I couldn't believe others with my level of education would hold onto them. It shocked me.
How Did We Become Conscious of Our Unconsciousness?
On several occasions we became aware of our own assumptions that altered the paths of our own learning. Below we discuss our preconceived ideas that brought about change, then share the impact of guest interventions and how we came to understand the importance of language in these interventions.
Our assumptions for the intervention were challenged in many ways. For instance, we believed that a safe and respectful space was created for all students by the intervention. As time went on, we realised that not all students found the workshop to be a safe space. Consequently, we had to rethink our approach, and came to better understand the sentiment of Zembylas and McGlynn (2012, 56) who claim that "an ethic of empathy and caring is necessary to provide a safe place for students to examine, challenge, and change their cherished beliefs and assumptions."
We had to become more sensitive to the fact that there were extreme positions in our student group, from those who identified with the SGM community to others who did not even know what the LGBTI acronym stood for, or were frankly opposed to SGMs. We became more pro-active in setting ground rules and challenging any homophobic comments that could arise. The latter could prove difficult and stretched our skills as facilitators. Having guests to address homophobic comments and preconceived ideas proved enormously helpful. While for some students open conversations with guests about sexual health and sexual acts were welcome, for others it was clearly uncomfortable or embarrassing, especially in the context of religious beliefs, and it was difficult to try and contain these widely varied responses. The following comments are responses to the question "what did you not appreciate about the workshop?"
The discrimination against us who don't think homosexual (sic) is normal.
Forcing us to think it's normal.
Some of the pictures of lesbian and gay people kissing.
The guests invited to each student session all identified with the SGM community or worked closely with this key population. A large variety of guests attended over the years and naturally responded in different ways. Their input and presence were always appreciated by the students, however what was particularly needed for students' engaged learning was to hear personal narratives. For some guests, understandably, it was more comfortable to focus on facts that reflected discriminatory practices than to share their personal lived experiences. In these cases, the majority of students fed back that they would have preferred some lived examples. Similarly, we found very few students willing to express their own vulnerabilities, but when they did, the impact was enormously powerful. The one activist student who came forward in 2017, and joined us as part of our teaching team, initially expressed his disgust at the deficiency of the undergraduate curriculum, saying "our medical education severely lets down queer individuals."
Related to this sense of undermining others was the issue of language used to discuss SGM health matters, which can be contentious. One of many student comments was "I realised how easily one can let slip a word or phrase that may come across as offensive to LGBTI patients without intending to offend." Chivaugn reflected that:
One of the biggest challenges I've faced is the unconscious use of what is potentially harmful language-e.g. "they" and "normal." One group of students wrote and enacted a play about a gay man, chronicling his different life stages and all the prejudice he faced at every phase. The students chose not to cast a stereotypical "queen" as the gay character, which several other groups had done. I congratulated them afterwards for doing this, but put my foot in my mouth-I said "I like that you decided not to cast him as effeminate. You chose to depict him as just a normal guy" My intention with the comment was to emphasise that stereotypes are not always true; that to decide that someone is gay just by appearances is incorrect. The student himself (who was heterosexual) said to me laughingly, "What's normal?" I was so embarrassed, but I turned it into a teaching moment-showing students how easily we can lapse into heteronormative language and assumptions.
What Moments Glowed for Us?
Learning was clearly enhanced by students' own performances and peer teaching. In medicine there are few opportunities for students to show off their creativity. We were astounded by the imaginative and effective use of different media used by student groups. Students wrote poems, songs, created videos that included themselves and others, role-played different scenarios, and brought their musical instruments to play in the class performance. Interviewing their peers on their views on SGM matters and members of the SGM community indicated a willingness and desire to move beyond the usual classroom practices. One group wrote a comprehensive framework for how to take a history from an SGM patient, and then videoed an enactment of this. These extra efforts just gleamed with advocacy. We felt immensely rewarded that our work was making a difference to students' learning and hopefully their future practice as caring doctors. There was also evidence in the workshop evaluations of transformative learning moments and the development of new awareness for the need to advocate for SGM. Examples of students' response to the question "what did you learn from your preparation for, and presence in this workshop?" are shown below.
I was shocked at how homophobic I was, and I still feel strongly about my views but now I understand that everyone has the right to live the way they want to, I have to relate to that.
I now know how important it is to respect others' way of living and that my opinions can affect how I treat my patients.
To be an activist against [discrimination] and often help in NGOs [non-governmental organisations] and [with] physical care from a Dr.
Students' Reflections
Feedback on the workshop was overwhelmingly positive. The feedback was given first, through the workshop evaluations, which were part of our data collection method, and second, through the post-hoc workshop reflection, which was designed as an educational tool rather than a data collection method. These reflections yielded very valuable information. Common themes emerging from these reflections will be presented below with respect to learning, process, criticisms and suggestions.
Most students' comments showed some evidence of an improvement in their understanding about the healthcare needs of the SGM community. Even more importantly, there was the move towards transforming previously held assumptions and beliefs about their roles as doctors and responsible citizens. Students commented on how their preconceived ideas, stereotypes and judgments had been challenged and had subsequently shifted. However, a small but significant number showed limited evidence of any shift in understanding, attitudes or prejudices about the SGM population. Their comments appeared to be based on religion, and the teaching that homosexuality is wrong. Some students were extreme in what they said in their reflections; it happened in most workshops. This was troubling for us. Were we sending out graduate students who would refuse to care for members of the SGM population? A consolation for us was that the workshop possibly provided these students with a sensitisation that could stay with them and have a potential for change.
In terms of the impact of the workshop on learning, most students said that they had learned an enormous amount about the healthcare needs of SGM and about their own thoughts and actions that they had previously not had to scrutinise. Some students also developed a new appreciation for the courage of SGM individuals who have to face such societal stigma and hardship.
In the process of preparing and presenting, some students were shocked at the ignorance and disinterest of some of their colleagues. Others felt that we were impinging on private matters that ought not be discussed. Differing religious beliefs impacted on group dynamics, as illustrated by a student saying "[m]y group member summarising our presentation with a religious sentence-that was her personal view and she should have expressed it later, not in our presentation."
Criticisms towards the intervention included time issues. Students cope with an overloaded schedule and some felt that too much time was devoted to this topic. We also had many students challenging the fact that we were creating a space to focus just on this group of people. Was this unnecessarily boxing an already marginalised key population group? However, with further discussion, most students came to appreciate the need to highlight SGM health needs specifically. Some students expressed their wish for the workshops to be taught by experts and not peer-led. There was a sense that the student body were not adequately knowledgeable to inform their colleagues. A few students felt that the workshops were too basic and assumed ignorance about SGM matters in all students.
The strongest suggestions were to introduce this topic in earlier years, integrate SGM health matters into other disciplinary spaces and as previously stated, to include personal narratives.
How Far Do We Go in Our Attempts to Promote Transformative Learning?
In the classroom, when facilitating sensitive topics, we grapple with the levels and degrees of engagement that are appropriate with a diverse group of students. While discomfort is a strategy to work with in social justice, the affective sensitivities are not measurable or evident unless there is an outburst such as a defensive reaction. Knowing how far to push students along their gradient of discomfort in the name of transformative learning was difficult, and we did not always succeed. Each workshop was different. We moved with the flow of conversations realising that we could not anticipate or place pressure on the depth of discussion. We learned that the most important factors that enhanced our ability to facilitate transformative learning in the moment were to be fully present in the space, and to be attentive to subtle cues such as body language, which betrayed group dynamics and individual students' responses.
The curriculum on SGM healthcare needs was radically changed by our workshops. Since 2018, students have had a chapter on SGM in their course notes, which is examinable. In other words, we are communicating the value of this area by creating a space in the course, and giving students content that is assessed. Ensuring that course content is assessed is crucial in communicating the importance of a topic to students (Tabish 2008).
Limitations of the Intervention
Because workshops were student-directed, the topics covered differed in scope and quality, and some students were unsettled by the lack of structure with specific learning outcomes and expressed a desire for a more traditional approach to which they are accustomed. Furthermore, a longitudinal study would be required to determine whether this one-off intervention does in fact contribute to improved healthcare delivery for the SGM population. We acknowledge that there is a minority of students who are unmoved by the intervention, which remains a deep concern for us in terms of their future interactions with patients.
Conclusion
There is a distinct gap in the South African medical undergraduate curriculum in terms of teaching towards SGM healthcare needs. This is also a global issue. Even resources for teaching on this marginalised group have been limited, with a slow trickle now emerging (AAMC 2007; 2014; Ard and Makadon n.d.; Davy, Amsler, and Duncombe 2015).
However, inclusion of content related to the health of SGM is not enough. In this paper we point out the complexity of teaching around sensitive SGM issues in a meaningful way. We describe an innovative intervention at UCT. Our reflections include the motivating factors, challenges and inspirations gained from facilitating these workshops over five years. Most striking is the levels of vulnerability that we faced as educators willing to step into a curricular gap and keen to be part of a process of changing and decolonising past curricular practices.
Acknowledgements
We acknowledge the curriculum map on SGM teaching in the undergraduate medical curriculum conducted by our colleague Dr Alexandra Muller. We further acknowledge her expertise and contributions to the workshop's design, and for all the insightful co-facilitation she offered when she was available. We are grateful for the willingness of guests and members of the SGM community who volunteered their time to be with us and share their insights-they have been the true backbone of the intervention. We further wish to thank Dr David Backwell, the then student who volunteered to co-facilitate the workshops, drawing on personal and professional experiences.
Veronica wishes to acknowledge the input gained from interactions with Professors Michalinos Zembylas and Vivienne Bozalek and other colleagues in the National Research Foundation collaborative project on Reconceptualising Socially Just Pedagogies (Grant No: 105851).
References
AAMC (Association of American Medical Colleges). 2007. "Joint AAMC-GSA and AAMC-OSR Recommendations Regarding Institutional Programs and Educational Activities to Address the Needs of Gay, Lesbian, Bisexual and Transgender (GLBT) Students and Patients." Washington, DC: Association of American Medical Colleges. Accessed February 19, 2019. https://myhs.ucdmc.ucdavis.edu/documents/41620/0/Recommendations+Regarding+GLBT+Students+and+Patients.pdf/3e41ba7f-b71b-4983-879b-d166da744829. [ Links ]
AAMC (Association of American Medical Colleges). 2014. Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals Who Are LGBT, Gender Nonconforming, or Born with DSD: A Resource for Medical Educators. Washington, DC: Association of American Medical Colleges. Accessed February 19, 2019. https://members.aamc.org/eweb/upload/Executive%20LGBT%20FINAL.pdf. [ Links ]
Ard, K. L., and H. J. Makadon. n.d. "Improving the Health Care of Lesbian, Gay, Bisexual and Transgender People: Understanding and Eliminating Health Disparities." Boston, MA: The Fenway Institute. Accessed February 18, 2019. https://www.lgbthealtheducation.org/wp-content/uploads/Improving-the-Health-of-LGBT-People.pdf. [ Links ]
Banks, C. 2003. "The Cost of Homophobia: Literature Review on the Human Impact of Homophobia in Canada." Saskatoon: Gay and Lesbian Health Services. Accessed February 18, 2019. https://cuisr.usask.ca/documents/publications/2000-2004/The%20Cost%20of%20Homophobia%20Literature%20Review%20on%20the%20Human%20Impact%20of%20Homophobia%20On%20Canada.pdf.
Bateman, C. 2011. "Transgender Patients Sidelined by Attitudes and Labelling." The South African Medical Journal 101 (2): 91-3. Accessed February 19, 2019. http://www.samj.org.za/index.php/samj/article/view/4735. [ Links ]
Beehler, G. B. 2001. "Confronting the Culture of Medicine: Gay Men's Experiences with Primary Care Physicians." Journal of the Gay and Lesbian Medical Association 5 (4): 135-41. Accessed February 19, 2019. https://doi.org/10.1023/A:1014210027301. [ Links ]
Bennett, J., and V. Reddy. 2009. "Researching the Pedagogies of Sexualities in South African Higher Education." International Journal of Sexual Health 21 (4): 239-52. https://doi.org/10.1080/19317610903307712. [ Links ]
Boler, M., and M. Zembylas. 2003. "Discomforting Truths: The Emotional Terrain of Understanding Difference." In Pedagogies of Difference: Rethinking Education for Social Change, edited by P. Trifonas, 110-36. New York: Routledge Falmer. [ Links ]
Brotman, S., B. Ryan, Y. Jalbert, and B. Rowe. 2002. "The Impact of Coming Out on Health and Health Care Access: The Experiences of Gay, Lesbian, Bisexual and Two-Spirited People." Journal of Health and Social Policy 15 (1): 1-29. https://www.ncbi.nlm.nih.gov/pubmed/12212930. [ Links ]
Bullough, V. 2005. "Teacher Vulnerability and Teachability: A Case Study of a Mentor and Two Interns." Teacher Education Quarterly Spring 23-39. Accessed February 20, 2019. https://files.eric.ed.gov/fulltext/EJ795314.pdf.
CWUR (Center for World University Rankings). n.d. "CWUR World University Rankings 2018-2019." Accessed February 19, 2019. https://cwur.org/2018-19.php.
Chisholm, L. 2005. "The Politics of Curriculum Review and Revision in South Africa in Regional Context." Compare: A Journal of Comparative and International Education 35 (1): 79-100. https://doi.org/10.1080/03057920500033563. [ Links ]
Cloete, A., N. Sanger, and L. C. Simbayi. 2011. "Are HIV Positive Women Who Have Sex with Women (WSW) an Unrecognized and Neglected HIV Risk Group in South Africa?" Journal of AIDS and HIV Research 3 (1): 1-5. Accessed February 19, 2019. http://www.academicjournals.org/article/article1379500655_Cloete%20et%20al.pdf. [ Links ]
Davy, Z., S. Amsler, and K. Duncombe. 2015. "Facilitating LGBT Medical, Health and Social Care Content in Higher Education Teaching." Qualitative Research in Education 4 (2): 134-62. Accessed February 19, 2019. https://doi.org/10.17583/qre.2015.1210. [ Links ]
Duncan, M., M. Alperstein, P. Mayers, L. Olckers, and T. Gibbs. 2006. "Not Just Another Multi-Professional Course! Part 1: Rationale for a Transformative Curriculum." Medical Teacher 28 (1): 59-63. https://doi.org/10.1080/01421590500312888. [ Links ]
Eliason, M. J., and R. Schope. 2001. "Does 'Don't Ask Don't Tell' Apply to Health Care? Lesbian, Gay, and Bisexual People's Disclosure to Health Care Providers." Journal of the Gay and Lesbian Medical Association 5 (4): 125-34. https://doi.org/10.1023/A:1014257910462. [ Links ]
Fallin-Bennett, K. 2015. "Implicit Bias against Sexual Minorities in Medicine: Cycles of Professional Influence and the Role of the Hidden Curriculum." Academic Medicine 90 (5): 549-52. https://doi.org/10.1097/ACM.0000000000000662. [ Links ]
Freire, P. 2000. Pedagogy of the Oppressed. New York, NY: Continuum. [ Links ]
GLMA (Gay and Lesbian Medical Association). 2001. Healthy People 2010. Companion Document for Lesbian, Gay, Bisexual, and Transgender (LGBT) Health. San Francisco, CA: Gay and Lesbian Medical Association. Accessed June 29, 2011. http://www.nalgap.org/PDF/Resources/HP2010CDLGBTHealth.pdf. [ Links ]
Hafferty, F. W., and J. F. O'Donnell, eds. 2014. The Hidden Curriculum in Health Professional Education. Hanover, NH: Dartmouth College Press. [ Links ]
Haraway, D. 2016. Staying with the Trouble. Making Kin in the Chthulucene. Durham, NC: Duke University Press. [ Links ]
Harcourt, J. 2006. "Current Issues in Lesbian, Gay, Bisexual, and Transgender (LGBT) Health." Journal of Homosexuality 51 (1): 1-11. https://doi.org/10.1300/J082v51n01_01. [ Links ]
HC3 (The Health Communication Capacity Collaborative). 2016. Factors Impacting the Effectiveness of Health Care Worker Behavior Change: A Literature Review. Baltimore: Johns Hopkins Center for Communication Programs. Accessed February 19, 2019. https://healthcommcapacity.org/wp-content/uploads/2016/05/HCW-Barriers-and-Facilitators-Lit-Review_May2016.pdf. [ Links ]
Herbenick, D., M. Reece, V. Schick, S. A. Sanders, B. Dodge, and J. D. Fortenberry. 2010. "Sexual Behavior in the United States: Results from a National Probability Sample of Men and Women Ages 14-94." The Journal of Sexual Medicine 7 (5): 255-65. https://doi.org/10.1111/j.1743-6109.2010.02012.x. [ Links ]
Hartman, N., and J. Seggie. 2001. "New MBChB Curriculum Goal." Cape Town: University of Cape Town, Faculty of Health Sciences. [ Links ]
Lane, T., T. Mogale, H. Struthers, J. McIntyre, and S. M. Kegeles. 2008. "'They See You as a Different Thing': The Experiences of Men Who Have Sex with Men with Healthcare Workers in South African Township Communities." Sexually Transmitted Infections 84: 430-33. https://doi.org/10.1136/sti.2008.031567. [ Links ]
Kim J., and M. Motsei. 2002. "'Women Enjoy Punishment': Attitudes and Experiences of Gender-Based Violence among PHC Nurses in Rural South Africa." Social Science and Medicine 54 (8): 1243-254. https://doi.org/10.1016/S0277-9536(01)00093-4. [ Links ]
Mayers, P., M. Alperstein, M. Duncan, L. Olckers, and T. Gibbs. 2006. "Not Just Another Multi-Professional Course! Part 2: Nuts and Bolts of Designing a Transformed Curriculum for Multi-Professional Learning." Medical Teacher 28 (2): 152-57. https://doi.org/10.1080/01421590600603137. [ Links ]
MacLure, M. 2010. "The Offence of Theory." Journal of Education Policy 25 (2): 277-86. https://doi.org/10.1080/02680930903462316. [ Links ]
Meyer, I. H. 2001. "Why Lesbian, Gay, Bisexual, and Transgender Health?" American Journal of Public Health 91 (6): 856-9. Accessed February 19, 2019. https://www.ncbi.nlm.nih.gov/pubmed/11392921. [ Links ]
Muller, A. 2013 a. Sexual and Reproductive Health for Transgender and Gender Non-Conforming People: Guidelines for Healthcare Workers in Primary Care. Cape Town: Gender Dynamix. [ Links ]
Muller, A. 2013b. "Teaching Lesbian, Gay, Bisexual and Transgender Health in a South African Health Sciences Faculty: Addressing the Gap." BMC Medical Education 13: a174. https://doi.org/10.1186/1472-6920-13-174. [ Links ]
Muller, A. 2015. "Strategies to Include Sexual Orientation and Gender Identity in Health Professions Education." African Journal of Health Professions Education 7 (1): 4-7. https://doi.org/10.7196/AJHPE.359. [ Links ]
Obedin-Maliver, J., E. S. Goldsmith, L. Stewart, W. White, E. Tran, S. Brenman, M. Wells, D. M. Fetterman, G. Garcia, and M. R. Lunn. 2011. "Lesbian, Gay, Bisexual, and Transgender-Related Content in Undergraduate Medical Education." JAMA 306 (9): 9717. https://doi.org/10.1001/jama.2011.1255. [ Links ]
O'Hanlan, K. A., R. P. Cabaj, B. Schatz, J. Lock, and P. Nemro. 1997. "A Review of the Medical Consequences of Homophobia with Suggestions for Resolution." Journal of the Gay and Lesbian Medical Association 1 (1): 25-39. https://doi.org/10.1023/B:JOLA.0000007009.83600.ae. [ Links ]
Republic of South Africa. 2011. National Strategic Plan on HIV, STI's and TB, 2012-2016. Pretoria: Department of Health. Accessed February 19, 2019. http://www.hst.org.za/publications/NonHST%20Publications/hiv-nsp.pdf [ Links ]
Rich, E. 2006. Overall Research Findings on Levels of Empowerment among LGBT People in Western Cape, South Africa. Johannesburg: Joint Working Group. Triangle Project and the UNISA Centre for Applied Psychology. Accessed February 19, 2019. https://thetriangleprojectsite.files.wordpress.com/2014/02/levels-of-empowerment-among-lgbt-people-in-the-western-cape-south-africa.pdf. [ Links ]
Rochlin, M. 1972. "The Heterosexual Questionnaire." Accessed December 14, 2017. https://www.uwgb.edu/pride-center/files/pdfs/Heterosexual_Questionnaire.pdf.
Royal College of General Practitioners. 2015. "Guidelines for the Care of Lesbian, Gay and Bisexual Patients in Primary Care." Accessed February 19, 2019. http://www.rcgp.org.uk/policy/rcgp-policy-areas/lgbt.aspx.
Sandfort, T. G. M., L. R. M. Baumann, Z. Matebeni, V. Reddy, and I. Southey-Swartz. 2013. "Forced Sexual Experiences as Risk Factor for Self-Reported HIV Infection among Southern African Lesbian and Bisexual Women." PLoS ONE 8 (1): e53552. https://doi.org/10.1371/journal.pone.0053552. [ Links ]
Stevens, M. 2012. Transgender Access to Sexual Health Services in South Africa: Findings from a Key Informant Survey. Cape Town: Gender Dynamix. Accessed February 19, 2019. https://www.genderdynamix.org.za/wp-content/uploads/2012/10/Transgender-access-to-sexual-health-services-in-South-Africa.pdf. [ Links ]
Tabish S. 2008. "Assessment Methods in Medical Education." International Journal of Health Sciences (Qassim) 2 (2): 3-7. [ Links ]
UNAIDS. 2016. Prevention Gap Report. Geneva: UNAIDS. Accessed February 19, 2019. http://www.unaids.org/sites/default/files/media_asset/2016-prevention-gap-report_en.pdf. [ Links ]
Wilton, T. 2000. Sexualities in Health and Social Care: A Textbook. Buckingham: Open University Press. [ Links ]
Zembylas, M. 2008. "The Politics of Shame in Intercultural Education." Education, Citizenship and Social Justice 3 (3): 263-80. https://doi.org/10.1177/1746197908095135. [ Links ]
Zembylas, M., and C. McGlynn. 2012. "Discomforting Pedagogies: Emotional Tensions, Ethical Dilemmas and Transformative Possibilities." British Educational Research Journal 38 (1): 41-59. Accessed February 19, 2019. https://doi.org/10.1080/01411926.2010.523779. [ Links ]


{kind=link}