










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.22 no.4 Centurion 2023
http://dx.doi.org/10.17159/2309-8309/2023/v22n4a2
KNEE
Coding guidelines for soft tissue knee procedures based on a national Delphi consensus study
Michael HeldI, *; David NorthII; Peter HardcastleIII; Peter ErasmusIV; Ponky FirerV; Bradley GelbartV; Michael BarrowVI; Richard von BormannVII; Robert DunnI
IDepartment of Orthopaedic Surgery, Groote Schuur Hospital, University of Cape Town, Cape Town, South Africa
IIDepartment of Orthopaedic Surgery, Paarl Hospital, Western Cape, South Africa
IIIVergelegen Mediclinic, Somerset West, Cape Town, South Africa
IVKnee Clinic, Stellenbosch, South Africa
VLinksfield Orthopaedic Sports and Rehabilitation Centre, Wits Institute of Sports and Health, University of the Witwatersrand, Johannesburg, South Africa
VISunninghill Hospital and The Waterfall Sports Centre, Sandton, South Africa
VIICape Town Sports and Orthopaedic Clinic, Christiaan Barnard Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND: No guidelines for ethical coding practice of commonly performed soft tissue knee procedures exist in South Africa. The aim of our study was to establish and prioritise codes for these procedures via a consensus of knee surgeons.
METHODS: Fifty-nine South African Knee Society (SAKS) members were approached for a blinded Delphi consensus process. In the first survey round, a list of codes was generated which was prioritised in subsequent rounds. Agreement of 70% or more was defined as consensus. These codes were then moderated during a fourth round by the SAKS committee.
RESULTS: Sixteen SAKS members, performing a median of 200 knee procedures (interquartile range [IQR] 115-312) annually, participated in each round. Consensus was achieved for codes 0667, 0614 and 0673 when coding for meniscus and cartilage surgery. For anterior cruciate ligament reconstruction 0667, 0614, 0679, 0673 and 0775 all reached consensus. Here, some codes (0593) did not achieve consensus although their inclusion was promoted by the SAKS committee round. Furthermore, 88% of the participants agreed that rule 0005 should be used for multiple knee ligament reconstruction, and each should be seen as a separate procedure. Code 0592 (36%) should not be routinely used for minor debridement. No code exists to code for increased complexity in meniscal root repairs and therefore 0677 was proposed to be reassigned for meniscus repair, as well as 0296 to code for the major technical nature of the procedure. For medial patellofemoral ligament reconstructions, 0679 (88%) and 0579 (63%) were proposed along with 0667 (100%), 0775 (94%) and 0614 (69%). For osteotomy of the knee region, codes 0527 (94%) and modifier 0051 were put forth, as well as 0667 (75%), 0614 (75%) and 0673 (56%). When bone is harvested and/or grafted, 0507 (56%) and 0499 (44%) respectively are also thought to be appropriate.
CONCLUSION: This consensus study is based on the coding practice of 16 members of the South African Knee Society performing a median of 200 knee procedures annually. A variety of techniques are available, some without specific allocated codes which called for moderation and reallocation of certain codes. With this work we hope to achieve transparent and consistent coding for soft tissue knee procedures.
Level of evidence: Level 4
Keywords: coding, billing, soft tissue knee procedures, arthroscopy, South Africa
Introduction
Determining one's value in orthopaedic private practice is daunting, especially for novice surgeons. Here we walk a fine line between altruistic social obligation to the patient and commercial self-interest regarding our practice and family. In South Africa, coding for procedures was introduced to allow standardisation of remuneration as legislated by Section 53(3) paragraph D of the Health Professions Act (56 of 1974). Since the introduction of this system, few changes have been made, which creates challenges to code in an evolving field. A Competition Commission ruling in 2004 prohibited collective negotiation on healthcare tariffs. Healthcare professionals must therefore negotiate tariffs with medical schemes individually.1 It was also stated that public sectors and representative associations are not permitted to negotiate tariffs on behalf of their members.
The medical scheme tariff model represents an application of the resource-based relative value scale.1 Here medical schemes have assessed their claims risk profile based on the number of claims processed during prior periods. This includes the risk of reoccurrence of claims during current periods as well as available funds. It resulted in medical schemes offering surgeons tariffs that schemes could afford, without healthcare professionals being able to assess whether they could deliver sustainable healthcare services at the offered prices.
Furthermore, the reimbursement is limited to codes approved by the medical aid. These codes are often not in line with professional recommendations and are not fully inclusive of all appropriate codes that may be charged for a procedure. And so multiple codes, with decreasing percentage of value, need to be used in order to appropriately reflect the work performed. Adding to the complexity, different medical aids choose to reimburse different codes for the same procedure. Similarly, different surgeons utilise different codes for the same procedure. This results in lack of predictability in income for the surgeon, costs for the patients and costs for the medical schemes.
The National Reference Price List (NRPL) was designed by the Council for Medical Schemes on behalf of the Department of Health. This list does not contain negotiated prices, and is created by gathering submissions from the health service with suggestions regarding the actual cost of running a practice. Based on practice costs estimated in excess of three times NRPL rates, a private practice turnover of 3.2 and 3.7 times a state-employed specialist cost-to-company package is needed to match that salary.2 This is dependent on years of service and taking into account overtime, working hours and holiday.2
Ideally, remuneration should be ethical, affordable to patients, medical aids and society, but also sustain our surgical business.3 In the current remuneration structure, many surgeons might not charge more than NRPL rates due to their patients' backgrounds. To make their targets of turnover they might need increased volumes with the potential risk of over-servicing patients or surgeon burnout.4 Others are billing at a higher rate which can lead to exclusion from referral groups or designated service-provider systems.
The drive to receive higher payment may also lead to excessive coding, especially when surgeons are unable to charge above NRPL, or to look into other perverse incentives.5 Here, a transparent billing practice with consistent codes of procedures performed is key to avoid this. Yet, these guidelines are not available for surgeons in South Africa which can have detrimental effects on funders, patients and surgeons alike. This is especially true for soft tissue knee surgery, which is the most common elective orthopaedic surgery performed worldwide.6
The aim of this study was to provide a bundle of codes which can be used consistently, are reviewed by high volume knee surgeons, and endorsed by the South African Knee Society (SAKS).
Methods
We performed a modified Delphi consensus study, comprising three iterative rounds, producing codes which were then moderated by a study panel. In the first round, orthopaedic surgeons who were members of SAKS were asked to provide the codes they use for certain soft tissue knee procedures (Table I). For each procedure, they were also prompted to include an acceptable estimate of total unit value as per the 2021 Medical Doctors Coding Manual (available at https://www.samedical.org/products). The specific descriptions of the codes used in this manuscript are shown in Table II. These codes were prioritised by the participants in a second round, blinded to answers of the cohort. In a third round, the percentage agreement for each code used in a procedure was shown to the participants who could then adjust codes. The consensus rounds were performed over three months starting in April 2023, with the rounds occurring every second week. Reminders were sent via email to non-respondents at least three times, every three days. The age, years of experience and self-reported annual case volume of knee surgeries done were provided by the participants. Consensus was defined as agreement of 70% of participants or more. Anonymity was ensured throughout this process by deleting identifiable information. In a final meeting among executive committee members of SAKS as well as four previous SAKS presidents, these prioritised codes were then discussed and a final recommendation was provided along with specific reasoning for the recommendations. The study was approved by a local review board (HREC 141/2023) and informed consent was obtained prior to participation.

Data capture and analysis
The data was captured with Research Electronic Data Capture (REDCap), an electronic database, and hosted at the main study centre. The study population was described by summarising normally distributed continuous data by mean, standard deviations (SD) and 95% confidence intervals (CI), whereas non-normally distributed continuous data were summarised by median and interquartile range (IQR). To summarise categorical data, 95% CIs with proportions were used.
Sample size
All 59 SAKS members were targeted for the first round to provide a list of factors. Statistical representativeness of the sample as for other surveys do not apply for Delphi studies.7 Participant numbers for subsequent consensus rounds as low as 10-15 and as high as 50-70 were considered acceptable.8,9
Results
Participants
Throughout all three rounds, 16 members provided feedback. They had a median age of 53 years (IQR 46-57), with an average of 20 years (IQR 13-30) experience, performing a median of 200 knee procedures (IQR 115-312) per year. All but one (state practice with limited private practice) were surgeons with a full-time private practice. All Ave executive committee members provided input for the moderation of the prioritised list.
Consensus rounds and moderation statements
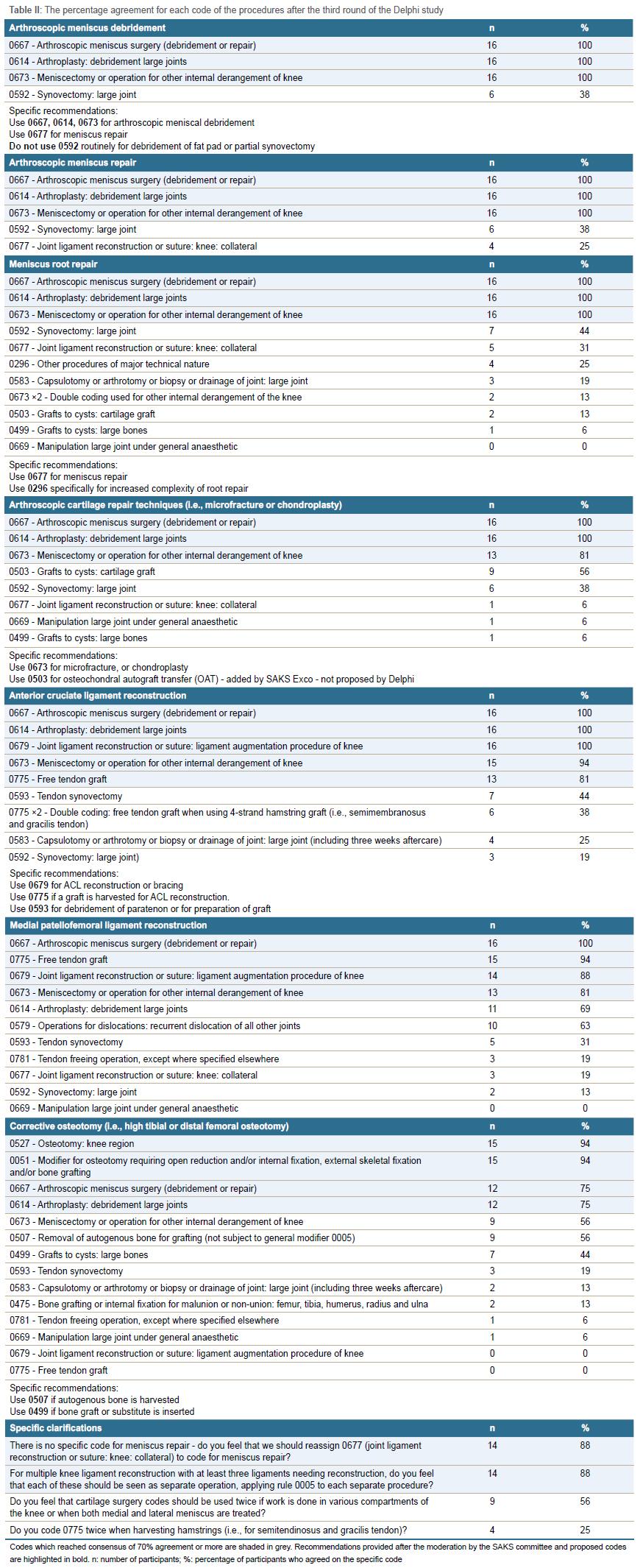
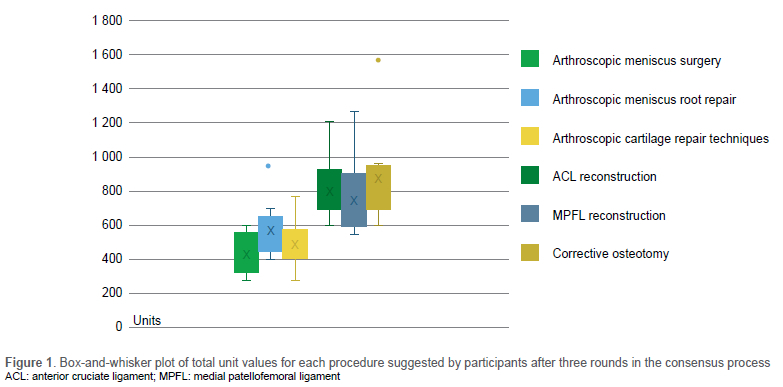
Table II shows the percentage agreement for each code of the procedures prioritised after the third round of the Delphi study. The codes proposed after the moderation by the SAKS committee are also highlighted with specific recommendations given. Participants also provided feedback regarding acceptable total unit values for each procedure. Here, higher valued procedures were medial patellofemoral ligament (MPFL) reconstruction for patellofemoral instability, anterior cruciate ligament (ACL) reconstruction and corrective osteotomy (Figure 1).
Discussion
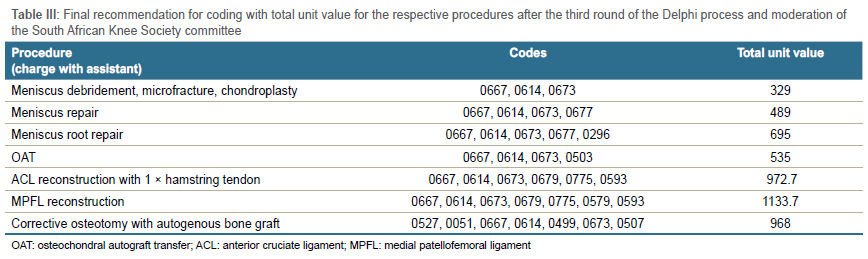
Based on this study and the moderation by SAKS, the recommendations of codes for the specific procedures are shown in Table III. Besides the specific procedure codes, the SAKS moderation round agreed that assistants are necessary for most arthroscopies and codes should be charged accordingly. To compare coding practice to guidelines of other countries is extremely challenging as it is often bundled into a single code per procedure. In our discussion we have therefore related some of our findings to the US system, which still uses some individual codes for various surgical steps.
Arthroscopic meniscus debridement
For general arthroscopic meniscus debridement, codes 0667, 0614 and 0673 reached more than 70% agreement and were also recommended by the moderation committee. The moderation round came to the conclusion that using a cartilage surgery code twice is acceptable if work is done in various compartments of the knee or when both medial and lateral meniscus are treated. Of the participants, 56% agreed with this. Similarly, the US National Correct Coding Initiative (NCCI) Policy Manual for Medicare Service suggests different codes for medial OR lateral meniscus versus medial AND lateral meniscus work to differentiate between this.10 The moderation round further decided that synovectomy, 0592 (38% agreement), should not be used for routine debridement of fat pad or partial synovectomy, but mainly for extensive synovitis such as in tuberculosis or pigmented villonodular synovitis. This is also in line with NCCI coding practice, where minor (i.e. plica or fat pad debridement) and major synovectomy can be differentiated and can only be billed when it is the only arthroscopic procedure performed.10
Meniscus repair
The group recommended 0677 should be used for meniscus repair. Although only 25% of participants selected this code during the consensus rounds, a later specific proposal to reassign 0677 to meniscus repair reached agreement in 88%. This process of reallocation is possible as the South African Orthopaedic Association and its subgroup societies inform and determine the assignment of codes to certain procedures. The low consensus agreement is likely due to the fact that no specific code is available to compensate for increased complexity when compared to meniscus debridement. Similarly, the US NCCI uses a separate code which does exist in this system for meniscus repair.10 The SAKS moderation round also suggested to code for increased complexity in transosseous meniscus root repairs compared to other forms of meniscus repairs. For this code 0296 should be used, although this was only selected by 24% of participants during the consensus process.
Arthroscopic cartilage repair techniques
Various new techniques have been established recently which do not have appropriate codes available. Here 0673 should be used for microfracture or chondroplasty. Again, the majority of the group felt that double coding was acceptable if work is done in various compartments of the knee (i.e. for microfracture in the patellofemoral and medial tibiofemoral compartment) or when separate meniscus debridement is done. In the US, billing for chondroplasty is only possible if this is done in a separate compartment.10 For osteochondral autograft transfer (OAT), 0503 should be used but case-by-case motivation will likely be triggered with some funders. This code was only mentioned in discussions with previous SAKS presidents and seemed not to be known in general knee surgery coding practice as reflected by its absence in the list of codes submitted in the consensus rounds.
ACL reconstruction and multiple knee ligament injuries
Multiple codes were prioritised with more than 70% agreement during the consensus study: 0667, 0614, 0679, 0673 and 0775. Here, 0679 can be used either for reconstruction or ligament bracing. Double coding if more than one graft is harvested (i.e., semitendinosus and gracilis tendon) can be added. This was supported by a majority of committee members although some mentioned that they do not follow this coding practice currently and only 25% of participants agreed with this in a specific question about double coding. Use of 0593 for debridement of paratenon or for preparation of graft was seen as appropriate coding practice. Furthermore, for multiple knee ligament reconstruction with at least three ligaments needing reconstruction, 88% of participants felt that each of these should be seen as a separate operation, applying the 0005 to each separate procedure.
Medial patellofemoral ligament (MPFL) reconstruction
Participants proposed one of the highest average total unit values for MPFL reconstruction; only ACL reconstructions and osteotomies were valued higher. This reflects the complexity in the surgery and management of patients with patellofemoral instability. The moderation round concluded that the total unit value should increase when the surgery is more technically demanding, yet there was no agreement which of the procedures (ACL reconstruction, MPFL reconstruction, osteotomy) should be assigned the highest value. For MPFL reconstruction, 0667, 0679, 0673 and 0775 received consensus of more than 70%. Besides these codes, the committee recommended the use of 0614, 0579 and 0593. These all describe important aspects of instability surgery involving tendon grafts and treating internal derangement of the knee. As for ACL reconstructions, 0593 for debridement of paratenon or for preparation of graft was proposed to be appropriate coding practice.
Corrective osteotomy
Consensus was reached for codes 0527, 0051, 0667 and 0614. Further codes which did not reach consensus were still recommended by the SAKS committee for specific scenarios. Code 0673 should be used if osteotomies are done for cartilage, meniscus or ligamentous derangements. If autogenous bone is harvested for grafting, i.e., in open wedge osteotomies, 0507 should be used. Also, code 0499 should be used if bone graft or bone substitute is inserted. The total unit value suggested by the participants ranked corrective osteotomies highest (Figure 1), but this was not the case when calculating the total unit value with the proposed codes (Table III). MPFL or ACL reconstruction reached higher unit values, even though complexity, risk of complications and follow-up requirements are more. This shows the need for a coding reform beyond simply guiding current practice. For example, in US billing guidelines, ACL, MPFL and osteotomy surgery is bundled into one code which excludes meniscal or cartilage work.10 Due to the increased perioperative and postoperative risks of osteotomy, the moderation round agreed that this justifies greater total unit value.
This study had some limitations. First, only 16 South African orthopaedic surgeons took part in each round, most of whom had a high case volume and were more advanced in their career. This could introduce bias and overshadow opinions of surgeons with lower case volumes. Years of practice or case volume does not necessarily equate to the correct use of coding with high ethical standards. Secondly, the definition of consensus was set at 70%. This might have resulted in certain codes narrowly missing the definition of agreement although they might be appropriate. The moderation round of the executive committee attempted to take this into consideration and has included codes of lower consensus agreement in their recommendations. Thirdly, corrective osteotomy was not specified into various types of osteotomies, i.e., high tibial osteotomy, distal femoral osteotomy, tibial tubercle osteotomy or more complex osteotomies such as trochleoplasty. Coding recommendations specific to the complexity, risk and follow-up implications of these osteotomies could therefore not be made. Finally, the executive committee round was not blinded during the discussion which could have led to more vocal members enforcing their opinion.
Conclusion
This study provides a bundle of codes which can be used to achieve transparent, consistent and, therefore, ethical coding for soft tissue knee procedures. It is based on the coding practice of members of the South African Knee Society and should be seen as dynamic guidelines which can be further modified. Future focus should be directed at discussion with funders to allow coding for procedures without current coding options. Ultimately, this list may be used to guide coding practices for procedures that are acceptable to surgeons, hospitals and funders. The value of our work is dynamic, influenced by demand and supply, but should reflect our goal to grow both social and commercial capital with our practice.
Acknowledgements
he following surgeons critically reviewed codes and provided feedback throughout the Delphi study: Naude Marais, Eugene Pelser, Jason Sagor, Deon Engela, Daniel Morkel, Frederick du Plessis, Graham Bayes, Avesh Magan, Mphele Tladi, Peter Smith, Jaco Willers.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Prior to commencement of the study, ethical approval was obtained from the following ethical review board: University of Cape Town (HREC 141/2023). Informed consent was obtained prior to participation.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
MH: design, data collection and analysis, and manuscript preparation
DN: data collection, analysis and manuscript preparation
PH: data analysis and manuscript preparation
PE: conceptualisation and manuscript preparation
PF: data collection, data interpretation and manuscript preparation
BG: data interpretation and manuscript preparation
MB: conceptualisation, data analysis and interpretation as well as manuscript preparation
RvB: conceptualisation, data interpretation and manuscript preparation
RD: conceptualisation, data analysis and manuscript preparation
ORCID
Held M https://orcid.org/0000-0002-0671-0439
North D https://orcid.org/0000-0003-3918-3206
Gelbart B https://orcid.org/0000-0003-2024-0442
Von Bormann R https://orcid.org/0000-0002-4546-3143
Dunn R https://orcid.org/0000-0002-3689-0346
References
1. South African Medical Association. https://www.samedical.org/private-health/practice-cost-calculator (date last accessed 1110.22) [ Links ]
2. Dunn R. Ethics of billing: determining one's value. SA Orthop J [Internet]. 2011;10:20-25. Available from: http://www.scielo.org.za/scielo.php?script=sci_arttext&pid=S1681-150X2011000200003&nrm=iso [ Links ]
3. Ramme AJ, Patel M, Patel KA, et al. Personal finance primer for the future orthopaedic surgeon: A starting point. JBJS Open Access. 2021;6(1). [ Links ]
4. Mir H, Downes K, Chen AF, et al. Physician wellness in orthopaedic surgery: a multinational survey study. Bone Jt Open. 2021;2(11):932-39. [ Links ]
5. Legotlo TG, Mutezo A. Understanding the types of fraud in claims to South African medical schemes. South African Med J. 2018;108(4):299-303. [ Links ]
6. Blom AW, Donovan RL, Beswick AD, et al. Common elective orthopaedic procedures and their clinical effectiveness: umbrella review of level 1 evidence. BMJ 2021;374:n1511. [ Links ]
7. Delbecq AL, Van de Ven AH, Gustafson DH. Group techniques for program planning: A guide to nominal group and Delphi processes. 1975. Scott, Foresman Glenview. [ Links ]
8. Ludwig B. Predicting the future: Have you considered using the Delphi methodology? J Ext. 1997. [ Links ]
9. Witkin BR, Altschuld JW, Altschuld J. Planning and conducting needs assessments: A practical guide. Sage. 1995. [ Links ]
10. National Correct Coding Initiative [Internet].. NCCI Policy Manual Archive. 2022. Available from: https://www.cms.gov/ncci-medicare/medicare-ncci-policy-manual. [ Links ]
Received: August 2023 (resubmission)
Accepted: August 2023
Published: November 2023
* Corresponding author: michael.held@uct.ac.za
Editor: Dr Thomas Hilton, University of Cape Town, Cape Town
Funding: No funding was received for this study.
Conflict of interest: All authors are surgeons working in private practice and therefore have commercial interest in orthopaedic surgery.


{kind=link}
{kind=link}
{kind=link}