










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Higher Education
On-line version ISSN 1753-5913
S. Afr. J. High. Educ. vol.37 n.5 Stellenbosch Oct. 2023
http://dx.doi.org/37-5-5181
GENERAL ARTICLES
Desktop analysis and qualitative investigation of programmes and initiatives for the prevention of and response to gender based violence at South African universities with medical campuses
M. HewettI; L. Butler-KrugerII; K. FoflonkerIII; J. EdgeIV; M. H. BothaV; S. SeedatVI
IFaculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa. Department of Psychiatry. https://orcid.org/0000-0002-4995-0002
IIFaculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa. Department of Psychiatry. https://orcid.org/0000-0002-0082-4427
IIIFaculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa. Division Student Affairs
IVFaculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa. Division of Surgery. https://orcid.org/0000-0003-3005-7254
VFaculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa. Department of Obstetrics and Gynaecology. https://orcid.org/0000-0002-6046-1453
VIFaculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa. South African Medical Research Council Unit on the Genomics of Brain Disorders Department of Psychiatry. https://orcid.org/0000-0002-5118-786X
ABSTRACT
Gender-based violence (GBV) is pervasive at South African higher education institutions (HEIs). Based on a media statement (dated 6 October 2016) by the Department of Higher Education and Training, GBV programmes at HEIs need to be evidence-informed, responsive, contextually relevant, inclusive and person-centred. The present article aims to explore the nature of GBV programmes currently implemented at HEIs in South Africa. A rapid review of the literature, supported by qualitative interviews with representatives of South African HEIs with medical campuses, was conducted. Findings indicate that there is an urgent need to clearly define GBV and to mention it explicitly in policy documents. In addition, research evidence on the effectiveness of prevention and response interventions at HEIs in South Africa is lacking. Challenges highlighted by the HEIs that were surveyed include the lack of trust by staff and students in the response and action plans of the response/task teams at HEIs, uncertainty with regards to the roles of relevant stakeholders and sectors when reporting incidents, as well as insufficient information about what GBV is. This study is intended to provide a baseline for further research evaluating current GBV programmes on medical campuses at HEIs, and highlights the need for an evidence-informed framework of the key ingredients for effective GBV response and prevention programmes.
Keywords: Gender-based violence, rapid review, qualitative interviews, higher education institutes, medical campuses, South Africa.
INTRODUCTION
Gender-based violence (GBV) is pervasive at South African higher education institutions (HEIs). Gender-based violence (GBV) is a widespread public health, social and economic concern that is systemic and deeply entrenched in institutions, cultures and traditions (Decker et al. 2015). GBV is defined as "violence that is directed against an individual or group of individuals based on their gender" (Cruz and Klinger 2011). It involves violence against women and girls as well, against men and boys, people who are lesbian, gay, bisexual, transgender and intersex ( LGBTQIA+), and other individuals who do not conform to dominant gender roles (ILO 2012). The critical consequences of GBV are extensive and necessitate long-term interventions (WHO 2020; Calvete, Corral, and Estévez 2007).
Globally, the WHO estimates that more than 30 per cent of women have experienced either physical or sexual intimate partner violence and 6 per cent of women have experienced non-partner sexual assault (Violence against women Prevalence Estimates 2018). In South Africa rates of GBV are thought to be much higher than the global average, yet accurate and official statistics are often difficult to obtain (Machisa et al. 2011; Abrahams et al. 2013). It is difficult to obtain statistics related to sexual harassment, intimidation in the workplace and at educational institutions since these forms of GBV are difficult to quantify (Sloand et al. 2015; WHO 2013). Non-disclosure of GBV also obscures prevalence statistics given that it is estimated that less than 40 per cent of the women who experience GBV seek help of any sort and less than 10 per cent of those seeking help appeal to the police (United Nations Economic and Social Affairs 2015). Addressing GBV is a complex issue requiring a multi-faceted undertaking. Recent publicised incidents of GBV on university campuses, coupled with attempts to downplay the occurrence of GBV and/or perpetrators not being held accountable, has emphasised the need for these institutions to complement societal interventions for GBV by implementing institutional interventions (Saferspaces n.d).
It has been suggested that a high number of GBV acts, especially rape, are reported by South African university students, however, there are no nationally representative data documenting the extent of GBV on South African Higher Education Institutions (HEI) campuses (Davids 2020). While a few South African studies related to GBV programmes at HEIs have been published, little is known about the implementation, strengths and limitations of these programmes (Abrahams et al. 2013). To explore the nature of GBV programmes implemented at HEIs in South Africa, we conducted a rapid review of the literature. The rapid review was complemented by qualitative interviews with representatives of South African HEIs with medical campuses.
METHODS
Information was gathered and triangulated by empoying the following methods:
A rapid review of the literature
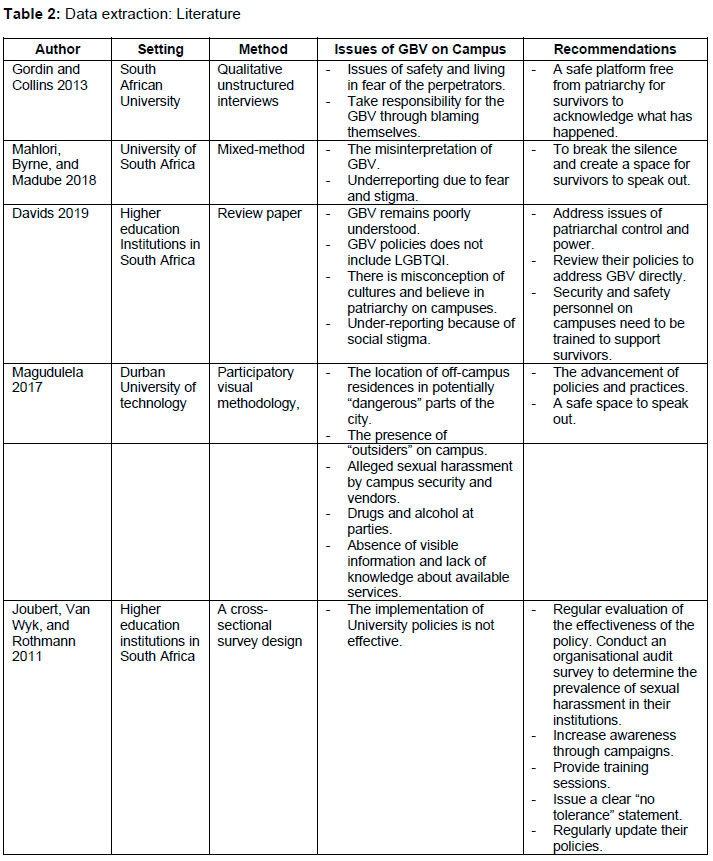
A systematic search of the following databases was conducted in October 2020 for published literature between the years 2000 and December 2020: Ebscohost (African wide Information); Sabinet African Journals and JSTOR using search terms: Gender-based violence OR Violence against women AND Higher education institutions OR Universities AND Preventative interventions AND/OR Response interventions, independently by two researchers. Studies were excluded if they were not in English or not conducted in South Africa or at a higher educational institution in South Africa. Five publications related to components of GBV programmes/initiatives at HEIs in SA were retained. A data extraction form was used to collect information on: The setting of the study, the method, issues related to GBV on campuses and recommendations made. In an effort to gain a richer understanding of GBV at HEIs, grey literature (which represents information gleaned from non-traditional publishing and distribution channels, and which is often not well represented in scientific) indexing databases). was incorporated in the discussion.
A review of policy frameworks
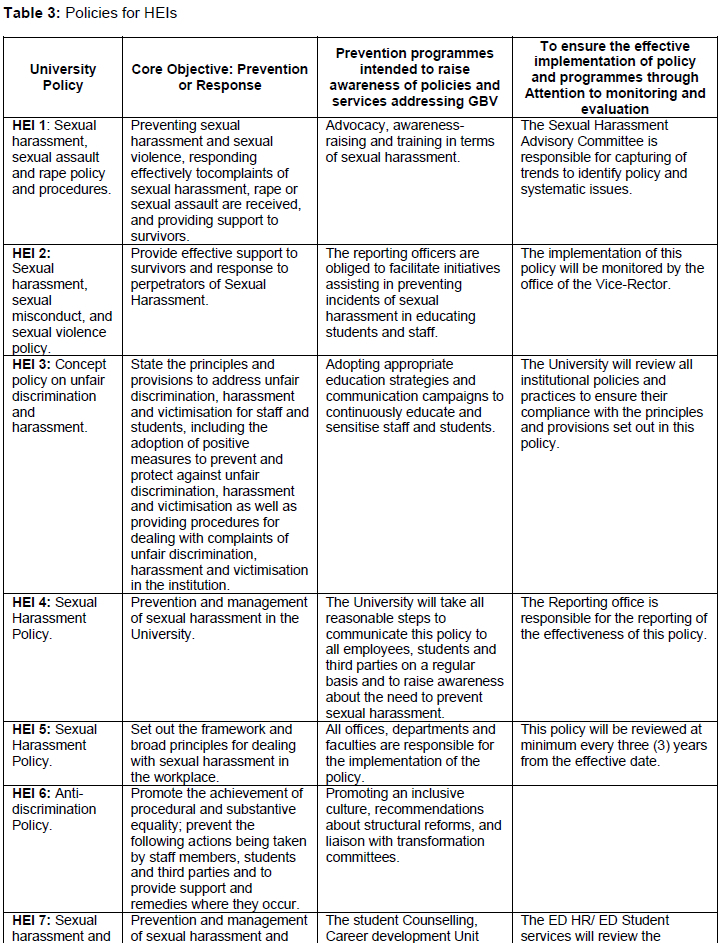
Nine universities were identified as offering medical training in South Africa (2020). The policies of these universities were requested with only three universities providing their policies. The policies of four additional universities were available online. Thus a total of 7 university policies were studied and a data extraction form was used to collect information based on their policies' core objective, their efforts to raise awareness and the implementation of their proposed policies.
Qualitative interviews with university representatives
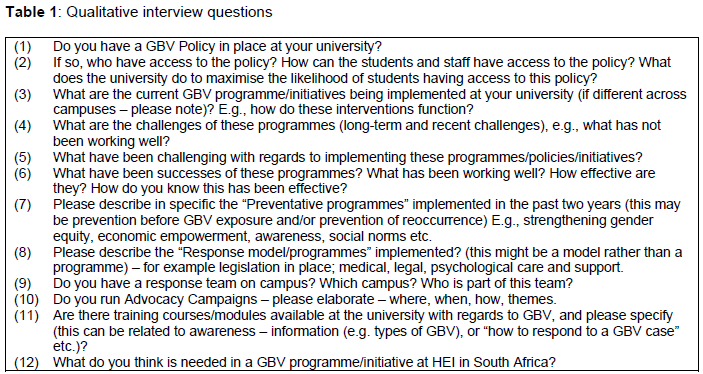
An introductory email was sent to a representative(s) of each university, with the request to provide information on the nature of the GBV programmes implemented at the respective university and their GBV policy. A minimum of 2 and maximum of 6 follow-up emails were sent and where this was not successful telephonic contact was made/attempted. Qualitative semi-structured interviews (Table 1) were conducted by a researcher with a representative at each university, comprising a total offive universities with medical campuses in South Africa. Representatives of four universities did not respond to the introductory/follow-up emails and phone calls. One university (of the five that did respond) reported that there were no GBV programmes or initiatives implemented at their campus at present. Interviews followed the recommendations for face-to-face qualitative interviewing proposed by Creswell (2007), DiCicco-Bloom and Crabtree (2006), Sandelowski (2000), and Paley (2010), with questions centred around a set of predetermined open-ended questions, with other questions emerging from the dialogue between the interviewer and interviewee.
Ethical considerations
Ethical clearance was not required as this study did not represent human subjects research. University representatives who participated in the qualitative interviews reported on their university policies and initiatives. An email to the respective university representative of all HEIs with medical campuses providing information about the study and an explicit phrase that their participation and contribution was entirely voluntary. For the purpose of this research, informed consent was tacitly obtained. Participants were informed of the aim, nature and extent of the study. It was further stated that if any HEI representative preferred not to be included in the write-up, this would be respected. Confidentiality of participant data was ensured by not revealing the names of participants or the identity of the respective universities. Numbers were allocated to both universities and participants to preserve their anonymity. The data were safely stored on a password protected computer.
Data analysis
The interviews were recorded, transcribed, coded, annotated and analysed using a thematic approach. The themes identified were compared with the original interview questions and objectives. The findings were contextualised in existing theory or evidence-based literature.
RESULTS
Literature review
From the literature, it emerged that GBV programmes are generally directed at prevention and response (see Table 2). The knowledge base of preventative and response initiatives on HEI in South Africa remain limited. While researchers around the globe agree that prevention programmes are a central component of the response of institutions of higher education to GBV, little is known about the structure and content of the strategies currently being used at HEIs in South Africa.
A key entry point in addressing GBV at HEIs is the appropriateness of their Campus Support and Response Structures. Most institutions have a strong focus on making GBV part of student curriculum, based on the premise that education and curricula have an important role to play in the prevention of GBV (Davids 2020). HEIs have a range of support structures available to survivors of GBV with further counselling and legal assistance (Gordin and Collins 2013).
From the literature it is evident that many HEIs may have policies in place (Gordin and Collins 2013; Mahlori, Byrne, and Madube 2018; Davids 2019). However, what is clearly emphasised is the non-adherence of staff and students (Gordin and Collins 2013; Mahlori, Byrne, and Madube 2018; Davids 2019). Studies highlight the need for these programmes to be implemented, however many had limited knowledge of policies at HEIs, nor awareness of the processes to follow when faced with GBV.
Qualitative interviews
Qualitative data obtained in this study support the need for prevention and response efforts. Most participants reported that there was a need for GBV prevention strategies to be intrinsically linked to efforts to enhance gender equality across the board. Three participants indicated that effective support was provided to survivors of GBV, namely individual case support which often includes legal advice. The importance of effective referral systems to counselling/therapeutic services for students who are survivors of GBV was also noted by these participants. The lack of knowledge of GBV as a contributory factor to poor identification and a failure of redress, were echoed.
We highlight a few key aspects based on key themes that emerged from the literature and qualitative interviews.
Characteristics of gender-based violence programmes
Available GBV programmes have a strong focus on participants' relationship skills through gender transformative interventions. The programmes aim to improve stress management, mental health as well as value-based decision-making. Programmes include the "WITS against GBV" and the South African NGO Sonke Gender Justice programme. The Sonke CHANGE Trial is based on Sonke's existing multi-level intervention "One Man Can" with the final goal of reaching gender equality. Other preventative programmes and initiatives against GBV include survivors' empowerment and bystander approaches (Singh et al. 2016).
Qualitative data indicate similar characteristics of GBV programmes. The need for awareness campaigns as part of the prevention strategy - for both staff and students - was highlighted. Three participants reported that there was minimal implementation of awareness strategies in 2020 as a result of COVID-19. One participant reported a moderate level of implementation of awareness strategies in 2020. This participant reported the use of social media to be particularly helpful during social containment restrictions in 2020. Most participants were in agreement that awareness programmes need to focus on addressing the core drivers of GBV. The topics that were highlighted were normative role expectations and unequal gendered/power relationships. All participants reported that they were planning to implement awareness campaigns for both staff and students. Three participants endorsed the need for, and continuation of, information sessions and training in their programmes for both staff and students.
Policy frameworks on gender-based violence
The purpose of institutional policy is to provide an environment in which staff and students feel safe. From the available policies (see Table 3), it can be seen with the exception of one university that directly unpacks GBV in its policy, all policies are directed at sexual assault and harassment. Thus, policies lack a clear definition and understanding of GBV. All policies (see below) aim to both prevent and respond to sexual harassment effectively, by outlining all procedures whether formal or informal that could be taken, possible consequences for perpetrators, and the support available to survivors as well as perpetrators. According to the literature sourced, even though HEIs have these policies in place non-adherence remains a challenge on many campuses.
From the qualitative interviews, all participants endorsed a zero-tolerance attitude to any act of violence. Three participants reported a recent or current re-formulation of their GBV policy framework. Three participants stressed that strengthening the legal and policy framework was an important element of both prevention of and response to GBV.
Sectors responsible for gender-based violence initiatives
The responsibility for GBV initiatives often lies with campus support offices. Highlighted in the literature is the need for more sectors to be involved, as support offices often fail in reaching the whole campus community in creating awareness and providing training (Gordin and Collins 2013; Mahlori, Byrne, and Madube 2018; Davids 2019; Magdulela 2017; Joubert, Van Wyk, and Rothman 2011).
Three universities reported in qualitative interviews the need to enhance multi-sectorial services and improved coordination among different sectors. Three representatives reported a clear and comprehensive response plan that was being implemented which included collaboration among various sectors.
Definition, risk factors and prevalence of gender-based violence
In contrast to other types of violence, GBV remains poorly defined (Davids 2020). At the current time, the central narrative and understanding of GBV is of male-on-female violence. This understanding has a number of ramifications. Firstly, the homogenisation of women as powerless (Davids 2020), which may result in the idea that women cannot be perpetrators of GBV. Secondly, the construction of gender as universal and static, and yet, as previous studies have highlighted (Butler 1999), gender is not consistently composed in different historical contexts, and intersects with social, class, ethnic, sexual and regional modalities of broadly comprised identities (Bulter 1999). The most common definition is that of the UN Declaration on the Elimination of Violence against Women: "any act of gender-based violence that results in, or is likely to result in, physical, sexual or psychological harm or suffering to women, including threats of such acts, coercion or arbitrary deprivations of liberty, whether occurring in public or private life". The "Policy Framework to address GBV in the Post-School Education and Training System" is similarly premised on the dominant view of GBV as male-on-female violence. Nonetheless, the policy framework does acknowledge that while GBV is often aimed at women as the noticeable bearers of the female, LGBTQI individuals may also experience GBV and become the targets of corrective rape and hate crimes (Davids 2020). The recent amendments to the South African Domestic Violence 2020 2B(1)(a) "Any person who has knowledge, reasonable belief or suspicion that an act of domestic violence has been committed against a child, person with a disability or an older person must report such knowledge, reasonable belief or suspicion immediately to a social worker or police official" (p16) state that staff members or students of HEI are now obligated to report any incidence of GBV on and around campus.
In August 2020, the government announced its new policy ("Policy Framework to Address Gender-based Violence in the Post-School Education and Training System") in the fight against GBV at educational institutions (Peta 2020). There are few South African studies of the prevalence of GBV at HEIs. A few studies that were undertaken have identified these occurrences in both students and staff, with perpetrators including staff, students as well as visitors (Sixsmith and Daniels 2011; Isaacs 2016; Braine, Bless, and Fox 1995; Clowes et al. 2009). In a public statement, the Deputy Minister of Higher Education, Science and Technology, Manamela claimed that 10 per cent of reported cases of rape across South Africa were reported by university students, excluding those from TVET colleges. An additional 62 per cent of students surveyed felt that female students would be sexually harassed on campus. The same study reported that approximately 28 per cent of males and 27 per cent of females (aged 15-19) considered women not to have the right to refuse sex with her partner and an alarming 55 per cent of male students thought that sexual violence does not include forcing sex with someone familiar (SAnews 2018). A study by Clowes et al., (2009), noted that female students (in their first year of studies) from poor, rural backgrounds are predominantly vulnerable to the transactional and unequal relationships often linked to forceful, intimidating and aggressive sexual practices.
There are several other factors that account for underreporting. A recent survey by UNISA, reported reasons for underreporting as fear of stigma and repercussions (Street and Arias 2001). Additional contributory factors are comparable to those reported in international literature and include: a) fear that the perpetrator will discover this and the potential consequences (Street and Arias 2001); b) lack of confidence in institutional response mechanisms (Decker et al. 2015) and c) anxiety over how the case will be conducted by the particular institution and/or police. There are a number of reasons as to why under-reporting is challenging and complex. Firstly, it is noted that survivors often do not receive the needed help and support. Secondly, it can be more challenging to bring perpetrators to justice. Thirdly, owing to under-reporting, the extent and nature of GBV on campuses is hard to determine which in turn pose a challenge in the development of GBV interventions. Furthermore, survivors can report both internally (student support etc) and externally (SAPS) which makes it harder to keep track of GBV incidences on HEI campuses.
The qualitative data support the need for clearer definitions of GBV concepts, as well as greater accuracy of GBV prevalence statistics at HEIs in South Africa. Three universities maintained that the disclosed violence or incidents reported do not reflect the actual prevalence and incidence of GBV.
Strengths and limitations of gender-based initiatives based on the literature, HEI policies and qualitative interviews
In a recent paper by Davids (2020), the challenges facing HEIs in South Africa are highlighted. One challenge is that students are often not fully informed as to "what to do" when confronted with GBV resulting in underreporting GBV. Furthermore, Gouws and Kritzinger (2007) found that only 56 per cent of heads of departments and even less members of the Women's Forum (36%) at a particular university in South Africa were aware of its sexual harassment policy. Similarly, Mahlori, Byrne and Madube (2018), refer to the same challenge with staff members often not fully trained on processes outlined by policies for reporting GBV on HEIs campuses and only few staff receiving training on implementation of these policies (Mahlor et al. 2018; Joubert et al. 2011). This further highlights that not only are staff members unaware of the processes outlined by the HEIs but that they also lack understanding of what constitutes GBV and when to take action, resulting in a "downplay" of the occurrence of GBV. Furthermore, students and staff differ in opinions on what constitutes sexual harassment from patriarchal and/or cultural perspectives (Davids 2020).
A second challenge of reporting incidents is the notion of women living in fear of their perpetrators (Gordin and Collins 2013: Davids 2019). Women often take the responsibility of the actions taken against them due to fear, allowing perpetrators to continue with violations and possibly allowing other women to fall victim to the same perpetrators (Gordin and Collins 2013). Many HEIs have offices responsible for receiving and following up on GBV claims and reports. However, students and staff may fear the patriarchal control and power in their institutions. Women report being fearful of being reprimanded for reporting cases of GBV as many reporting officers and security structures are headed by men. In a report by Magudulela (2017), women participants identified campus security as alleged perpetrators of GBV. It was also found that the stigma and resulting shame attached to being a survivor of GBV are reinforced by those norms and discourses occurring in societies and institutions (Davids 2020). As an example, the programmes and initiatives which aim to address GBV are often directed at women, or those who have experienced GBV, and therefore places the responsibility of stopping this violence on them, rather than on the perpetrators (Davids 2020).
A third challenge was the application and use of HEI policy framework (Gordin and Collins 2013). At many institutions, GBV falls under the HEI policy framework for sexual harassment and sexual misconduct and neither specifies GBV nor mentions the LGBTQI community. Therefore, although students and staff understand the consequences of sexual harassment, they do not have the same understanding of the consequences of GBV (Davids 2019).
Concerns have been raised in the literature about whether prevention and response programmes adhere to best practices and whether these include the components mandated by government legislation (Bennet et al. 2007). Many South African universities have presented policies and grievance procedures to deal with sexual harassment, but the challenge remains in the application thereof (Bennet et al. 2007). In a 2016 report published by the Rhodes University Sexual Violence Task Team (SVTT), it was found that there was a lack of clarity concerning the mandate of each role player involved in preventing and responding to GBV at the particular university (Abraham et al. 2013).
Two participants highlighted the level of commitment of university role players in creating awareness of GBV is a strength. Though the current pandemic has challenged the implementation of GBV initiatives, three participants reported that this challenge had inadvertently contributed to the strengthening of alternative information platforms, such as online channels. Two participants reported that COVID restrictions has resulted in increased visibility of GBV awareness campaigns on social media. Three universities noted as a strength the multiple ways in which a complaint could be lodged: online system, toll free numbers (24/7) and walk-ins. Two universities reported that their response units allow for a complaint to be made by another person on behalf of the complainant. Two participants noted that case outcomes through disciplinary procedures have been expedited and efficacy of response has been closely monitored. Another participant maintained that the reporting procedure which was often delayed due to the multiple stakeholders involved needed improvement.
Concerns from students about a lack of trust in security response units/structures, as well as a frustration with response time were highlighted as areas of concern. Three participants reported the use of a case manager to coordinate a complaint across the various units, as effective. According to three participants confusion reigned among students as to which office to approach first. All three participants confirmed that a GBV Response Structure Protocol existed and was circulated to staff and students. Two of the participants who were members of the response team at their institutions reported frustrations with students' failure to readinformation provided to them via numerous communication platforms. Challenges in implementation were reported both by student representatives and the institutional GBV task/response team. The need for programme evaluation and monitoring was highlighted by participants. Another challenge, pertained to the lack of resources, mostly insufficient workforce. The response teams were reportedly over-burdened, which also contributed to ineffective coordination and longer response times.
Two participants reported that bridging the gap between policy and practice is a challenge. According to three participants, GBV policies were made available to students on various platforms, for example all first year students were provided with the policy. A concern expressed by two participants, representing response/task teams, was the failure of students to access this information. Three participants confirmed the use of a variety of platforms for distributing information on GBV. Two participants noted that since online reporting tools were introduced, the number of reported incidents have increased.
DISCUSSION
The Discussion that follows is based on a : (i) a rapid review of the literature, (ii) review of policy frameworks, and (iii) qualitative interviews.
An increase in the incidence of GBV at HEIs is a concern.Given the consequences of GBV, long-term interventions are crucial in addressing GBV at HEIs. There is an urgent need to clearly define GBV and to mention it explicitly in policy documents.
The dearth of research on GBV at HEIs links to the lack of evidence on effective prevention and response interventions at HEIs in South Africa. Information from the literature highlights the many challenges that remain in the prevention and response to GBV at HEIs, such as the lack of clarity on what defines an incident the lack of awareness of GBV policy, reporting structures, and the presence and function of support offices. It could be argued that the ability of HEIs to create a safe environment and violence-free community is dependent on the availability of comprehensive and relevant GBV policies, whether staff and students are aware of what legislation applies, whether they acknowledge GBV to be a problem at HEI sand society at large, what their understanding of GBV is, and whether they are aware of and understand the impact of their own gender constructions. Addressing this challenge requires parallel implementation of both prevention and response, including appropriate training for both staff and students.
The platforms used to communicate both preventative and response initiatives need to be evaluated on a systematic basis to assess whether dissemination is effective and far-reaching, and whether accessibility is reasonable, fair and inclusive.
Response strategies should involve multi-sectoral and multi-level interventions. Challenges highlighted by HEIs include the lack of trust in the response and action plan of the response, uncertainty with regards to the relevant sectors for reporting incidents, as well as insufficient information about GBV is. When GBV is normalised or tolerated and not addressed adequately by HEIs it promotes perceptions about a corrupt culture lacking in transparency, accountability, inclusivity and responsibility.
CONCLUSION
This study sought to explore the existence and content of GBV programmes at HEIs in South Africa with medical campuses. The findings provide an evidence-informed framework of the key factors for GBV programmes to be locally relevant, inclusive and person-centred. The rapid review and qualitative interviews report on challenges and strengths of existing programmes. Literature on GBV at HEIs is scarce and the qualitative data may not be a comprehensive representation given that just over a half of HEIs with medical campuses participated.
This study is intended to provide a baseline for further research evaluating current GBV programmes at HEIs with medical campuses, which may inform the development of an evidence-informed framework of the key ingredients for effective GBV programmes.
REFERENCES
Abrahams, N., S. Mathews, L. J. Martin, C. Lombard, and R. Jewkes. 2013. "Intimate Partner Femicide in South Africa in 1999 and 2009." PLoS Med 10(4): e1001412. [ Links ]
Bennett, J., A. Gouws, A. Kritzinger, M. Hames, and C. Tidimane. 2007. "'Gender is Over': Researching the Implementation of Sexual Harassment Policies in Southern African Higher Education." Feminist AfricA 8(September): 83-104. [ Links ]
Braine, J. D., C. Bless, and P. M. Fox. 1995. "How do students perceive sexual harassment? An investigation on the University of Natal, Pietermaritzburg campus." South African Journal of Psychology 25(3): 140-149. [ Links ]
Butler, J. 1999. Gender Trouble: Feminism and the Subversion of Identity. New York: Routledge. [ Links ]
Calvete, E., S. Corral, and A. Estévez. 2007. "Cognitive and coping mechanisms in the interplay between intimate partner violence and depression." Anxiety, Stress & Coping: An International Journal 20(4): 369-382. [ Links ]
Clowes, L., T. Shefer, E. Fouten, T. Vergnani, and J. Jacobs. 2009. "Coercive sexual practices and gender-based violence on a university campus." Agenda 23(80): 22-32. [ Links ]
Creswell, J. W. 2007. Qualitative inquiry and research design: Choosing among five approaches. 2nd Edition. Thousand Oaks, CA: Sage. [ Links ]
Cruz, A. and S. Klinger. 2011. Gender-based violence in the world of work: Overview and selected annotated bibliography. ILO Working Paper 3 / 2011. [ Links ]
Davids, N. 2019. "The consequences of increasing student alienation in higher education institutions." BrieflySpeaking No. 9. Council on Higher Education. [ Links ]
Davids, N. 2020. "Reconceiving a World Around Our Bodies: Universities, Gender-Based Violence, and Social Justice." In University Education, Controversy and Democratic Citizenship, 13-30. Palgrave Macmillan, Cham. [ Links ]
Decker, M. R., A. D. Latimore, S. Yasutake, M. Haviland, S. Ahmed, R. W. Blum, F. Sonestein, et al. 2015. "Gender-based violence against adolescent and young adult women in low- and middle-income countries." Journal for Adolescence Health 56(2):188-196. [ Links ]
DiCicco-Bloom, B. and B.F. Crabtree. 2006. "The qualitative research interview." Medical Education 40: 314-321. doi:10.1111/j.1365-2929.2006.02418.x. [ Links ]
Gordon, S. F. and A. Collins. 2013. "'We face rape. We face all things': Understandings of gender-based violence amongst female students at a South African university." African Safety Promotion: A Journal of Injury and Violence Prevention 11(2): 93-106. [ Links ]
Gouws, A. and A. Kritzinger. 2007. "Dealing with sexual harassment at institutions of higher learning: Policy implementation of a South African university." South African Journal of Higher Education 21(1): 68-84. https://doi.org/10.1080/10615800701628850. [ Links ]
ILO. 2012. Discrimination at work on the basis of sexual orientation and gender identity. Results of the ILO's PRIDE Project. [ Links ]
Isaacs, D. H. 2016. "Social representations of intimate partner violence in the South African media." South African Journal of Psychology 46(4): 491-503. [ Links ]
Joubert, P., C. van Wyk, and S. Rothmann. 2011. "The effectiveness of sexual harassment policies and procedures at higher education institutions in South Africa." SA Journal of Human Resource Management / SA Tydskrif Vir Menslikehulpbronnebestuur 9(1): Art. #310. doi:10.4102/sajhrm.v9i1.310. [ Links ]
Machisa, Mercilene, Rachel Jewkes, Colleen Lowe Morna. and Kubi Rama. 2011. The War at Home: The Gauteng GBV indicators research study. Genderlinks, and Gender and Health Research Unit, South African Medical Research Council, Johannesburg. [ Links ]
Magudulela, N. 2017. "Tackling sexual and gender-based violence on campus: An intervention at the Durban University of Technology." Agenda 31(2): 99-108. [ Links ]
Mahlori, X. F., D. C. Byrne, and L. A. Mabude. 2018. "Perceptions of gender-based violence among university staff: interim results." Sage open 8(3): 2158244018800163. [ Links ]
Paley, J. 2010. "Qualitative interviewing as measurement." Nursing Philosophy 11(2): 112-126. [ Links ]
Peta, C. 2020. "Achieving Academic Excellence in Africa: A Focus on the Intersection of Sexuality, Gender and Disability in Higher Education." In Inclusion as Social Justice, 368-387. Brill Sense. [ Links ]
Rothmann, S., P. Joubert, and C. van Wyk. 2011. "The effectiveness of sexual harassment policies and procedures at higher education institutions in South Africa." SA Journal of Human Resource Management 9(1): 1-10. [ Links ]
Saferspaces. n.d. "Gender-Based Violence at Higher Education Institutions in South Africa." https://www.saferspaces.org.za/understand/entry/gender-based-violence-at-highereducation-institutions-in-south-africa1. [ Links ]
SA news.gov.za. 2018. Policy on gender-based violence at higher education institutions pending. https://www.sanews.gov.za/south-africa/policy-gender-based-violence-higher-education-institutions-pending. [ Links ]
Sandelowski, M. 2000. "Focus on research methods: Whatever happened to qualitative description?" Research in Nursing & Health 23: 334-340. [ Links ]
Singh, S., B. Mabaso, R. Mudaly, and A. S. Pillay. 2016. "Policy for prevention of sexual assault on campus: Higher education students' perspectives." Alternation Journal 23(1): 113-134. [ Links ]
Sixsmith, J. and J. Daniels. 2011. Action research. Qualitative methods in psychology: A research guide. 2nd Edition. Maidenhead: Open University Press/McGraw Hill. [ Links ]
Sloand, E., C. Killion, F. A. Gary, B. Dennis, N. Glass, M. Hassan, D. W. Campbell, et al. 2015. "Barriers and facilitators to engaging communities in gender-based violence prevention following a natural disaster." Journal of Health Care Poor Underserved 26(4): 1377-1390. [ Links ]
Street, A. E. and I. Arias. 2001. "Psychological abuse and posttraumatic stress disorder in battered women: Examining the roles of shame and guilt." Violence and victims 16(1): 65-78. [ Links ]
United Nations Economic and Social Affairs. 2015. The World's Women 2015, Trends and Statistics, 159. [ Links ]
Violence against women Prevalence Estimates. 2018. Global, regional and national prevalence estimates for intimate partner violence against women and global and regional prevalence estimates for non-partner sexual violence against women. WHO: Geneva, 2021. [ Links ]
WHO see World Health Organization. [ Links ]
World Health Organization. 2013. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. Department of Reproductive Health and Research, London School of Hygiene and Tropical Medicine, South African Medical Research Council. [ Links ]
World Health Organisation. 2020. Levels of domestic violence increase globally, including in the Region, as COVID-19 pandemic escalates. Regional Office for the Eastern Mediterranean. [ Links ]


{kind=link}
{kind=link}
{kind=link}