










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Higher Education
versão On-line ISSN 1753-5913
S. Afr. J. High. Educ. vol.37 no.1 Stellenbosch Mar. 2023
http://dx.doi.org/10.20853/37-1-5678
SPECIAL SECTION
Negotiating boundaries: framing and sense-making in a design thinking project with an elderly community
D. MinnéI; N. ConradII; T. S. DouglasIII; T. MutsvangwaIV
IApplied Microbial & Health Biotechnology Institute Health & Wellness Sciences, Cape Peninsula University of Technology, Cape Town, South Africa. https://orcid.org/0000-0002-1243-1495
IIDivision of Biomedical Engineering, Department of Human Biology, University of Cape Town: Health Sciences Campus, Cape Town, South Africa. https://orcid.org/0000-0001-5186-8641
IIIDivision of Biomedical Engineering, Department of Human Biology, University of Cape Town: Health Sciences Campus, Cape Town, South Africa. Deceased. https://orcid.org/0000-0003-2024-4179
IVDivision of Biomedical Engineering, Department of Human Biology, University of Cape Town: Health Sciences Campus, Cape Town, South Africa. https://orcid.org/0000-0003-1210-2832
ABSTRACT
In recent years Design Thinking has established itself as a popular methodology for unlocking the creative potential that drives innovation, and scholars have begun to apply it in the health sector. However, as a conceptual framework, the approach has been criticised for lacking coherence and empirical validation. Although few have explicitly highlighted the central role of frame management in Design Thinking, we propose that much of the innovative potential, as outlined in its founding principles, stems from a concern with mental processes that contextualise new information to give it meaning and significance. Here we sought to address this gap by studying the framing process in two design teams tasked with developing solutions to assist an elderly population with compliance with medication schedules. Findings from a qualitative analysis indicate that although Design Thinking has clear merit as a methodology for helping designers shift beyond their immediate field of expertise, feedback and observations gathered during engagement with stakeholders inevitably appear to make their way through a filtering process where specific interpretations and meanings become censored and constrained by dominant discourses. Especially in the health sector, where information is sensitive, critical attention to the underlying value systems and prevailing discourses that influence designers' implicit frames of reference is needed if Design Thinking is to gain credibility as a scientifically robust method for innovation.
Keywords: design thinking, framing, health innovation, medication adherence
INTRODUCTION
Design is never neutral. It represents a process of selection where elements are ranked and arranged in strategic ways to create new meanings and patterns that aim to serve a purpose, and for this reason, make "sense" in the lives of specific individuals. Buchanan (1992, 8) argues that "There is no area of contemporary life where design is not a significant factor in shaping human experience". Design can therefore be a powerful tool for change. However, because "sense-making" (Kolko 2010) follows from predictions that emerge from what we already know, the innovation that designers strive for, that is, the capture or creation of value in entirely original ways, can quickly be stifled. This is a central paradox in design. How can we secure novel outcomes that make sense if we are not guided by certainty? This conundrum is amplified when designing for social innovation where designers must grapple with ill-defined or "wicked" problems (Rittel and Weber 1973), which are difficult to conceptualise because they are embedded within complex social and cultural systems. In the healthcare setting, an intimate space in which individuals may be at their most vulnerable, appropriate, evidence-based design of health programmes is a great challenge. This poses a major barrier to care in the South African context, a multicultural setting where historical and structural patterns of healthcare inequality persist (Bell et al. 2022).
DESIGN THINKING
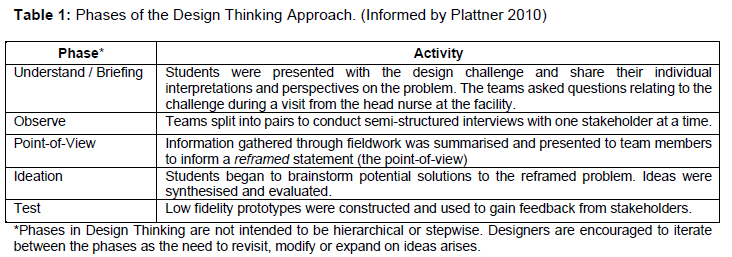
In recent years, a methodology referred to as Design Thinking has gained recognition as a solution to the conundrum of designing from experience. Originating from the fields of ergonomics and computer science, design thinking describes a method for designing sustainable and innovative products or programmes, aiming to acknowledge the meaning and experience that a solution should offer its beneficiaries (Brown 2008; Giacomin 2014). In Design Thinking, teams typically iterate between 5 phases of the design process in which they (1) unpack initial understandings of a challenging brief, (2) undertake activities to explore the problem space through observation, and (3) develop a point-of-view that defines the problem statement from the user's perspective, (4) ideate to develop potential solutions, (5), and prototype to test candidate solutions.
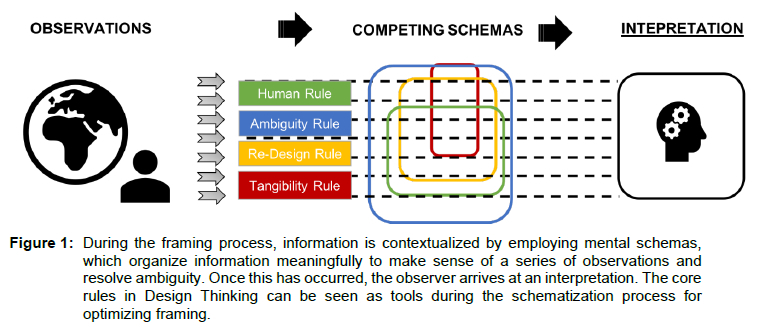
This approach rests on four core principles: the human rule, the ambiguity rule, the redesign rule and the tangibility rule (Plattner, Meiner, and Leifer 2011). Although not all scholars refer to these principles as rules, they are nonetheless discussed as core aspects of the method (Bjögvinsson, Ehn, and Hillgren 2012; Brown and Katz 2011; Holloway 2009). The human rule is a foundational principle of design thinking and maintains that all design activities are social in nature. Designers are influenced by culture and society, and they design for the benefit of society. This requires, first and foremost, a deep level of empathy, where empathy is understood as the ability to understand and respond appropriately to the emotional circumstances of another individual (Decety and Jackson 2004; Batson, Fultz, and Schoenrade 1987).
The second rule, the ambiguity rule, aims to promote tolerance for ambiguity during the design process, encouraging designers to experiment with ideas and scenarios beyond the limits of their existing knowledge and skill sets (Plattner et al. 2011). It is believed that by allowing space for uncertainties that tend to arise in novel and unpredictable contexts, the reliance on fixed schemas, that is, mental shortcuts or tunnel vision, might be circumvented so that new understandings of the problem can emerge (Considine 2012; Rassin et al. 2008).
The re-design rule recognises that design initiatives are embedded in ongoing attempts by society to address longstanding problems. Though the challenges are seldom new, technology and social circumstances evolve, giving way to opportunities for innovation. The re-design rule urges designers to delve into the history of problems to gain insight into the conditions that might hinder or support future attempts at solving them. Finally, the tangibility rule emphasizes making ideas tangible through the construction of models or prototypes in the belief that tangibility opens up and animates lines of communication that may otherwise lie dormant if thoughts are restrained to the verbal modality.
The innovation potential of Design Thinking has been recognised by several scholars and organisations (Bell 2008; Brown 2009; Leavy 2010; Martin 2010; Neumeier 2009). Some of the reluctance to embrace the intuitive mindset that Design Thinking encourages (Lindegaard and Wesselius 2018) may stem from the fact that, as a collection of toolkits and "how-to" resources freely available to the public (for example, IDEO 2019), there appears to be less critical scrutiny at a theoretical and conceptual level regarding the kinds of cognitive processes that the method tries to unlock (Badke-Schaub, Roozenburg, and Cardoso 2010; Carlgren, Rauth, and Elmquist 2016). Carlgren et al. (2016) have noted that among key proponents, main concepts are not always defined and when they are, too often, superficial or popular descriptions are used. As a result, coherence in Design Thinking and a clear articulation of the conceptual framework is lacking. Others have argued that in the academic literature, there is little substantive critical discussion of the concept of Design Thinking, and in practice, it differs in meaning depending on the context (Hassi and Laakso 2011; Johansson-Sköldberg, Woodilla and Çetinkaya 2013). Under such circumstances, the approach can easily be regarded as hype or a fad (Johansson and Woodilla 2010), unsubstantiated by scientific rigour, implying that it is unlikely to endure as a practice that is taught in academic or more formal training institutions (Lindegaard and Wesselius 2018).
We offer a perspective that may contribute towards the theoretical understanding of Design Thinking. Although seldom explicitly articulated, the tremendous innovative potential in Design Thinking, which is to appreciate problems in entirely new ways, stems from a central concern with the issue of framing (Dorst 2015). In other words, if we unpack the four core principles of Design Thinking, each describes a strategy to achieve new frames of reference that help designers break out of the mental schemas that restrain novel interpretations and constructions of meaning in problem settings. Engagement with framing as an underlying concept will encourage practitioners to reflect on their process critically.
FRAMING IN DESIGN THINKING
Framing can be understood as a tool that the mind implicitly employs to contextualise information to reduce ambiguity (Goffman 1974). By connecting new information to what is already known, framing functions as an interpretative lens enabling vague, intangible facts to become meaningful. Existing mental schemas and theoretical perspectives operate here much like rules or algorithms for filtering incoming information so that it can be "packaged" and represented mentally in ways that make sense. Framing is not very different from what it means to understand and is central to the sense-making process (Kolko 2010). The problem is that we do it unconsciously (Bacchi 2009; McElroy and Conrad 2009), often not mindful that meaning is subjective. By mentally filtering out "irrelevant" facts that do not conform to the particular schema out of which the situation is interpreted, other ways of understanding may be lost. Too often, implicit perceptions of relevance are constrained by prevailing discourses linked to authorities on various bodies of knowledge and practices (Foucault 1980) such as those linked to science and medicine, implying that dominant ideals and frames of interpretation are continuously reproduced. As illustrated in Figure 1, Design Thinking tries to address this phenomenon.
As a core principle of the methodology, the human rule places emphasis on empathy, which encourages designers to detach from their own frames of reference continually and view a situation from the vantage point of the intended user (Gasparini 2015; Kolko 2015). Focussing on the user interrupts the natural tendency to revert to a designer's educational and theoretical frame of reference. Based on a theory of mind (Premack and Woodruff 1978), Kim and Ryu (2014) adopt the term the "simulated-self" to describe this mode of processing, in which a designer uses the self as a proxy for sensing the user's inner, private world. Deriving from this simulated version of the user's relationship to the problem, a new set of predictions regarding outcomes can unfold. This capacity for shared representation thus enables a window into another person's world.
The human-centred approach of Design Thinking is not only directed at fostering empathic insight but calls for closer appreciation of subjective experiences and meanings that characterise users' attitudes toward a problem or solution. Unlike other schools where aesthetics or technology drive the design process, Design Thinking is concerned with user needs. This entails exploring human emotions and motivation - what it feels like to interact with a product and what underpins the user's interest in it. This focus can be seen as a type of reference frame. According to Dorst (2015), a deeper understanding of human needs and the meanings associated with a particular set of problems in the wider context of personal lives, enables the development of new meaningful perspectives without straying from the fundamentals. Purely rational explanations of problems - explanations that appeal to logic or reason - often fall short of accounting for why people behave and act in the ways they do (Kahneman, Knetsch, and Thaler 1991). Self-Determination Theory, which looks beyond "logic", has been recognised as an essential framework for understanding health and wellbeing (Deci and Ryan 2008). It proposes that individuals harbour the natural, innate tendency to develop and maintain a unified sense of self or identity. This necessarily involves the propensity to seek out opportunities for autonomy and self-regulation and meaningful interaction with others (Deci and Ryan 2002). These human needs are often overlooked in healthcare. For example, Bracken (2002) argues that healthcare has become disproportionately influenced by the dominant logic of medical science, which has sought to translate human suffering and misery into the technical nomenclature of medicine, making it amenable to corrective medical interventions by clinicians. In this way, efforts to ameliorate suffering can escape the inherent intangibility of the psyche and instead places the control of human pain in the rational, expert hands of a medical professional (Davis 2010). The perception of pain in others is contained and made tolerable in this way. If health practitioners and designers do not consider underlying psychological needs for social connection and identity, medical advice that ignores these sources of intrinsic motivation, or circumvents opportunity for their realisation, is less likely to succeed. The human rule of Design Thinking can be viewed as highlighting this humanistic frame of reference when defining the problem space so that new "products" can integrate seamlessly with wider underlying value systems (Dorst 2015).
Framing is similarly embedded in the ambiguity rule. The ambiguity rule is designed to interrupt the automatic tendency to employ dominant mental schemas for making sense of a vague or perplexing situation. In this way, it could be thought of as encouraging reflexivity, which is a practice understood as the process of applying critical attention to the kinds of value systems and theories that influence everyday actions and assumptions (Finlay and Gough 2008). Design thinkers should be aware that ideas that challenge established norms and professional dogmas are often the ones that deliver more radical change (Leifer and Steinert, 2011). Nevertheless, many studies show that intuitive heuristics strongly influence decisionmaking (De Martino et al. 2006; Kahneman and Frederick 2007). When faced with a decision under complex circumstances, individuals tend to fall back on standard rules of thumb based on their previous experiences (Gilovich, Griffin, and Kahneman 2002). For instance, creative teams tend to favour analytical approaches grounded in rational or face-value models of human thought and behaviour because these models carry the illusion of being better suited for dealing with uncertainty. The irony here is that this approach may leave designers unequipped for coping in unfamiliar contexts and, at times, might in fact be counterproductive since it is driven by fear - an aversion to that which is unpredictable - and not by logic because the nature of innovation is that it overcomes problems that are inherently "wicked" and ambiguous. By fostering tolerance for the discomfort of unpredictability in a climate of uncertainty, the ambiguity rule tries to make space for the emergence of new or unanticipated explanations of novel information.
Often, this process requires a switch to non-linguistic modes of sense-making. Because it is difficult to explain in verbal terms the meaningful connections that form the basis of a novel interpretation, the tangibility rule of Design Thinking, which involves rapid and frequent prototyping, offers a means for clarifying, in tangible form, how different aspects and ideas linked to a solution relate to each other to form a meaningful whole. Mainstream theories of knowledge assume that conceptual representations, categorical knowledge or knowledge about relationships, reside in a specialised semantic module of the brain, separate from other systems for perception, action and inference (Smith and Medin 1981). However, in more recent times, this has been viewed as problematic, and many scholars now believe that conceptual knowledge is perceived and understood through embodied interactions with the world. In other words, the way the human mind understands meaning in abstract ideas takes the form of re-enactments of sensory and motor simulations (Barsalou 2003; Clark 1998; Lakoff and Johnson 1980). For example, the concept of distance is grasped by simulations of walking within the brain (Witt and Proffitt 2008). By "acting through" ideas with prototypes, the tangibility rule takes advantage of the way in which the human mind constructs conceptual knowledge through interaction. Solutions become perceptible through the lens of the body and its actions. Lindegaard and Wesselius (2018, 91) suggest that because "explicit moves always occur in relation to an implicit 'sense of fit' or 'feeling for' a solution ... material design practices such as sketching and prototyping may assist this 'feeling for', particularly in collaborative situations". Finally, the re-design rule frames the design challenge within its historical context to provide a socially shared representation of a problem that may not be immediately apparent in the present (Liu and Hilton 2005). By doing so, norms and values within which the problem has been associated, and the roots of present-day constraints, can be traced (Wright 1996). A historical perspective on a design challenge can influence how current problems are interpreted, providing richer framing.
Thus, to summarise this section, the techniques and principles that characterise Design Thinking as a methodology appear to be firmly rooted in the notion of framing. Indeed, the negotiation of shared frames forms a core activity of design teams (Whelton 2004). Dorst's (2015) seminal work on frame innovation in Design Thinking explores this topic. It emphasises the critical role that "reframing" of a problem serves before professional designers can develop viable solutions and interventions. Although several authors have written about framing as a design concept (Dorst 2015; Van Leeuwen et al. 2016), few have explicitly highlighted and critically examined the central role of frame management in the Design Thinking approach. Empirical studies are needed if Design Thinking is to persevere as a scientifically robust approach to innovation.
Here, we sought to address this gap by studying the process of framing in two design teams newly acquainted with the Design Thinking method. Using various qualitative methods, we aimed to explore the influence of Design Thinking principles on framing. We sought to identify the types of frames adopted by the teams at various phases of the process and to explore not only why specific frames were favoured but also, what the various consequences of framing might be for design outcomes.
METHODS
This research followed a design challenge carried out by students taking the master's-level Health Innovation and Design course at the University of Cape Town, South Africa. The course introduces students to the principles of Design Thinking as a way of developing sustainable solutions to health and wellbeing in the South African context. This approach is grounded in the ethos of "engaged scholarship" (Sandmann 2009) and aims to align academic activities with real-life outcomes that serve community development. The course implementation described here was in partnership with a non-profit organisation in Cape Town that assists pensioners with the provision of communal housing, primary healthcare, small enterprise opportunities and social support so that they can remain active, independent members of their community. The facility staff put forward a challenge brief relating to medication non-adherence in their community members. The problem statement was as follows: "Redesign ways to improve adherence to chronic medication in the elderly, as older persons are overwhelmed by changes in their health".
Students were partitioned into two design teams with 6 members in each group. Group 1 consisted of 3 women and 3 men, 3 South Africans and members from Zimbabwe, Netherlands, and Canada. Group 2 comprised 2 women, and 4 men, of which 3 were South African and the rest were from Ghana, Uganda and Kenya. Students came from a diversity of academic backgrounds related to health, geography, science or engineering. The Design Thinking process followed by the teams is outlined in Table 1.
A single researcher collected data. Observational methods were employed throughout the project to gain insight into the framing process. Data were also gathered more formally using open-ended qualitative interviews with students (n = 12), residents of the facility (n = 8) and facility staff members (n=4). These interviews lasted between 50 and 80 minutes, and they centred on experiences of the project, engagement process, views on medication adherence and life at the residence, and other related insights. Students were further invited to fill in a series of short online surveys distributed on three occasions during the project with open-ended questions relating to their impressions of the facility, their perspectives on the information gathered from stakeholders, and their experiences of the Design Thinking process.
Interviews were recorded and transcribed for later processing. All participants of this research gave informed consent before offering information. Anonymity and confidentiality were upheld at all times, and participants were reminded of their rights to withdraw from the study at no personal cost. Ethical clearance for this research was granted by the Human Research Ethics Council of the University of Cape Town (HREC/REF: 554/2015).
Raw data was uploaded to NVivo 12, a qualitative data analysis software package. Raw data was coded and grouped into thematic categories. The analysis was guided by the principles of Grounded Theory (Strauss and Corbin 1990), which is an inductive approach that enables themes and elements to emerge from the data and coalesce into concepts and categories that form the basis of theoretically meaningful explanations. Based on its emphasis on experiences and meaning-making, this approach was complemented by Interpretative Phenomenological Analysis (Smith and Osborne 2003) to maintain focus on how participants make sense of a particular phenomenon in a given context.
FINDINGS AND DISCUSSION
In the following section, results are synthesised and discussed about the first two rules of the Design Thinking approach - the human rule and the ambiguity rule. Because our methods were most appropriate to investigating these first two rules, our analysis precluded the re-design and tangibility rules. This decision was also made to limit the scope of our inquiry to ensure an appropriate level of depth in our discussion. In the following sections, we unpack the various forms of framing that emerged during data collection and reflect on their respective relationships to the core principles underlying the human and ambiguity rules.
The human rule
The human rule fosters an engagement style that tries to uncover the emotional and contextual meanings that a user attaches to the design problem and its proposed solution. It encourages designers to adopt the user's unique point of view. We therefore looked for themes emerging from the framing process that relate to these facets of the human rule.
Both design teams showed signs of perspective-taking. To begin with, the majority of student participants mentioned that prior to stakeholder interviews, they assumed that the best solution to the problem of medication compliance would involve a technological intervention, in the form of an automated mobile phone application to remind residents to take their medication or a device for monitoring adherence. Both teams were hastily dissuaded of a technology-based solution after gathering user-feedback. Group 1 developed an idea called "Adherence Heroes", which centred on a programme of recognition to reward residents for adhering to their medication schedules, and for providing social support to fellow community members to do the same. Recognition was delivered by posting photographs of the monthly "heroes" in the community centre in frames designed to mimic television sets, in this way drawing on the residents' shared love for local soap operas. Group 2 designed a calendar system called "Medi-cal", where residents would be able to list their medications and record whether or not they took them as prescribed. This system was based on the need for establishing a system whereby staff could monitor and track medication adherence. Both teams recognised that the lives of residents were not technologically oriented. It was not simply that many residents did not own a smart device but that assistive technology did not offer meaning to the community. Their preferred daily activities were, in fact largely devoid of technology.
Thus, perspective taking did occur, but it was often limited to physical and not mental or emotional frames of reference. To illustrate, one team member offered:
"The main aspects that were focused on were the physical limitations of the elderly."
This trend occurred against a subtle backdrop of the medicalisation of old-age, where medicalisation is understood as the phenomenon by which everyday human or "life" problems are framed and treated in terms of medical problems (Conrad 2007). Questions to students about hardships faced by residents were answered in large part with reference to the absence of medically-related complications. For example, life was deemed to be pleasant in large part because most residents were in relatively good health and the facility provided community members with regular medical check-ups, ongoing supervision by nursing staff, and with a system that circumvented the need to wait in lengthy queues at government health facilities to fill out prescriptions. Furthermore, feedback from medical staff regarding the residents' needs was prioritised over feedback from the residents themselves. There was little reference, for example, to family and the fact that many residents had scarce contact with their loved ones.
Understanding the elderly from this perspective is not uncommon or surprising. Vincent (2006) argues that in modern Western societies, the understanding of aging is framed by science. The ability of science to prolong life and intervene in common pathologies of old-age has unnaturalised the aging process, positioning the aged body in a state of disorder, as having distinct pathology requiring medical intervention, and ultimately, as "dying" (Cole 1992; Katz 1996).
Here, the medicalisation of aging was more nuanced. In particular, painful experiences were acknowledged but largely through the lens of medicine, that is, physical pain. Both teams discussed unpleasant side effects as a major determinant of medication non-compliance. In contrast, there was considerable hesitancy to frame adherence in relation to emotional or psychological meaning. Instead, the problem of medication non-compliance was explained in rational terms as a problem of structural or environmental constraints and factors:
"The problem revolves around medication and adherence, and the thinking was to understand the entire medication process from prescription to government procurement to medication consumption and everything in between."
"A reason I encountered was them not having the correct preparations to take the medication. This may be them not having eaten on time or not having any water with them to take the medication. Having not met the right conditions, the residents seemed to write off taking that particular medication for the day."
Or as a problem related to education or lack of awareness about health outcomes:
"Maybe they don't realise the importance of taking it consistently. Because if you have a condition, once the symptoms fade, then it's like the importance of taking the medication will also fade."
"I think they mentioned side effects. ... initially we had like a pamphlet type of solution." "Adherence heroes was trying to address the issue of misinformation
There were signs too, of the implicit assumption (particularly by students with an engineering background) that the solution would require technical knowledge because the problem is a practical one, not a social-emotional one:
"I found the contributions of people from non-engineering backgrounds useful even if they may not be able to implement the solution."
In contrast, feedback during interviews with the residents revealed that difficulties with medication adherence were complex and multidimensional, involving both "rational" accounts like concern over imagined side-effects but also more personal or psychological reasons relating to motivation, the assertion of autonomy, and a desire to be treated for pain in other more traditional or humanised ways. For example, several residents spoke about their preferences for remedies that have been passed down to family generations ("Grandmother's remedy") - therapies that involve applying certain soothing oils or heat packs to the skin that evoked experiences of care. They expressed frustration that doctors disregarded their requests for alternative treatments and instead always prescribed pharmaceuticals, even though these were upsetting to the stomach. A number of residents expressed the belief that non-compliance often had to do with giving-up, and a loss of motivation to live on. Others spoke about the struggle for independence and autonomy in the communal living environment and how instructions from staff members to take medication can be experienced as a battle of wills:
"And then also encouragement can be seen as being bossy, or 'you watching me', or 'you are not my policeman', you know, like policing someone else. Don't tell me what to do."
"It's just an attitude of 'I will do what I like to do and if I don't get time to do it I'm not going to do it' .... 'There is nothing wrong with me so you know."
"And then there is putting authority over another person, telling others what to do."
For the student designers, medical discourse might thus have contributed in part to the silencing of other psychological factors that would have explained an additional side to the problem of medication adherence. Medicalisation might, as such, be seen as a device that compartmentalises human suffering (Bracken 2002) to make perceptions of pain manageable. Nevertheless, topics surrounding emotional suffering and engagement with painful feelings was difficult for the students. A strong theme emerged instead around the notion of wellbeing. The facility was largely described as a place of security, happiness, social connection and rest. Despite the acknowledgement of evidence to contradict or complicate this view, designers maintained the opinion that the facility was, almost unequivocally, a place of well-being and happiness.
"... when I got there, it seemed like it's a very happy living environment and residents are proud of their home, .... They seemed very content in their home .... But I think from their point of view, they have been through the hardships. Maybe a lot worse their whole lives, and I just think that they don't see it in that sense. They still feel that they are happy to live at a very good price in a safe home."
Interviewer: "And did anything come to light that was a particular challenge about being part of the community?"
Interviewee: "No. Not anything like that ... There's nothing that stood out for me."
Interviewer: "Okay. So there wasn't ... Nobody spoke about difficulties, whether it was about the people or just life struggles?"
Interviewee: "No. No. If anything, they help each other."
"I sensed fear amongst the residents - the rules with regard to losing your residency .... Like people tip-toe around staff especially. ... It's like they feel like at any moment you can be asked to leave .... But I felt like they were happy. They felt relieved ... they've been stressing their whole lives, they didn't know how they would survive without [the facility]. So like they're really happy to be there."
Evidence that contradicted the ideal of the facility as a place of harmony and wellbeing was not tolerated well. We see here that when this frame was challenged, the idealised version of residency took precedence. Experiences and meanings related to suffering were subsequently not well incorporated into solution prototypes. For instance, both design teams were aware that interpersonal conflict in the communal homes was a major source of distress for residents. Still, it did not register as a meaningful topic for the design task. This theme, however, emerged in almost all interviews with residents and staff. Conflict in the residence was described as a problem with repercussions for many other aspects of life - it was felt to underlie frustration levels and rising blood pressure, to explain why certain individuals would not participate in social activities, why many residents often confined themselves to their bedrooms, and why some may go to lengthy measures to reclaim their sense of dignity and autonomy. Some residents even believed that conflict explained why residents would at times fail to take their medication - if meals were skipped to avoid encountering a housemate in the kitchen, certain pills that require a full stomach before being ingested would not be taken.
For the students, the immense gratitude that almost all residents expressed at being at the facility appeared to prevail over meaningful acknowledgement of residents' dissatisfaction.
"The hardship has nothing to do with [the facility], but life ... growing old, and to some extent the habits some of them were used to before ... excessive drinking and smoking. But I think [the facility] has done a fantastic job to help these aged people find some comfort and an enjoyable life before they depart."
"... they didn't know how they would survive without [the facility] ... they are happy to be there, you know."
When suffering is present, its acknowledgement is a central component of empathising. The idealisation of life at the facility suggests that students struggled to some degree with the human rule of Design Thinking if it meant acknowledging and exploring pain. Often though, people will try to conceal pain. Dorst (2015) maintains that in complex design challenges, the root of the problem usually relates to human interpersonal emotions and values. Because these themes are deeply personal, they are often not always apparent on the surface. Even so, student participants were, in fact astute at perceiving when residents began to feel discomfort with certain sensitive topics.
"I found myself making sure that the interviewee knew I was listening but would try and steer the next question towards a more comfortable area of reflection."
"We did not probe her to expand further on personal issues which we could sense was a touchy subject for her. We turned the conversation to another subject."
Thus, a dominant frame to emerge out of the student accounts was that health and its ramifications are deeply private affairs to be navigated with great sensitivity, or at times, not at all. This frame functioned as a gatekeeper, but it appears to have arisen, paradoxically, in response to a strong commitment towards the human rule, which urges designers to prioritise the user's perspective and needs without interference by their preconceptions and technical knowledge. In other words, out of respect for the stakeholders, the human rule appears to have encouraged designers to not dig too deep, to take things at face-value and to refrain from "decoding" feedback.
"The biggest challenge was making sure we didn't overstep any boundaries especially since we were engaging in health issues. We wanted to make sure that the interviewee had a chance to share openly because we had no idea how they would react to questions, even though they volunteered."
In their studies of class depictions in the popular media, Streib, Ayala, and Wixted (2017) argue that meta-frames that erase or sanitise poverty and inequality function to downplay the suffering these groups experience. These frames, in turn alleviate a sense of burden or responsibility in more affluent groups (Bullock, Wyche, and Williams 2001). Here, however, there are signs of a different trend. Students showed concern about, and acute awareness of, the imbalance of power between the university and the community:
"It's like, obviously knowing we're coming from a university .... They didn't have the opportunities that we have. So, yeah, it's knowing that ... we have a lot more privilege than they do .... "
"There's an issue of the ages ... we look like their children. You wouldn't want to look like you're not taking your medications. So they wouldn't want to admit, like, that it's a problem, I think for 'appearances'. So they won't really want to share that with someone who's so young 'who can be my child'."
"It seems that like most of the residents aren't like particularly highly educated, you know, and so when a bunch of people from the University come, it's like 'Okay cool they gonna fix everything, they know what they are doing .... Because they're coming from the University, then they know what's going on'."
It could be argued that framing the community in terms of suffering and therefore as disadvantaged consolidates their adversity, and in this way may have been experienced by the students as an act that further entrenched the power imbalance. However, the censorship of pain in students' portrayals of life at the facility is problematic for the design process because it decontextualises the problem of medication adherence. This is what the human rule in Design Thinking tries to address. It must be noted, however, that it is possible that in the current cohort of designers, principles of Design Thinking, such as the human rule, were not adequately grasped, which may explain how pain was dealt with. Data gathered from individual interviews showed that conceptions of empathy, for example, differed considerably across student participants. For many, empathy was equated with sympathy. Others held more comprehensive understandings of the term but felt strongly that not every person would be capable of deep empathic engagement, a skill not easily learnt, and certainly, not fostered through instruction. Nonetheless, we see more generally that framing decisions were affected not only by participation from stakeholders, but also by the emotions that the interaction evoked in the designers. When competing interpretations arose and no single frame could do justice to the representation of the situation, acceptable or dominant discourses tended to take precedence. This can effectively reproduce explanations that function to maintain the status quo and is a far cry from the "disruptive innovation" that Design Thinking claims to foster (Bucolo and Matthews 2010).
The ambiguity rule
The ambiguity rule aims to intervene when the desire to make sense of an uncertain situation prevents latent meanings - ways of understanding that are not immediately apparent - from unfolding. The very perception of ambiguity is meaningful in itself; it signals competing explanations. As we discussed above, because observations of suffering put into conflict with the authority of the frame depicting the facility as a place of wellness, the full range of meanings related to the problem of medication adherence was compromised. This suggests that ambiguity was not tolerated well, and, like the human rule, the ambiguity rule comes under threat if certain aspects of human experience are flagged as off-limits.
Interestingly, the process of allowing space for new ideas to gradually and organically emerge was perceived by some as lacking the rigour of more traditional technical design approaches, like those linked to engineering: "I won't say it makes you lazy ... but it makes it easier, in a way, to just like think, you know."
It appears that value was attached to the ambiguity rule. It changed the experience of the learning process. Other members, for example, found it invigorating:
"But yeah, that's kind of like being uncertain about where this is going, and so of treating it like an adventure and so we could figure things out."
However, it became evident that tolerance for ambiguity was closely linked to personality styles. Some team members were described by their peers as being rigid, selective and uncompromising in their interpretations of user feedback and solution ideas:
"... some members are very closed to new or different ideas - they have made up their mind and not willing to change direction."
"I have noticed some class members only wrote down selective impressions, while others transcribed most of what is said. The first group (mostly engineers) distils and boxes the data and the true emotion gets lost when you need to tell the rest of the group about it. The social sciences members focused more on social issues."
"Some members have very set ideas. They felt comfortable with it, made the decision, 'this is what the group will do' and went with that. I spoke up many times but it was not seen as important. I did not get the support of other team members either. I [suggested] a whole new direction/idea after our first [facility] session. The reaction was: 'But that is a whole new idea! ! '"
Working through ambiguity to develop frames that spoke to the complexity of a problem appeared to be a group-level issue. It mattered less that individual team members could grasp the multi-dimensionality of life at the facility; the interpersonal dynamics in team work ultimately determined what frames were deemed acceptable and most appropriate. Although solution prototypes did not capture the depth of the problem of medication adherence, several individuals did recognise the subtle complexities of the situation:
"This is their last resort of resistance where they can make decisions for themselves. It needs to be respected as well."
"Like they don't feel like [they] deserve to continue [living]."
"It's like your faith will heal you ... if you take medications you are doubting your faith."
Therefore, power dynamics operating within design teams appear to have played a role in shaping the sense-making process. Many authors have written about the influence of power on knowledge (Foucault 1980; Giroux 1988; Hooks 1989). Part of the formally accepted definition of power is that those who possess it are thought to have both the authority "to know" and also the right and obligation to define meaning. Studies have found that the knowledge constructed and presented by individuals with more power in work-groups takes precedence and subsequently constrains the scope of knowledge production (Brooks, 1994). Working through ambiguity to reach consensus is a space within the design process that might benefit from specific tool-kits that help give voice to less dominant members.
Interestingly, one of the more puzzling issues that both teams described was how to respond to the consistent feedback from residents and staff that medication adherence was not a widespread problem.
"After the first round of interviews, I said to one of my group members, do you guys really think adherence is a problem and everyone said 'No'.... So that was quite interesting in that no one really could confirm the challenge and so it was almost like, is this a tricky question ...?"
"The assumption is that they are not adhering and their health is deteriorating ... but that wasn't what we found out."
"The staff want to improve medication adherence, but it does not seem to be a problem for the residents. If the residents are not going to 'see' the problem, they will not 'own' it and it cannot be made better."
Design teams were faced with inconsistency - feedback from the residents did not validate the problem brief. This acknowledgment was not ambiguous, but the end goal was uncertain, and the appropriate course of action was unclear. One possible explanation is that the dilemma was resolved by deferring to accepted authorities - the head nurse was strongly invested in the brief, and so Group 1 did not abandon it, but Group 2 re-framed the problem statement to specify the user as the "health worker" instead of the residents.
In Group 1, interviews with designers indicated that ambiguity surrounding the root cause of the problem, what Dorst (2015) refers to as the "archaeology" of the problem, was never felt to be resolved.
"The real problem is that we do not really know. We do not have data to help us understand the situation. We focused on the healthier patients."
"I think everybody had an opportunity where they have to compromise because, yeah, because I think it was just because no one was sure about what would work or where to go."
"I do think the persons' intentions in our team was not wrong. They also cared, but chose a safer option, a blanket approach."
In reality, no single explanation could likely account for the lack of medication adherence. Many published studies report heterogeneity in accounting for why the elderly struggle to comply with medication schedules (Balkrishnan 1998; Gellad, Grenard, and Marcum 2011; MacLaughlin et al. 2005). Possibly, acknowledgement of this heterogeneity evoked a sense of "design paralysis" in both teams, a term that has been used to describe messy experiences when designers are faced with very complex problems and overwhelming demands on decision-making (Schön 1983; Stolterman 2008). Doubt surrounding the problem's root cause may have impinged upon Group 1's willingness or confidence to re-define the brief. This seems to have been compounded by limitations on time (changing the brief after the first round of stakeholder interviews would have meant finding the time to conduct another round of initial interviews), but also as a result of academic conventions, where the freedom to modify assignment or essay questions is not usually tolerated. Team 2, however, changed the brief early on, but not radically, and their approach was strongly influenced by not being able to tell with certainty whether or not residents were compliant.
"I remember in the first conversation with the [nurse] in charge, one of our questions was how they measured adherence, and when we were unpacking it into view with my group, it came up that it doesn't seem as if they actually have a method of measuring the adherence .... I think that guided us throughout the whole process, and then in the end our solution was actually based on that .... because our solution was about measuring the adherence and it was about helping the elderly remember .... So our initial thought was, okay, measure the adherence."
According to several authors, this experience of uncertainty is often dealt with by taking measures to reinstate a sense of control, often by creating simpler, artificial scenarios (Stolterman 2008). Team 2's decision to reframe the end-user, and the problem brief can arguably be interpreted along similar lines. While this strategy may best have addressed the problem space, the specification of the end-user must be made early on in the design process, given that Design Thinking gains its momentum from the needs of users, and re-specifying the user may have significant implications for the wellbeing and empowerment of a target group. Dorst (2015) has offered some guidance on how to reduce complexity when framing becomes ambiguous. By focussing on creating an inventory of interests, values and behaviours that users attribute to the broader context of their lives, instead of purely casual explanations of the problem under study, the identification of shared or underlying themes and meanings can function to define a user-centred problem space.
CONCLUDING REMARKS
The innovative potential of Design Thinking has been attributed to its ability to unlock modes of thinking that enable designers to recognise and develop revolutionary solutions to problems. The approach rests on four core principles; the human rule, the ambiguity rule, the re-design rule and the tangibility rule (Plattner et al. 2011). We have argued that implicit in these principles is the notion that their adoption will optimise creative framing, where framing is understood as a mental device that contextualises new information to give it meaning and significance. In this study, we focussed on the first two rules. We analysed them about the processes of framing that unfolded during a design challenge undertaken by two teams of student designers.
The analyses here provide clear evidence that Design Thinking holds promise as a methodology for helping designers shift beyond their immediate field of expertise to adopt alternative frames of reference. However, ideas, feedback and observations gathered during engagement with stakeholders inevitably appear to make their way through a filtering process that sets the tone of interpretation according to what is deemed "acceptable". Findings suggest that acceptability is evaluated using an array of heuristics; by appealing to pre-existing authorities such as individuals or institutions that hold positions of power, by drawing from dominant discourses or ideologies that privilege certain meanings or interpretations, and by social codes that govern privacy and respect. The emotional state evoked in designers plays an equally influential role as gatekeepers in the framing process. Situations that cause discomfort, whether those feelings are acknowledged or not, may function to censor essential parts of a story.
Future investigations into this topic will benefit the field of Design Thinking by exploring whether or not experience in applying the method plays a role in the types of frames that designers adopt. The designers in the current study were very newly acquainted with the methodology and with design in general, and the findings should be interpreted within this context. As the practice of implementing Design Thinking becomes more familiar, it is likely that student designers will gain confidence to conceptualise and brainstorm in new and unusual ways.
Despite this important limitation, the findings presented here suggest that without a holistic engagement with core Design Thinking concepts and toolkits, their realisation in practice will be hampered. Subtle biases and socially accepted ways of thinking that primarily operate outside of conscious awareness present barriers to their effective implementation. Especially in the health sphere, where problems are intimate and are often shrouded in stigma, the Design Thinking approach will benefit from the incorporation of a 5th overarching principle, and that is reflexivity. The term extends beyond the simple notion of "reflection" that already forms part of the Design Thinking toolkit (IDEO 2012). Schön (1983) uses the terms reflection-in-action or reflection-on-action to describe how professional growth and insight can emerge from a commitment to critical contemplation. However, reflexivity is also an ethical imperative to which all human investigations should be accountable. Nonetheless, while much progress can be gained through reflexivity alone, some frames may require explicit learning, such as those that articulate theories of human motivation and behaviour change (Deci and Ryan 2008; Schwarzer 2008). The challenge going forward will be in how to adapt Design Thinking, which emerged out of the technical sciences and flourished in the domain of business, for healthcare and its unique set of obstacles, without compromising the "bottom-up", user-centeredness that sets the approach apart from traditional design methodologies.
REFERENCES
Bacchi, C. 2009. "The issue of intentionality in frame theory: The need for reflexive framing." In The discursive politics of gender equality, 39-55. Routledge, UK. [ Links ]
Badke-Schaub, P. G., N. F. M. Roozenburg, and C. Cardoso. 2010. "Design thinking: A paradigm on its way from dilution to meaninglessness?" In Proceedings of the 8th Design Thinking Research Symposium (DTRS8), ed. K. Dorst, S. Stewart, I. Staudinger, B. Paton, and A. Dong, 39-49. [ Links ]
Balkrishnan, R. 1998. "Predictors of medication adherence in the elderly." Clinical Therapeutics 20(4): 764-771. [ Links ]
Barsalou, L. 2003. "Situated simulation in the human conceptual system: Language and Cognitive processes 18(5-6): 513-562. [ Links ]
Batson, C. D., J. Fultz, and P. A. Schoenrade. 1987. "Distress and empathy: Two qualitatively distinct vicarious emotions with different motivational consequences." Journal of Personality 55(1): 1939. [ Links ]
Bell, G. J., J. Ncayiyana, A. Sholomon, V. Goel, K. Zuma, and M. Emch. 2022. "Race, place, and HIV: The legacies of apartheid and racist policy in South Africa." Social Science & Medicine 296: 114755. [ Links ]
Bell, S. 2008. "Design thinking: A design approach to the delivery of outstanding service can help put the user experience first." American Libraries 39: 44-49. [ Links ]
Bjögvinsson, E., P. Ehn, and P. A. Hillgren. 2012. "Design things and design thinking: Contemporary participatory design challenges." Design Issues 28(3): 101-116. [ Links ]
Bracken, P. 2002. Trauma: Culture, meaning and philosophy. London: Whurr Publishers. [ Links ]
Brooks, A. K. 1994. "Power and the production of knowledge: Collective team learning in work organizations." Human Resource Development Quarterly 5(3): 213-235. [ Links ]
Brown, T. 2008. "Design Thinking." Harvard Business Review 86(6). [ Links ]
Brown, T. 2009. "Change by Design: How Design Thinking Transforms Organizations and Inspires Innovation." Harper Business, New York. [ Links ]
Brown, T. and B. Katz. 2011. "Change by design." Journal of Product Innovation Management 28(3): 381-383. [ Links ]
Buchanan, R. 1992. "Wicked problems in design thinking." Design Issues 8(2): 5-21. [ Links ]
Bucolo, S. and J. H. Matthews. 2010. "Using a design led disruptive innovation approach to develop new services: Practising innovation in times of discontinuity." In Proceedings of the 11th International CINet Conference: Practicing Innovation in the Times of Discontinuity, 176-187. CINet. [ Links ]
Bullock, H. E., K. Wyche, and W. R. Williams. 2001. "Media images of the poor." Journal of Social Issues 57(2): 229-246. [ Links ]
Carlgren, L., I. Rauth, and M. Elmquist. 2016. "Framing design thinking: The concept in idea and enactment." Creativity and Innovation Management 25(1): 38-57. [ Links ]
Clark, A. 1998. Being there: Putting Brain, Body, and World Together Again. MIT press, USA. [ Links ]
Cole, T. R 1992. The Journey of Life: A Cultural History of Aging in America. Cambridge University Press, UK. [ Links ]
Conrad, P. 2007. The Medicalization of Society: On the Transformation of Human Conditions into Treatable Disorders. The Johns Hopkins University Press, Baltimore. [ Links ]
Considine, M. 2012. "Thinking outside the box? Applying design theory to public policy." Politics & Policy 40(4): 704-724. [ Links ]
Davis, J. E. 2010. "Medicalization, social control and the relief of suffering." In The New Blackwell Companion to Medical Sociology, ed. W. C. Cockerham, 211-241. Malden, MA: Blackwell Publishers. [ Links ]
De Martino, B., D. Kumaran, B. Seymour, and R. J. Dolan. 2006. "Frames, biases, and rational decision-making in the human brain." Science 313(5787): 684-687. [ Links ]
Decety, J. and P. L. Jackson. 2004. "The functional architecture of human empathy." Behavioral and Cognitive Neuroscience Reviews 3(2): 71-100. [ Links ]
Deci, E. L. and R. M. Ryan. (Ed.). 2002. Handbook of self-determination research. University Rochester Press, USA. [ Links ]
Deci, E. L. and R. M. Ryan. 2008. "Self-determination theory: A macrotheory of human motivation, development, and health." Canadian Psychology/Psychologie Canadienne 49(3): 182. [ Links ]
Dorst, K. 2015. Frame Innovation. MIT Press, Cambridge, MA. [ Links ]
Finlay, L. and B. Gough. (Ed.). 2008. Reflexivity: A Practical Guide for Researchers in Health and Social Sciences. John Wiley & Sons, UK. [ Links ]
Foucault, M. 1980. Power/knowledge: Selected Interviews and Other writings, 1972-1977. Pantheon, New York. [ Links ]
Gasparini, A. 2015. "Perspective and use of empathy in design thinking." In ACHI, The Eight International Conference on Advances in Computer-Human Interactions, 49-54. [ Links ]
Gellad, W. F., J. L. Grenard, and Z. A. Marcum. 2011. "A systematic review of barriers to medication adherence in the elderly: Looking beyond cost and regimen complexity." The American Journal of Geriatric Pharmacotherapy 9(1): 11-23. [ Links ]
Giacomin, J. 2014. "What is human centred design?" The Design Journal 17(4): 606-623. [ Links ]
Gilovich, T., D. Griffin, and D. Kahneman. (Ed.). 2002. Heuristics and biases: The psychology of intuitive judgment. Cambridge university press, UK. [ Links ]
Giroux, H. A. 1988. "Border pedagogy in the age of postmodernism." Journal of Education 170(3): 162-181. [ Links ]
Goffman, E. 1974. Frame analysis: An Essay on the Organization of Experience. Harvard University Press, USA. [ Links ]
Hassi, L. and M. Laakso. 2011. "Conceptions of Design Thinking in the design and management discourses." In Proceedings of IASDR2011, the 4th world conference on design research, Delft, October 2011, 1-10. [ Links ]
Holloway, M. 2009. "How tangible is your strategy? How design thinking can turn your strategy into reality." Journal of Business Strategy 30(2/3): 50-56. [ Links ]
Hooks, B. 1989. Talking back: Thinking feminist, thinking black. South End Press. [ Links ]
IDEO. 2012. "Design Thinking for Educators Toolkit." http://designthinkingforeducators.com/. [ Links ]
IDEO. 2019. "Unlock your creative potential through IDEO U." https://www.ideou.com. [ Links ]
Johansson, U. and J. Woodilla. 2010. How to avoid throwing the baby out with the bath-water. In An ironic perspective on design thinking. European Group for Organization Studies Colloquium, Lisbon, Portugal. [ Links ]
Johansson-Sköldberg, U., J. Woodilla, and M. Çetinkaya. 2013. "Design thinking: Past, present and possible futures." Creativity and Innovation Management 22(2): 121-146. [ Links ]
Kahneman, D. and S. Frederick. 2007. "Frames and brains: Elicitation and control of response tendencies." Trends in Cognitive Sciences 11(2): 45-46. [ Links ]
Kahneman, D., J. L. Knetsch, and R. H. Thaler. 1991. "Anomalies: The endowment effect, loss aversion, and status quo bias." Journal of Economic Perspectives 5(1): 193-206. [ Links ]
Katz, S. 1996. Disciplining Old Age: The Formation of Gerontological Knowledge. University Press of Virginia, London. [ Links ]
Kim, J. and H. Ryu. 2014. "A design thinking rationality framework: Framing and solving design problems in early concept generation." Human-Computer Interaction 29(5-6): 516-553. [ Links ]
Kolko, J. 2010. "Sensemaking and framing: A theoretical reflection on perspective in design synthesis." Presented at the Design Research Society International Conference, Design & Complexity, Montreal, Canada. [ Links ]
Kolko, J. 2015. "Design thinking comes of age." Harvard Business Reviews 1: 66-71. [ Links ]
Lakoff, G. and M. Johnson. 2008. Metaphors We Live By. University of Chicago press. [ Links ]
Leavy, B. 2010. Design thinking - a new mental model of value innovation. Strategy & Leadership 38(3): 5-14. [ Links ]
Leifer, L. J. and M. Steinert. 2011. "Dancing with ambiguity: Causality behavior, design thinking, and triple-loop-learning." Information Knowledge Systems Management 10(1-4): 151-173. [ Links ]
Lindgaard, Karin and Heico Wesselius. 2017. "Once more, with feeling: Design thinking and embodied cognition." She ji: The Journal of Design, Economics, and Innovation 3(2): 83-92. [ Links ]
Liu, J. H. and D. J. Hilton. 2005. "How the past weighs on the present: Social representations of history and their role in identity politics." British Journal of Social Psychology 44(4): 537-556. [ Links ]
MacLaughlin, E. J., C. L. Raehl, A. K. Treadway, T. L. Sterling, D. P. Zoller, and C. A. Bond. 2005. "Assessing medication adherence in the elderly." Drugs & Aging 22(3): 231-255. [ Links ]
Martin, R. 2010. "Design thinking: Achieving insights via the 'knowledge funnel'." Strategy & Leadership 38(2): 37-41. [ Links ]
McElroy, T. and J. Conrad. 2009. "Thinking about product attributes: Investigating the role of unconscious valence processing in attribute framing." Asian Journal of Social Psychology 12(2): 157-161. [ Links ]
Neumeier, M. 2009. The Designful Company: How to build a culture of nonstop innovation. Peachpit Press, Germany. [ Links ]
Plattner, H. 2010. An introduction to design thinking process guide. The Institute of Design at Stanford: Stanford. https://dschool-old.stanford.edu/sandbox/groups/designresources/wiki/36873/attachments/74b3d/ModeGuideBOOTCAMP2010L.pdf [ Links ]
Plattner, H., C. Meinel, and L. Leifer. 2011. "Design Thinking: Understand, improve, apply." Springer Science & Business Media 36. [ Links ]
Premack, D. and G. Woodruff. 1978. "Does the chimpanzee have a theory of mind?" Behavioral and Brain Sciences 1(4): 515-526. [ Links ]
Rassin, E., P. Muris, E. Booster, and I. Kolsloot. 2008. "Indecisiveness and informational tunnel vision." Personality and Individual Differences 45(1): 96-102. [ Links ]
Rittel, H. J. and M. M. Webber. 1973. "Dilemmas in the general theory of planning." Policy Science 4: 55-169. [ Links ]
Sandmann, L. R. 2009. "Placing Scholarly Engagement 'on the desk'." Essay. http://www.compact.org/wp-content/uploads/2009/04/sandmann-final.pdf. (Accessed November 2018). [ Links ]
Schön, D. A. 1983. The reflective practitioner. New York: Basic Books. [ Links ]
Schwarzer, R. 2008. "Modelling health behaviour change: How to predict and modify the adoption and maintenance of health behaviours." Applied Psychology 57(1): 1-29. [ Links ]
Smith, E. E. and D. L. Medin. 1981. Categories and Concepts. (Vol. 9). Cambridge, MA: Harvard University Press. [ Links ]
Smith, J. A. and M. Osborn. 2003. Interpretative Phenomenological Analysis in Qualitative Psychology: A practical Guide to Methods. Sage, London. [ Links ]
Stolterman, E. 2008. "The nature of design practice and implications for interaction design research." International Journal of Design 2(1). [ Links ]
Strauss, A. and J. Corbin. 1990. Basics of qualitative research. Sage publications. [ Links ]
Streib, J., M. Ayala, and C. Wixted. 2017. "Benign inequality: Frames of poverty and social class inequality in children's movies. Journal of Poverty 21(1): 1-19. [ Links ]
Van Leeuwen, J., D. Rijken, I. Bloothoofd, E. Cobussen, B. Reurings, and R. Ruts. 2016. "Thematic Research in the Frame Creation Process." In Service Design Geographies. Proceedings of the ServDes. May 2016 Conference 125: 352-364. Linköping University Electronic Press. [ Links ]
Vincent, J. A. 2006. "Ageing contested: Anti-ageing science and the cultural construction of old age." Sociology 40(4): 681-698. [ Links ]
Whelton, M. G. 2004. "The Development of Purpose in the Project Definition Phase of Construction Projects." DPhil dissertation, University of California, Berkeley. [ Links ]
Witt, J. K. and D. R. Proffitt. 2008. "Action-specific influences on distance perception: A role for motor simulation." Journal of Experimental Psychology: Human Perception and Performance 34(6): 1479. [ Links ]
Wright, D. W. 1996. "Infrastructure planning and sustainable development." Journal of Urban Planning and Development 122(4): 111-117. [ Links ]


{kind=link}
{kind=link}