










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkWater SA
versión On-line ISSN 1816-7950
versión impresa ISSN 0378-4738
Water SA vol.43 no.2 Pretoria abr. 2017
http://dx.doi.org/10.4314/wsa.v43i2.02
Carbapenem-resistant bacteria in a secondary wastewater treatment plant
J HrenovicI, *; M GanjtoII; I Goic-BarisicIII
IUniversity of Zagreb, Faculty of Science, Department of Biology, Zagreb, Croatia
IIZagreb Wastewater - Management and Operation Ltd., Zagreb, Croatia
IIIUniversity Hospital Centre Split, Department of Clinical Microbiology and University of Split, School of Medicine, Split, Croatia
ABSTRACT
Bacterial resistance to carbapenems is an emerging problem of this century. A carbapenem-resistant bacterial population (CRBP) grown at 42°C was monitored in the influent and effluent of a secondary municipal wastewater treatment plant over 10 months. The municipal wastewater consisted of domestic, industrial, hospital and storm wastewaters. Median numbers of CRBP in influent and effluent water were 3.5 and 1.3 log CFU/mL, with its prevalence among total heterotrophic bacteria at 47% and 26%, respectively. Correlation of CRBP with physico-chemical and other bacteriological parameters of wastewater was estimated. Higher numbers of CRBP in influent and effluent were found in cases of nutrient-rich wastewater with higher concentrations of total heterotrophic bacteria and intestinal enterococci. Reduction of CRBP in the wastewater treatment process of 54% was comparable to the reduction of intestinal enterococci. Despite the significant elimination of CRBP in the secondary type of wastewater treatment plant, substantial numbers of CRBP are released through the effluent into the natural receiving waters. Since the CRBP grown at 42°C was not found in natural water samples beyond the vicinity of hospitals, these bacteria may be used as an indicator of hospital wastewaters.
Keywords: environmental bacteria, carbapenem-resistant bacteria, public health, wastewater
INTRODUCTION
Carbapenems are potent β-lactam antibiotics including, at the present time, 7 antibiotics for the treatment of serious infections caused by multi-drug resistant bacteria in hospital settings. They have a broad antimicrobial spectrum action on selected Gram-positive and Gram-negative bacteria by acting on penicillin-binding proteins, thus inhibiting cell wall synthesis (EFSA Panel on Biological Hazards, 2013; Zavascki et al., 2013; Meletis, 2016). Before the 21st century only some clinical isolates of Pseudomonas aeruginosa and Acinetobacter baumannii were carbapenem-resistant, but carbapenem resistance in Gram-negative bacteria has become a global problem of this century (Zavascki et al., 2013; Meletis, 2016). For example, carbapenem-resistance in clinical isolates of A. baumannii in Croatia rapidly increased from 10% in 2008 to 82% in 2014 (CAMS, 2015).
Carbapenem resistance in Gram-negative bacteria, which is almost always associated with resistance to several other classes of antibiotics, can be a result of: production of carbapenemases, expression of efflux pumps, porin loss, and alteration in penicillin-binding proteins. Intrinsic carbapenem resistance implies the inherent low permeability of bacterial membranes, low affinity of penicillin-binding proteins, efflux pumps, and inducible chromosomally-encoded production of carbapenemases. A variety of environmental species of Proteobacteria, Firmicutes and Bacteroidetes pose intrinsic carbapenem resistance (EFSA Panel on Biological Hazards, 2013; Meletis, 2016). Additional acquired resistance implies the acquisition of transferable genetic elements providing for the possibility of successful horizontal spread of resistance genes, even between different genera (Diene and Rolain, 2014). Acquired carbapenemase-encoding genes are frequently harboured on integrons or transposons that are carried by plasmids which are responsible for enzymatic hydrolysis of carbapenems in A. baumannii, P. aeruginosa and Enterobacteriaceae (Opazo et al., 2012; Meletis et al., 2016).
Carbapenem-resistant Gram-negative bacteria are mainly studied as a cause of human infections, while reports regarding the occurrence of viable carbapenem-resistant bacterial populations (CRBP) outside medical institutions are globally scarce. Published papers on CRBP in nature are mostly focused on single bacterial isolates. Viable isolates of CRBP were recovered from hospital sewage both before and after disinfection (Ferreira et al., 2011; Chagas et al., 2011; Zhang et al., 2013; Chandran et al., 2014). From the mixture of domestic and hospital wastewaters two carbapenem-resistant Klebsiella pneumoniae and one Escherichia coli were recovered (Galler et al., 2014). From municipal sewage in Beijing, 37 isolates of CRBP were isolated (Zhang et al., 2013). Carbapenem-resistant isolates of A. baumannii were recovered from raw and secondary treated municipal wastewater (Hrenovic et al., 2016). In the effluent of the secondary municipal wastewater treatment plant, four isolates of CRBP (two members of the family Enterobacteriaceae and two Acinetobacter spp.) were found (Picao et al., 2013). A single isolate of carbapenem-resistant A. baumannii (Girlich et al., 2010) and E. coli (Poirel et al., 2012) were isolated from river water in Europe. Different species of carbapenem-resistant bacteria were isolated from drinking water in New Delhi (Walsh et al. 2011; Tanner et al., 2015).
Designs of the published studies which deal with the presence of CRBP in raw or treated wastewater were not quantitative. Therefore, the numbers of viable CRBP in wastewater remain to be determined, in order to quantify the influence of wastewater on the spread of CRBP in the environment. Moreover, the temperature at which the CRBP from wastewater were cultivated was 35-37°C (Girlich et al., 2010; Ferreira et al., 2011; Walsh et al., 2011; Galler et al., 2014; Tanner et al., 2015) or was not specified at all (Chagas et al., 2011; Poirel et al., 2012; Picao et al., 2013; Zhang et al., 2013). Cultivation at 37°C allows for the isolation of intrinsically carbapenem-resistant bacteria which are autochthonous populations in environmental samples. Therefore, the findings of CRBP grown at 37°C may overestimate its significance in the natural environment as an anthropogenic reservoir of clinically-important CRBP or reservoir of resistance genes which could be spread to autochthonous bacteria. The use of an elevated temperature will allow the enumeration of potential clinically-important CRBP, while eliminating the enumeration of CRBP which are autochthonous in natural waters. The aim of this study was to quantify the numbers of viable CRBP grown at 42°C in municipal wastewater, its removal in the secondary type of wastewater treatment process, and its correlation with physico-chemical and bacteriological parameters of wastewater. Moreover, the natural waters beyond the vicinity of hospitals were screened for the presence of CRBP.
MATERIALS AND METHODS
Wastewater treatment plant and sampling
The study was performed at the largest Croatian wastewater treatment plant, in the capital city of Zagreb. This secondary treatment plant was designed in 2007 for 1 200000 population equivalents. The plant treats municipal wastewater from the combined sewage system of domestic, industrial, hospital and storm wastewaters. Daily water flow is influenced by stormwater runoff. Hospital wastewaters are not pretreated before discharge to the sewage system. Raw wastewater which enters this wastewater treatment plant contains high levels of human-use antimicrobials, which are in general poorly removed in the conventional activated sludge treatment (Senta et al., 2013). The wastewater treatment consisted of primary (mechanical screens, sand and grease removal), and secondary treatment (activated sludge process in aeration basin). After the secondary settling, the effluent is discharged into the natural receiving waters, the Sava River. Sampling was performed from February to December 2014. A 24 h flow-proportional samples was collected from the influent after mechanical screening and from the final effluent after secondary settling. For bacteriological analyses the composite wastewater samples were aseptically taken in sterile 1 L glass bottles. All samples were processed in the laboratory within 2 h of collection.
Characterization of wastewater
The physico-chemical parameters of influent and effluent wastewater were measured according to the Standard Methods for the Examination of Water and Wastewater (APHA et al., 2005). Temperature was measured on-line and average values of composite samples are presented. The numbers of intestinal enterococci, aerobically grown total heterotrophic bacteria, and carbapenem-resistant bacteria were determined as colony forming units (CFU), logarithmically transformed, and expressed as log CFU per 1 mL of water. The samples of wastewater were concentrated on the sterile membrane filters of pore size 0.45 µm in triplicate both before and after dilution in sterile peptone water. The intestinal enterococci were determined according to HRN ISO 7899-2 (2000). Membrane filters were incubated on Slanetz Bartley agar (Biolife) at 37°C/72 h and subsequent confirmation of intestinal enterococci was done on Bile esculin azide agar (Sigma-Aldrich) after incubation at 44°C/4 h. Aerobically grown total heterotrophic bacteria were determined on nutrient agar (Biolife) after incubation at 22°C/72 h (APHA et al., 2005). Carbapenem-resistant bacteria were determined on CHROMagar Acinetobacter supplemented with CR102 (CHROMagar), which allows the growth of carbapenem-resistant isolates after incubation at 42°C/48 h. CHROMagar Acinetobacter with CR102 allows the growth of Gram-negative carbapenem-resistant Acinetobacter sp., Stenotrophomonas sp., Pseudomonas sp., Aeromonas sp. as red colonies, and species of family Enterobacteriaceae as blue colonies. Cultivation of CRBP was performed at 42°C to suppress the growth of environmental autochthonous species with intrinsic resistance to carbapenems such as Stenotrophomonas spp.
Some of the morphologically different colonies of CRBP were re-cultivated (42°C/24 h) on the CHROMagar Acinetobacter supplemented with CR102 and then on nutrient agar. Pure cultures were characterized by routine bacteriological techniques (Gram staining, oxidase and catalase reaction). Further identification was carried out by ATB 32GN and Vitek 2 systems (BioMerieux) and matrix-assisted laser desorption ionization-time of flight mass spectrometry MALDI-TOF MS (Microflex LT, Bruker Daltonics) on cell extracts, according to Sousa et al. (2014). Susceptibility to imipenem and meropenem was determined for 27 Acinetobacter sp. isolates by disc-diffusion tests. The MICs values were confirmed using AST-XN05 and AST-N233 testing card for Vitek2 system, and interpreted according to the European Committee on Antimicrobial Susceptibility Testing criteria (EUCAST, 2014).
Statistical analyses
Statistical analyses were carried out using Statistica software 10 (StatSoft, Inc.). Absolute numbers of bacteria were logarithmically transformed. The comparisons between variables were done using the ordinary Student's t-test for independent variables. The correlation between variables was estimated by Spearman correlation analysis. Statistical decisions were made at a significance level of p < 0.05.
Growth of CRBP at 37 and 42°C
In order to distinguish the growth of CRBP at 37 and 42°C, the spring, stream, lake, and well water samples without the influence of hospital waters were tested. Spring, stream, and well samples were taken at the Medvedinca mountain above the capital of Croatia, Zagreb. The lake sample was taken from the artificial Jarun Lake, which is used for recreation in the southwest part of Zagreb. The effluent from the wastewater treatment plant receiving the leachate from Zagreb's landfill, Jakusevec, where the solid hospital waste is disposed of, was taken as a water sample influenced by hospital waters. The numbers of intestinal enterococci and CRBP were determined as described above, except that CRBP were grown either at 37°C/72 h and 42°C/48 h.
RESULTS
The physico-chemical and bacteriological characteristics of influent and effluent wastewater are shown in Table 1. Measured parameters of both influent and effluent water varied slightly over 10 months of monitoring. High BOD5 to COD ratio and concentrations of nitrogen and phosphorus suggest nutrient-rich biodegradable influent wastewater. A high proportion of intestinal enterococci that are reliable indicators of faecal pollution suggests a high proportion of sanitary water in the influent. The median number of CRBP in influent water was 3.5 log CFU/mL with a prevalence among total heterotrophic bacteria of 47% (Table 1).

The secondary treatment of municipal wastewater resulted in a significant increase in dissolved oxygen and the temperature of treated water. Concentrations of suspended solids, nutrients, and monitored bacteria were significantly reduced after the passage of wastewater through the plant. Concentrations of nutrients in effluent wastewater are in compliance with the national emission standards, which do not imply the monitoring of microorganisms. In the treated effluent, the numbers of CRBP were reduced by 54% and the prevalence of CRBP among total heterotrophic bacteria by 34%. Reduction of CRBP in the secondary treatment of municipal wastewater was not significantly different from the reduction of intestinal enterococci (Table 1). Figure 1 shows the fluctuation of CRBP in influent and effluent water over 10 months of monitoring. Both the numbers of CRBP and their prevalence among total heterotrophic bacteria were significantly lower in effluent than in influent water, except for one case of their prevalence on 7 May. The lowest number of CRBP found in effluent water was 0.5 ± 0.2 log CFU/mL. The CRBP were represented by Gram-negative bacteria (Fig. 1) Pseudomonas sp. (P. aeruginosa, P. putida), Acinetobacter sp. (A. baumannii, A. pittii), and Enterobacteriaceae (K. pneumoniae, E. coli). All 27 examined isolates of Acinetobacter sp. were considered clinically resistant to imipenem and meropenem based on European Committee on Antimicrobial Susceptibility Testing criteria (EUCAST, 2014), with MIC values higher than 8 mg/L.
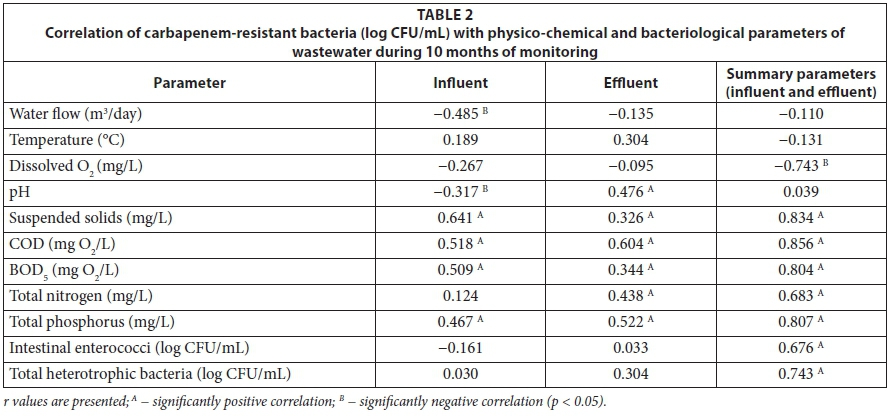
The numbers of CRBP were correlated with physico-chemical and bacteriological parameters of wastewater (Table 2) in order to find out which parameters determine the abundance of CRBP and to check which parameters could be used as surrogates for CRBP. The abundance of CRBP in influent significantly decreased with the increase of inflow due to the dilution of influent with stormwater. Temperature, concentration of dissolved oxygen and pH of water did not influence the abundance of CRBP. Discrepancies in correlation parameters of the influent and effluent water are explained by the huge increase in dissolved oxygen in the treated effluent and minor changes of pH values between influent and effluent water (Table 1). Concentration of suspended solids, COD, BOD5, total nitrogen, and total phosphorus showed a significant positive correlation with the numbers of CRBP, both in influent and effluent water. Absence of the significant correlation of CRBP and total nitrogen in influent water is explained by poor nitrogen removal in the wastewater treatment plant (Table 1). No correlation was found between CRBP with intestinal enterococci or total heterotrophic bacteria, both in influent or effluent water (Table 2). However, when parameters of influent and effluent water were analysed together, significant positive correlation was observed. This is explained by the relatively constant number of intestinal enterococci and total heterotrophic bacteria in influent and effluent water, as well as grouping of their numbers within two matching clusters. Variations of the numbers of monitored bacteria in influent and effluent water when analysed separately were minor, but when summarizing these numbers in influent and effluent water together, variations between these two groups were remarkable.
The CRBP grown either at 37°C or 42°C was not present in 100 mL of spring water where the intestinal enterococci were absent (Table 3). In the well, stream, and lake water samples beyond the vicinity of hospitals where the intestinal enterococci were present, the CRBP grown at 42°C was absent, although CRBP grown at 37°C was present (Table 3). In the leachate influenced by hospital waste, intestinal enterococci as well as CRBP grown either at 37°C or 42°C were present. The numbers of CRBP grown at 37°C were twice as abundant as the CRBP grown at 42°C (Table 3). No CRBP grown at 45°C was found. The CRBP grown at 37°C was represented by Stenotrophomonas maltophillia, Pseudomonas sp. (P. aeruginosa, P. fluorescens), Chryseobacterium sp., and Elizabethkinga meningoseptica, while the CRBP grown at 42°C was represented by Pseudomonas sp., Acinetobacter sp. and the genera of the family Enterobacteriaceae. The presence of CRBP in municipal wastewater receiving hospital wastewaters and in leachate influenced by hospital waste, together with its absence in water beyond the vicinity of hospitals, suggests that CRBP grown at 42°C are associated with hospital wastewaters.

DISCUSSION
Since carbapenems are heavily used in clinics worldwide, including Croatia, the occurrence of carbapenem-resistant isolates is primary connected to the hospital environment. Isolates of CRBP were recovered from hospital wastewaters worldwide (Ferreira et al., 2011; Zhang et al., 2013; Chandran et al., 2014). The prevalence of isolated CRBP in particular ecosystems will vary based on the breakpoint values of target antibiotics applied to determine antimicrobial resistance. There are many in-house-prepared and commercially-available selective media for detection of carbapenem-resistant bacteria from clinical samples (EFSA Panel on Biological Hazards, 2013). Recently, a fluorogenic heterotrophic plate count method was developed for detection of the broad range of carbapenem-resistant bacteria in drinking water (Tanner et al., 2015). In this study, we used a commercially available medium (CHROMagar Acinetobacter supplemented with CR102) intended for isolation of clinically important carbapenem-resistant bacteria, in combination with selective temperature. The applied method surely allowed the isolation of a narrower range of CRBP, but eliminated the enumeration of carbapenem-resistant bacteria which are autochthonous in water.
When summarizing results of this study, it can be concluded that the physico-chemical and routine bacteriological parameters cannot be directly used for the prediction of presence or abundance of CRBP in waters from different sources. The presence and abundance of CRBP in water primarily depends on the proportion of hospital water which influences the particular water ecosystem. The findings of CRBP grown at 42°C surely indicate the influence of hospital waste on the particular water. Therefore, the CRBP grown at 42°C could be used as an indicator of anthropogenic influence of hospital wastewaters on the natural water bodies. The enumeration of viable CRBP cultivated at 42°C seems to be a rapid and cost-effective laboratory method for estimation of the presence of hospital waste and consequently potentially pathogenic bacteria in different types of water.
Physico-chemical parameters could be used for prediction of the abundance of CRBP in the secondary wastewater treatment plants which receive hospital wastewater. In the case of increased concentrations of nutrients (suspended solids, COD, BOD5, total nitrogen, and total phosphorus) as compared to routine values, higher abundance of CRBP could be expected. In the case of increased water inflow due to stormwater runoff, dilution of CRBP is expected. In the raw influent water containing the highest concentrations of bacteria, higher numbers of CRBP are expected as compared to the treated effluent water. Numbers of CRBP in influent showed a significant positive correlation with their numbers in effluent water (r = 0.724). A significant positive correlation of CRBP with intestinal enterococci and total heterotrophic bacteria in the wastewater treatment plant (Table 2) suggests that the concentrations of CRBP through the plant were primarily attributable to the changes in total bacterial abundance rather than to efficiency of its removal. This observation is consistent with the report of a positive correlation of NDM-1 and 16S rRNA genes used as surrogates for multidrug resistant and total bacteria, respectively, in the secondary type of municipal wastewater treatment plant (Luo et al., 2014). A significant positive correlation of CRBP and suspended solids suggests that CRBP is removed from wastewater with the primary and excess secondary activated sludge, a process which needs future examination.
High numbers of CRBP grown at 42°C suggest a high proportion of hospital wastewater in influent, and consequently the presence of bacteria of clinical origin in effluent of the investigated municipal wastewater treatment plant. Reduction of CRBP (54%) in the secondary wastewater treatment process was comparable to the reduction of intestinal enterococci (57%). This suggests the similar fate of CRBP and intestinal enterococci in the secondary type of municipal wastewater treatment plant. Although the secondary treatment of municipal wastewater significantly decreased the numbers of CRBP, it is not sufficient to completely eliminate the CRBP from sewage. Hospital wastewater is recognised as a diffusion reservoir of New Delhi metallo-beta-lactamase-1 (NDM-1) producing bacteria (Zhang et al., 2013). Although the NDM-1 represents one of many mechanisms of carbapenem resistance, genes encoding NDM-1 were present in the domestic and industrial wastewater and each stage of the wastewater treatment process, including the chlorinated effluent (Luo et al., 2014). The finding of KPC-2-producing Gram-negative bacteria after the passage of hospital wastewater through the tertiary wastewater treatment plant (Chagas et al., 2011) suggests a resistance of CRBP to the process of chlorine disinfection. Therefore, the upgrade of the secondary wastewater treatment plant to tertiary stage or conventional disinfection of effluent water does not seem to be a promising method for the elimination of CRBP from municipal wastewater in which hospital wastewaters are diluted with other types of wastewaters. Alternative methods of disinfection of hospital wastewater at the source of contamination seem a promising strategy for mitigating the propagation of CRBP in the environment.
CONCLUSIONS
CRBP grown at 42°C were found in the influent and effluent water of the secondary type of municipal wastewater treatment plant receiving untreated hospital wastewater. Median numbers of CRBP in influent and effluent water were 3.5 and 1.3 log CFU/mL with a prevalence among total heterotrophic bacteria of 47% and 26%, respectively. Higher numbers of CRBP in influent and effluent were found in cases of nutrient-rich wastewater with higher concentrations of total heterotrophic bacteria and intestinal enterococci. Reduction of CRBP in the wastewater treatment process of 54% was comparable to the reduction of intestinal enterococci. Since the CRBP grown at 42°C was not found in natural water samples beyond the vicinity of hospitals, these bacteria may be used as an indicator of hospital wastewaters.
ACKNOWLEDGEMENTS
This work has been supported by the University of Zagreb (project no. 202751) and in part by the Croatian Science Foundation (project no. IP-2014-09-5656).
REFERENCES
APHA, AWWA, WEF (2005) Standard Methods for the Examination of Water and Wastewater (21st edn.). American Public Health Association, New York. [ Links ]
CAMS (2014) Antibiotic Resistance in Croatia, 2013. The Croatian Academy of Medical Sciences, Zagreb. 52-54. [ Links ]
CHAGAS TPG, SEKI LM, DA SILVA DM and ASENSI MD (2011) Occurrence of KPC-2-producing Klebsiella pneumoniae strains in hospital wastewater. J. Hosp. Infect. 77 (3) 274-283. https://doi.org/10.1016/j.jhin.2010.10.008 [ Links ]
CHANDRAN SP, DIWAN V, TAMHANKAR AJ, JOSEPH BV, ROSALES-KLINTZ S, MUNDAYOOR S, LUNDBORG CS and MACADEN R (2014) Detection of carbapenem resistance genes and cephalosporin, and quinolone resistance genes along with oqxAB gene in Escherichia coli in hospital wastewater: a matter of concern. J. Appl. Microbiol. 117 (4) 984-995. https://doi.org/10.1111/jam.12591 [ Links ]
DIENE SM and ROLAIN JM (2014) Carbapenemase genes and genetic platforms in Gram-negative bacilli: Enterobacteriaceae, Pseudomonas, and Acinetobacter species. Clin. Microbiol. Infect. 20 (9) 831-838. https://doi.org/10.1111/1469-0691.12655 [ Links ]
EFSA Panel on Biological Hazards (2013) Scientific opinion on carbapenem resistance in food animal ecosystems. EFSA J. 11 (12) 3501-3571. https://doi.org/10.2903/j.efsa.2013.3501 [ Links ]
EUCAST (European Committee on Antimicrobial Susceptibility Testing) (2014) EUCAST Reading guide. Version 4.0. EUCAST, Vaxjo. [ Links ]
FERREIRA AE, MARCHETTI DP, DE OLIVEIRA LM, GUSATTI CS, FUENTEFRIA DB and CORCAO G (2011) Presence of OXA-23-producing isolates of Acinetobacter baumannii in wastewater from hospitals in southern Brazil. Microb. Drug Resist. 17 (2) 221-227. https://doi.org/10.1089/mdr.2010.0013 [ Links ]
GALLER H, FEIERL G, PETTERNEL C, PEINTHALER FF, HAAS D, GRISOLD AJ, LUXNER J and ZARFEL G (2014) KPC-2 and OXA-48 carbapenemaseharbouring Enterobacteriaceae detected in an Austrian wastewater treatment plant. Clin. Microbiol. Infect. 20 (2) 132-134. https://doi.org/10.1111/1469-0691.12336 [ Links ]
GIRLICH D, POIREL L and NORDMANN P (2010) First isolation of the blaOXA-23 carbapenemase gene from an environmental Acinetobacter baumannii isolate. Antimicrob. Agents Chemother. 54 (1) 578-579. https://doi.org/10.1128/AAC.00861-09 [ Links ]
HRENOVIC J, GOIC-BARISIC I, KAZAZIC S, KOVACIC A, GANJTO M and TONKIC M (2016) Carbapenem-resistant isolates of Acinetobacter baumannii in a municipal wastewater treatment plant, Croatia, 2014. Euro Surveill. 21 (15) 21-30. https://doi.org/10.2807/1560-7917.ES.2016.21.15.30195 [ Links ]
HRN ISO 7899-2 (2000) Water quality - Detection and enumeration of intestinal enterococci, Part 2: membrane filtration method. Organization for Standardization, Geneva. [ Links ]
LUO Y, YANG F, MATHIEU J, MAO D, WANG Q and ALVAREZ PJJ (2014) Proliferation of multidrug-resistant New Delhi metallo-β-lactamase genes in municipal wastewater treatment plants in northern China. Environ. Sci. Technol. Lett. 1 (1) 26-30. https://doi.org/10.1021/ez400152e [ Links ]
MELETIS G (2016) Carbapenem resistance: overview of the problem and future perspectives. Ther. Adv. Infect. Dis. 3 (1) 15-21. https://doi.org/10.1177/2049936115621709 [ Links ]
OPAZO A, DOMINGUEZ M, BELLO H, AMYES SG and GONZALEZ-ROCHA G (2012) OXA-type carbapenemases in Acinetobacter baumannii in South America. J. Infect. Dev. Ctries. 6 (4) 311-316. [ Links ]
PICAO RC, CARDOSO JP, CAMPANA EH, NICOLETTI AG, PETROLINI VB, ASSIS DM, JULIANO L and GALES AC (2013) The route of antimicrobial resistance from the hospital effluent to the environment: focus on the occurrence of KPC-producing Aeromonas spp. and Enterobacteriaceae in sewage. Diagn. Microbiol. Infect. Dis. 76 (1) 80-85. https://doi.org/10.1016/j.diagmicrobio.2013.02.001 [ Links ]
POIREL L, BARBOSA-VASCONCELOS A, SIMOES RR, DA COSTA PM, LIU W and NORDMANN P (2012) Environmental KPC-producing Escherichia coli isolates in Portugal. Antimicrob. Agents Chemother. 56 (3) 1662-1663. https://doi.org/10.1128/AAC.05850-11 [ Links ]
SENTA I, TERZIC S and AHEL M (2013) Occurrence and fate of dissolved and particulate antimicrobials in municipal wastewater treatment. Water Res. 47 (2) 705-714. https://doi.org/10.1016/j.watres.2012.10.041 [ Links ]
SOUSA C, BOTELH J, SILVA L, GROSS F, NEMEC A, LOPES J and PEIXE L (2014) MALDI-TOF MS and chemometric based identification of the Acinetobacter calcoaceticus-Acinetobacter baumannii complex species. Int. J. Med. Microbiol. 304 (5-6) 669-677. https://doi.org/10.1016/j.ijmm.2014.04.014 [ Links ]
TANNER WD, VANDERSLICE JA, TOOR D, BENSON LS, PORUCZNIK CA, GOEL RK and ATKINSON RM (2015) Development and field evaluation of a method for detecting carbapenem-resistant bacteria in drinking water. Syst. Appl. Microbiol. 38 (5) 351-357. https://doi.org/10.1016/j.syapm.2015.03.010 [ Links ]
WALSH TR, WEEKS J, LIVERMORE DM and TOLEMAN MA (2011) Dissemination of NDM-1 positive bacteria in the New Delhi environment and its implications for human health: an environmental point prevalence study. Lancet Infect. Dis. 11 (5) 355-362. https://doi.org/10.1016/S1473-3099(11)70059-7 [ Links ]
ZAVASCKI AP, BULITTA JB and LANDERSDORFER CB (2013) Combination therapy for carbapenem-resistant Gram-negative bacteria. Expert Rev. Anti. Infect. Ther. 11 (12) 1333-1353. https://doi.org/10.1586/14787210.2013.845523 [ Links ]
ZHANG C, QIU S, WANG Y, QI L, HAO R, LIU X, SHI Y, HU X, AN D, LI Z, LI P, WANG L, CUI J, WANG P, HUANG L, KLENA JD and SONG H (2013) Higher isolation of NDM-1 producing Acinetobacter baumannii from the sewage of the hospitals in Beijing. PLoS ONE 8 (6) e64857. https://doi.org/10.1371/journal.pone.0064857 [ Links ]
Received 8 August 2015
Accepted in revised form 6 March 2017
* To whom all correspondence should be addressed: Tel: +385 1 48 77 700; Fax: +385 1 48 26 260; e-mail: jasna.hrenovic@biol.pmf.hr


{kind=link}
{kind=link}