










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkJournal of Contemporary Management
versão On-line ISSN 1815-7440
JCMAN vol.4 no.1 Meyerton 2007
RESEARCH ARTICLES
Global trends in the EMS treatment of indigent patients
C Kennedy
Department of Business Management, University of Johannesburg
ABSTRACT
This article gives an overview of the global trends in the treatment of indigent EMS (Emergency Medical Service) patients. Following an introduction to Netcare 911, the article starts with clarifying the definition of "indigent" from a specifically global perspective. The article then explores this topic in the South African context from which a broader global overview is taken, with particular research honing into four nations i.e. Singapore, Unites States of America, United Kingdom and Canada. Before making a final conclusion, the argument of whether it is a social, political or economic issue is contemplated.
Key words: Emergency Medical Services (EMS), health care, indigent patients, medical insurance, global perspectives
1 INTRODUCTION TO NETCARE 911
Netcare 911 is the wholly-owned pre-hospital risk management and emergency assistance subsidiary of Network Healthcare Holdings Limited (Netcare), which operates and manages the largest hospital and doctor network in the world outside of the Unites States of America. Netcare 911 is Africa's largest private emergency service and operates on a for-profit basis.
Operations have been mostly based in South Africa since its inception in 1998, however more recently Netcare 911 has expanded into surrounding countries such as Swaziland, Mozambique and Botswana. In 2006, Netcare 911 expanded its aero-medical evacuation capabilities in Nigeria to service the West African region (Netcare Insight 2006:90).
Its ever expanding infrastructure includes 1150 paramedical and administrative staff, 508 emergency vehicles, a fleet of four fixed wing aircraft and a number of helicopters. The customer base during 2006 increased to over nine million lives with emergencies attended to exceeding 167 000 (Netcare annual report 2006:40).
2 DEFINING "INDIGENT" PATIENTS
The Readers Digest Great Illustrated Dictionary (1984:857) defines indigent as "lacking the means of subsistence" or "a destitute or needy person". Findings from Stiglitz (2006:11) indicate that approximately 40 percent of the world's 6.5 billion people live in poverty. Poverty according the World Bank is defined as living on less than two United States Dollars (USD) per day.
A lot of previous research has tried to understand the dynamics behind the general treatment of indigent patients throughout the health care system from primary to tertiary care. The distinction this research attempts to make is the provision of EMS treatment to indigent patients. The requirement of immediate and non-discriminate assistance to patients in these circumstances could be the difference between life and death.
Addy (1996) maintains that "health care is a basic right for the good of the individuals and for the overall health of the community at large". Previous research has shown that there is a correlation between the perceived level of health and the financial status of the uninsured - which do not enjoy the same level of health as the insured (Lucey 2001). This continuum extends to even mortality rates, adverse health outcomes and the need for avoidable inpatient hospital care.
3 NETCARE'S APPROACH TO TREATING INDIGENT EMS PATIENTS
Since its inception, Netcare 911 has been fully committed to treating all patients with equal dignity and priority. They are fully aligned to the National Patients' Rights Charter (HPCSA 2002) which states that among others, every patient "has the right to; access to safe health care".
Policies within the organisation make special reference to the treatment of indigent patients and clearly states "under no circumstances should a patient requiring emergency medical attention be denied assistance irrespective of their financial or medical aid status" (Netcare Policy 2004:19). The policy further requires hospital management to be informed of any indigent patients receiving medical attention.
In an interview conducted with Mrs. MC Nel (Nel 2007), Netcare's group risk manager, she further explained that in the event of receiving and indigent patient, paramedics are required to pre-arrange transport for the patient to the nearest appropriate public sector medical facility. However, in some instances this is not possible and ultimately results in the patient being transported to the nearest Netcare facility. The increasing complexity behind subsequently transferring these patients to public sector facilities once treated in an emergency situation, has lead to an increase in cases of these patients' medical needs being satisfied at Netcare facilities as far as possible (Netcare Annual Report 2006:94).
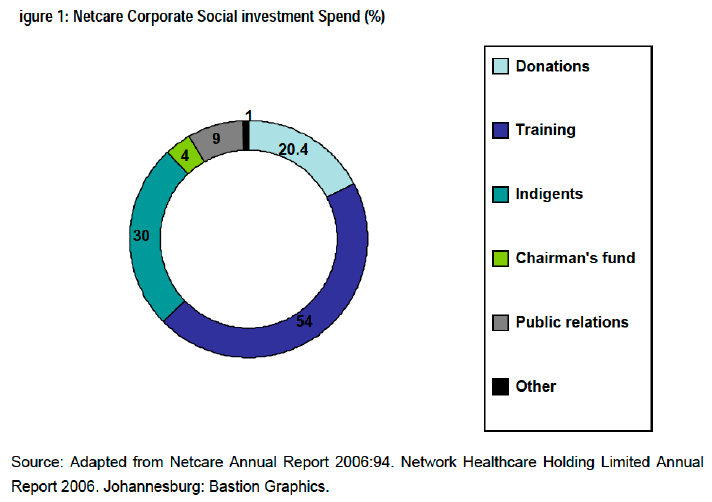
Netcare 911's legitimate support of indigent patients is further evident in the reported R18 million spent on treating indigent patients (Netcare Annual Report 2006:94). The treatment of indigent patients reflected 30 percent of the groups' total corporate social investment spends for the 2006 financial year as reflected in the diagram below.
4 TREATING INDIGENT EMS PATIENTS IN THE SOUTH AFRICAN CONTEXT
The EMS environment in South Africa is diverse in its operations and structures. Ranging from government managed and controlled to private and even volunteer EMS organisations.
Private operators include national EMS providers such as Netcare 911 and ER24 who both are affiliated to private hospital groups. Smaller operators such as Emoyeni Medical Rescue and Table Bay Rescue operate at provincial and even city level. Just as there is a vast divergence in the ownership and management of these operators, so too they differ in the services they provide. These range from basic patient transport to more comprehensive solutions such as medical events standby, paramedic placements and home assistance programmes. The expansion of services offered, provides a platform for these organisations to generate profits.
The increased subsidization of medical aid for government employees along with the introduction of the Government Employees Medical Schemes (GEMS) and the Low Income Medical Schemes (LIMS) is expected to bring considerable numbers of employed, currently uninsured people into the medical scheme pool.
Watson (2007:21) reports that GEMS has become a serious force as it reached the magical milestone of covering 100 000 principal members, which signifies close to 300 000 South African lives. This makes it one of the five largest medical schemes in the country. Netcare 911 was awarded the GEMS tender for the provision of emergency medical services.
The Department of Health introduced a policy in 2004 according to which it would remunerate private health care companies for the treatment of indigent patients. To date, no payment has been made to any such parties. (Nel 2007).
5 GLOBAL PERSPECTIVES ON THE TREATMENT OF INDIGENT PATIENTS
The effects of globalization is even being felt in what has been traditionally considered a local industry, that of health care (Hill 2007:3). The global shortage in medical professionals combined with the surge in medical technology has lead to an enigma not only to the World Health Organization (WHO) but also to local governments and the private health care enterprises operating in these economies.
According to Friedland, (Netcare Annual Report 2007:21), health care is globally at a cross roads. He substantiates this by explaining that developments in medical sciences and technology "hold the promise of healthier nations world-wide" however the costs of providing health care are rising. In many countries the high cost of health care, inadequate coverage, complex administrative procedures and overall public dissatisfaction (Lucey 2001) has lead observers to conclude that health care is in a crisis.
Governments worldwide have adopted a hybrid approach to providing health care infrastructure. French (1995) reported the conflict of the traditional fee-for-service approach which results in uninsured or indigent patients relying on hospital emergency departments for basic care. The incongruity of this approach is the irony that the treatment of minor ailments in an emergency department can cost up to five times more than if treated in a primary health care environment. Thus, further incentivising hospitals to encourage this perverse cycle.
French (1995) further contemplates the principles of managed care in guiding indigent patients toward preventative care. This should be further supported by the appointment of a primary care doctor resulting in emergency department visits being restricted to true emergencies.
6 SOME COUNTRY SPECIFIC RESEARCH
6.1 Singapore
A dual health care delivery system provides health care to this nations' population of 4.2 million people. Eighty percent of primary health care services are provided by private practitioners with the remainder being provided by state polyclinics (WHO n.d.:1). The state ensures the availability of affordable basic medical services through heavily subsidized services at public hospitals and government clinics. At the state polyclinics, citizens under the age of 18 and over the age of 65 enjoy a discount of up to 75 percent on treatment and consultation fees. Where required, other citizens qualify for a 50 percent discount (WHO n.d.:2).
The WHO regional office for the Western Pacific (WHO n.d.:1) further reports that EMS services are provided by the Singapore Civil Defense Force for the transportation of accident and trauma cases. For emergency services, patients have access to 24 hour accident and emergency department located in state hospitals.
The substantial health care subsidies provided through state, ensure that even in a country with the fifth highest per capita gross domestic product in the world (Singapore Ministry of Health n.d.:1), the potential indigent population's EMS needs are comprehensively met.
6.2 United States of America
According to the American College of Emergency Physicians (ACEP n.d.:1), almost 46 million Americans are uninsured. A health care safety net exists thanks to providers who have a legal mandate or mission to provide health care to all patients irrespective, of their ability to pay.
The Emergency Medical Treatment and Labor Act (EMTALA) is one of these legally mandated safety nets. This law ensures that anyone can receive access to EMS in the form of a medical screening exam and if required, to be stabilized. Particular further protection is given to children, who according to the State Children's Health Insurance Program (SCHIP) qualify for physician visits, prescription medicine and hospitalisation at little or no cost (ACEP n.d.:2).
Previously, hospitals shifted uncompensated costs to insured patients, however this option will not be viable in the near future due to the introduction of strict price controls, leaving little margin to shift these costs. It is estimated that one third of physicians lose up to an average of $138 000 per year as a result of EMTALA related bad debt (ACEP n.d.:3).
6.3 United Kingdom
The majority of EMS services in the United Kingdom (UK) are provided by the National Health Service (NHS). Although Netcare recently acquired the largest stake of the private health care sector in the UK through its 52,63 percent controlling stake in General Healthcare Group Limited (GHG), Netcare 911 has not been able to expand its EMS footprint in this country. In lieu of creating their own infrastructure, private operators purchase non-emergency transport on a contractual basis (NHS: n.d).
Netcare has a longstanding track record with the NHS and has been awarded many tenders for the provision of a wide range of outsourced services (Netcare Annual Report 2006:49). The NHS' increased spending in an attempt to improve health care standards to European levels has resulted in many portions of its health care delivery being outsourced. Creating a potential entry point for Netcare 911.
The UK's Emergency Operations Centre is the largest emergency operations centre in Europe, receiving up to 3 000 calls daily. These calls incorporate both insured and indigent patients.
A low five to six percent of the population has private medical insurance (NHS:2004). Thus the remarkable dependence on the NHS could be contributable to the fact that according to the WHO it is one of the best health services in the world.
6.4 Canada
The overall Canadian population (32 million people) is ageing rapidly with the population over 65 more than doubling in the past 35 years. The health care system entails federal, provincial and territorial governments sharing the responsibility. This system gives all Canadians access to health care and was implemented in 1968 (Statistics Canada).
In Canada, the Ministry of Health pays for most of the costs for medical transport including air transport. Patients typically pay $45 (Canadian) of the cost, however there are some exceptions. In cases where the trip is not medically necessary or if the patient does not have a Health Card, they are required to pay a fee of $240. The fee is forfeited where the patient is receiving provincial social assistance which could be in the form of either general welfare of family benefits (EMS Toronto n.d.:1)
7 IS IT A SOCIAL, POLITICAL OR ECONOMIC ISSUE?
7.1 Economic
Curran (1997:233) asks "what kind of ethical accountability do health care clinical leaders owe to their institution, their patients, and to the tax-paying public?". She goes on to explore several factors that affect the ethics behind health care service providers including the critical need for being profitable. Treating indigent patients puts a strain on the organisations' profit potential.
This scenario is further delineated by Tuckman (1990:9) who argues that the cost of indigent care is more accurately being paid for by the insured population. Leaving the financial burden on private individuals.
7.2 Political
Lucey (2001) contends that is up to local governments to address health care policy with the ensuing implementation of programs to meet the needs of the indigent.
The impact of nonprofit health care is precariously being debated in the political arena. According to Horwitz (2006:308), in the USA, state policymakers have suggested requirements that nonprofit health care organisations spend minimum revenue percentages on free care for indigent patients. These proposals furthermore extend to the private sector.
In 1986, American Congress passed the federal anti-dumping legislation, the purpose of which was to prevent the transfer of unstable emergency patients for economic reasons (Enfield & Sklar n.d.:579). Demonstrating that the problem has reached the levels of requiring state intervention.
7.3 Social
According to Barry and Keough (2005:48), the true problem is societal. 44 million of the American population is without insurance. The problem is compounded as the majority of the uninsured have incomes less than 200 percent of the federal poverty income level. This trend is certainly more intensely experienced globally, where as previously stated 40 percent of the global population is considered indigent.
Research by O'Toole (1999:215) indicates that medical training can have a direct impact on the treatment of indigent patients pertaining to the attitudes of students. Increased social investment by medical practitioners could lead to a pivotal turnaround in health care. Lyon (2003:501) reports that the new model of medical education focuses on the provision of services to indigent patients in certain urban areas in exchange for student and resident education. Does this imply that the indigent are the guinea pigs of health care?
Horwitz (2006:311) asserts that irrespective of the individual's wealth, level of disability or insurance status, access to health care institutions that can be trusted will always be needed.
8 CONCLUSION AND RECOMMENDATIONS
The growing number of the medically uninsured population, compounded globally by the increasing competition for a smaller pool of funding has created an increased strain on organisations that have traditionally served indigent patients.
There is no single panacea to this global predicament in health care. Accountability for solutions can not be pointed to any singular party e.g. state, private sector, medical professionals or even the insured public. The dilemma is getting consensus from all these parties.
The debate of whether the treatment of indigent patients in the primary health care setting is an economic, political or social issue can not be explicitly answered. However, a robust argument can be made in the case of the treatment of indigent patients in the EMS environment.
Global human rights (barring some extremist countries) consistently equate the equal treatment of all people irrespective of financial status. This is more underscored where the person is in a life-threatening predicament where the need for EMS is critical to saving such a life.
The global disparity in health care systems furthermore means that there is no singular solution. The recommendation therefore is that each nation in consultation with the WHO and other world governing bodies e.g. the United Nations (UN) or the World Bank, seek individual solutions to meet the needs of indigent patients in their countries. Clearly, this has already been undertaken by most countries, but the need for deeper interrogation of the key drivers is required. The more explicit change in this approach is the requirement that each nation includes all stakeholders in their discussions.
World poverty and health issues are not likely to be abolished. Diseases like malaria and HIV are certainly accounting for larger mortalities globally, particularly among indigents. However by ensuring that as a minimum EMS services for the indigent are consistently available, a further enhancement to overall indigent health care will be noted.
BIBLIOGRAPHY
Addy J. 1996. Issues of access: What is going on in health care? Nursing Economic$, 14(5):299-301. Available from: EBSCOHost: CINAHL: http://search.global.epnet.com/ [Downloaded: 2007-03-18]. [ Links ]
ACEP> American College of Emergency Physicians. Not dated. The Uninsured: Access to Medical Care. Available from: http://www.acep.org/webportal/PatientConsumers/critissues/UninsuredUnderinsured/ [Accessed: 2007-03-19]. [ Links ]
Barry D & Keough CL. 2005. Ready for prime time? Make your financial assistance policy a class act. Healthcare financial management; 48-55. Available from: EBSCOHost: Health Source - Consumer Edition: http://search.global.epnet.com/ [Downloaded: 2007-03-18]. [ Links ]
Curran CR. 1997. Whose needs are being met? Nursing Economic$, 15(5)233,278. Available from: EBSCOHost: CINAHL: http://search.global.epnet.com/ [Downloaded: 2007-03-18]. [ Links ]
Enfield LM & Sklar DP. Not dated. Patient dumping in the hospital emergency department: Renewed interest in an old problem. Available from: EBSCOHost: CINAHL: http://search.global.epnet.com/ [Downloaded: 2007-0318]. [ Links ]
French B. 1995. Medicaid managed care tackles emergency use - with mixed results. Hospitals & Health Networks, 69(4). Available from: EBSCOHost: Health Source - Consumer Edition: http://search.global.epnet.com/ [Accessed: 2007-03-18]. [ Links ]
Friedland R. 2006. Network Healthcare Holding Limited Annual Report 2006. Johannesburg: Bastion Graphics. [ Links ]
Hill CWL. 2007. International Business. Competing in the Global Marketplace. Sixth ed. New York: McGraw-Hill. [ Links ]
Horwitz J. 2006. Nonprofit ownership, private property, and public accountability. Implementing policies that undermine the private nature of nonprofits is risk. Perspectives, 308-311. EBSCOHost: Health Source -Consumer Edition: http://search.global.epnet.com/ [Downloaded: 2007-03-18]. [ Links ]
Health Professions Council of South Africa (HPCSA). 2002. Guidelines for good practice in medicine, dentistry and the medical sciences. National Patient's Rights Charter. Pretoria, (13). Available from: http://www.hpcsa.co.za/hpcsa/UserFiles/File/Patient'sRightsCharter.pdf [Downloaded: 2007-03-22]. [ Links ]
Lucey P. 2001. An access program for medically indigent individuals. Nursing Economic$, 19(1). Available from: EBSCOHost: CINAHL: http://search.global.epnet.com/ [Accessed: 2007-03-18]. [ Links ]
Lyon DS. 2003. Medical education in indigent patient care. Current Women's health reports, 3(6)501-504. Available from: EBSCOHost: CINAHL: http://search.global.epnet.com/ [Accessed: 2007-03-18]. [ Links ]
Nel MC. 2007. Verbal communication with the author. Johannesburg. (Notes in possession of the author. [ Links ])
Netcare Insight 2006. Johannesburg: Cannon Medical Media. [ Links ]
Network Healthcare Holdings. 2004. Emergency Medical Services Patient Care Policy 54(4)19. Johannesburg: Netcare Quality Care Steering Committee. [ Links ]
Network Healthcare Holding Limited Annual Report 2006. Johannesburg: Bastion Graphics. [ Links ]
National Health Service. Not dated. OtherNHS Help. Available from: http://www.lond-amb.sthames.nhs.uk/helpweoffer/other/other_main.html. [ Links ]
O'Toole TP. 1999. Experiences and attitudes of residents and students influence voluntary service with homeless populations. J Gen Intern Med, (14)211-216. Available from: EBSCOHost: CINAHL: http://search.global.epnet.com/ [Downloaded: 2007-03-18]. [ Links ]
The Reader's Digest Association Inc. 1984. Reader's Digest Great Illustrated Dictionary. New York: The Reader's Digest Association Limited. [ Links ]
Statistics Canada. Not dated. Health. A changing health care system. Available from: http://www41.statcan.ca/2966/ceb2966_000_e.htm [Accessed: 2007-03-21]. [ Links ]
Stiglitz J. 2006. Making globalization work. London: W.W.Norton and Company. [ Links ]
Toronto Emergency Medical Services. Not dated. Living in Toronto. Available from: http://www.toronto.ca/ems/overview/faz.htm [Accessed: 2007-03-19]. [ Links ]
Vastag B. 2003. Emergency Medical Treatment. Journal of the American Medical Association, 290(14):1 844. Available from: EBSCOHost: CINAHL: http://search.global.epnet.com/ [Downloaded: 2007-03-18]. [ Links ]
Watson E. 2007. GEMS now one of the five largest scheme in the country. The Star, 20 March:21. [ Links ]
World Health Organization. Not dated. Regional Office for the Western Pacific. Singapore Health Situation. Available from: http://www.wpro.who.int/countries/05sub/health_situation.htm [Accessed: 2007-03-18]. [ Links ]


{kind=link}