










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.22 n.3 Centurion 2023
http://dx.doi.org/10.17159/2309-8309/2023/v22n3a7
CASE REPORT
ORTHOPAEDIC ONCOLOGY AND INFECTIONS
A case of tenofovir-induced extreme osteopaenia
Marcelia TheronI; William D HarrisonII; Nando FerreiraI, *
IDivision of Orthopaedic Surgery, Department of Surgical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IILiverpool Orthopaedic and Trauma Service, Liverpool University Hospitals Foundation Trust, Liverpool, United Kingdom
ABSTRACT
BACKGROUND: Tenofovir disoproxil fumarate (TDF) is classified as a nucleoside reverse transcriptase inhibitor (NRTI). TDF is integral to several first-line treatment regimens for HIV and post-exposure prophylaxis. This case details an example of severe tenofovir-induced osteopaenia. We hope to raise awareness of this side effect so that it may be screened for more effectively and to provide an approach to management in secondary care.
CASE REPORT: We present the case of an HIV-positive, 52-year-old woman who had been on TDF treatment for over ten years. She presented complaining of progressively worsening weakness, bone pain and immobility and sustained spontaneous fractures of multiple long bones. Tenofovir-induced hypophosphaetemic osteomalacia and osteopaenia was diagnosed based on clinical, radiographic and laboratory findings.
DISCUSSION: The patient was successfully treated through the fixation of her long bone fractures with intramedullary nails and prophylactic nailing of the remaining long bones in her lower extremities. She received calcium and phosphate supplementation, and the causative agent was stopped.
CONCLUSION: HIV-positive patients on TDF should be screened routinely for renal function, and symptoms such as bone pain should not be ignored. Cessation of the causative agent and correct supplementation are critical adjuncts to surgical intervention for improved outcomes in these patients. In cases of severe osteopaenia, orthopaedic surgeons should consider prophylactic fixation of long bones and use intramedullary fixation where possible.
Level of evidence: Level XX
Keywords: tenofovir, osteopaenia, insufficiency fracture, HIV, orthopaedics
Background
Complications and morbidity in patients infected with HIV may arise from the disease itself or as side effects of the antiretroviral (ARV) agents used to treat it. Many first-line treatment regimens for HIV and post-exposure prophylaxis include tenofovir disoproxil fumarate (TDF) as the primary nucleoside reverse transcriptase inhibitor (NRTI).
Osteopaenia is a common complication of TDF use, with a frequency of up to 60.4% in some studies.1 Other studies have shown that loss of bone density following treatment with TDF may be reversible if the drug is stopped.2
This case details an example of uncommonly severe TDF-induced osteopaenia. Herein we present the case of a 52-year-old woman who was HIV-positive and had been on TDF treatment for over ten years. She presented complaining of progressively worsening weakness, bone pain and immobility. Her bone quality, unmonitored, progressively declined over a period of years while she lived in a rural area and was not recognised until spontaneous fractures occurred.
The patient was successfully treated through the fixation of her long bone fractures with intramedullary nails and prophylactic nailing of the remaining long bones in her lower extremities. She received calcium and phosphate supplementation, and the causative agent was stopped.
Through appropriate screening, complications of ARV treatment, such as TDF-induced osteopaenia and osteomalacia, can be treated successfully with early intervention. Cessation of the causative agent and correct supplementation are critical adjuncts to surgical intervention for improved outcomes in these patients.
Case report
A 52-year-old female patient presented with a left femur fracture following a low-energy fall from her bed. While she was being positioned for an X-ray, she sustained an iatrogenic left tibia fracture.
The patient was not a smoker and did not drink alcohol. She had had three previous pregnancies delivered at term, was post-menopausal, and was not on contraceptives or hormone replacement therapy. She suffered from hypertension, diagnosed 15 years prior and well-controlled. Her HIV diagnosis was made ten years earlier, for which she was promptly initiated on a fixed-dose combination of ARVs. She was virally suppressed at presentation, with a viral load lower than the detectable limit. Notably, the patient also had a history of pulmonary tuberculosis, diagnosed in 2014, for which she had completed treatment.
On history taking, the patient reported a gradual onset of weakness, myalgia, arthralgia and bone pain, primarily affecting her lower back and pelvic girdle. These symptoms had started in 2015, six years before her admission. Her condition had progressively worsened without surveillance. She developed significant weight loss, an unsteady gait, and finally, became unable to ambulate.
By the time of her presentation, she had been using a wheelchair for four years (since 2017). Considering the patient's history of retroviral disease and the context of her main complaint, TDF-induced osteopaenia and osteomalacia were suspected early in the patient's workup. For this reason, TDF was stopped and replaced with abacavir soon after her admission. Multiple myeloma was ruled out based on negative investigations.
Investigations
On admission, radiographs demonstrated significant osteopaenia and a pathological segmental fracture of the left femur. During positioning for radiographs, the patient sustained an iatrogenic left tibia fracture (Figure 1). A chest radiograph also suggested osteopaenia, with beading of the costochondral junctions and multiple old rib fractures. Spinal radiographs demonstrated insufficiency fractures of numerous thoracic and lumbar vertebrae, with lateral views of her spine showing biconcavity of the vertebrae, suggestive of osteomalacia.
HIV viral load was lower than the detectable limit, with an absolute CD4 of 402 cells/mm3. The patient was found to be vitamin D deficient with a total 25-OH vitamin D of 25.7 nmol/L (normal range: 50-125 nmol/L). This later improved to 44.4 nmol/L following the initiation of weekly parenteral vitamin D supplementation. Subclinical hyperthyroidism was diagnosed based on a thyroid-stimulating hormone (TSH) level of less than 0.01 L mlU/L. Thyroxine (free T4) was 22.3 initially (which later improved to 13.7 after initiation on carbimazole 5 mg PO daily).
Parathyroid hormone (PTH) was elevated at 7.6 pmol/L (normal range: 1.6-6.9 pmol/L). Twenty-four hour urine collection was done to measure the patient's urine phosphate, creatinine, calcium, and respective ratios. The urine volume was 900 mL. Details of urine and blood results are listed in Table I.

Differential diagnosis
Multiple myeloma was considered in the differential diagnosis as many of her symptoms of bone pain, pathological fractures, fatigue, anaemia and renal impairment were suggestive of multiple myeloma. However, there were no radiographical features of multiple lytic lesions, and the patient was hypocalcaemic. No pronounced monoclonal peak was observed on serum protein electrophoresis on serum plasmapheresis.
TDF-induced hypophosphataemic osteomalacia and osteo-paenia was diagnosed based on the clinical, radiographic and laboratory findings. The patient presented with hypophosphataemia, vitamin D deficiency and renal impairment with an elevated ALP, with multiple radiographs demonstrating critical features of osteomalacia and osteopaenia. The diagnosis was further supported by a whole-body bone scan, which confirmed increased bone turnover in keeping with osteomalacia. Furthermore, absent renal uptake was suggestive of significant renal impairment. Unfortunately, a DEXA scan could not be done on this patient as adequate positioning was not possible due to her fragility.
Treatment
The patient was promptly referred to endocrinology for co-management and started on calcium, vitamin D and intravenous phosphate supplementation. She consented to left femur and left tibia internal fixation with intramedullary nails, which were technically challenging due to the severe osteopaenia.
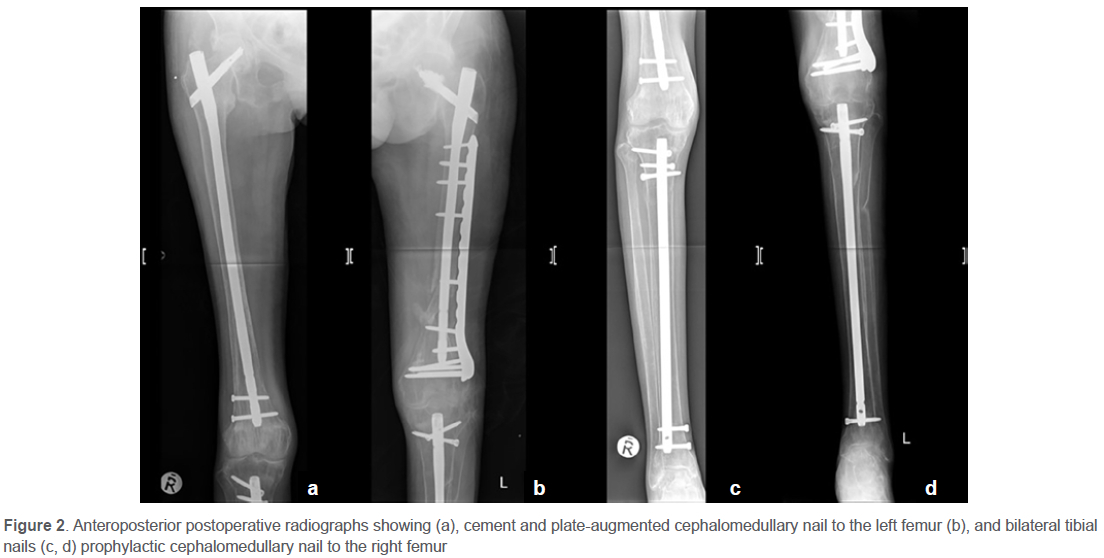
Two days postoperatively, the patient fractured the contralateral tibia while mobilising in bed. The patient was again taken to theatre, the fracture reduced, and an intramedullary nail inserted for her right tibia, while a prophylactic intramedullary nail was inserted for her right femur (Figure 2).
Outcome and follow-up
The patient's ARV regimen was changed, with abacavir prescribed in place of TDF. Patients receiving abacavir have been found to have a lower risk of developing hypocalcemia and less significant BMD loss than patients receiving TDF.3,4
She was discharged on carbimazole, atenolol and amlodipine to treat her existing comorbidities of hypertension and hyperthyroidism and received supplementary calcium, phosphate and vitamin D. Her levels showed improvement by the time of discharge.
The patient was assisted postoperatively with gentle bed mobilisation and, at the time of discharge, was sent home in a wheelchair for slow mobilisation, as advised by her physiotherapists. Early mobilisation has been shown to improve functional outcomes with increased walking distance, decreased pain and shorter lengths of stay among orthopaedic patients after surgery.5
Discussion
TDF is classified as a nucleoside reverse transcriptase inhibitor (NRTl). NRTls prevent the replication of retroviruses by inhibiting viral reverse transcriptase, thereby terminating the chain of viral DNA synthesis.
Current regimens by the International Antiretroviral Society (IAS) advise that first-line treatment be composed of two NRTIs, and one NNRTI (non-nucleotide reverse transcriptase inhibitor). As per these guidelines, TDF is integral to several first-line treatment regimens and for post-exposure prophylaxis.6
TDF has, in many cases, been linked to an increased bone turnover and substantial loss of bone mineral density (BMD). The incidence of osteopaenia was found to be 1-3% greater in TDF use compared to other ARVs. A longitudinal study conducted in Japan suggested the risk of osteopaenic fractures is increased in relation to the duration of treatment, with increased risk in those receiving treatment for more than five years.7 The patient in this case study had been on TDF for at least six years. Patients with osteomalacia typically present with weakness, bone pain and insufficiency fractures most commonly involving the spine and metaphyses of long bones.
This case was orthopaedically complex as the bone quality was so poor that there was a concern of peri-prosthetic fractures and implant failure. The principle of fixation was to span the entire length of the bone and use an intramedullary device where possible. A fundamental principle is to prophylactically fix the femoral neck, a potential stress riser around an orthopaedic femoral implant. Given the extremely low energy required to fracture the femur and the tibia, the decision was made to prophylactically fixate all the long bones of the lower limb. During reaming of the intramedullary canal, care was taken to use a slightly curved olive-tipped guidewire to direct the reamer away from the cortex. Reaming was performed under fluoroscopic control to avoid perforation of the cortex, which would have been easy in this case. The femoral head lag screw was augmented with injectable cement to improve the implant's hold in this very soft bone.
This patient also suffered from a substantial vitamin D deficiency, which in some studies has been associated with the use of TDF in conjunction with other ARVs such as emtricitabine. Regarding this, the patient was already more susceptible to vitamin D deficiency than the general population; factors such as her advanced age and low BMI are likely to have increased her risk.
Other general risk factors associated with vitamin D deficiency include male sex, lower latitudes and ARV therapy.8 Suboptimal vitamin D levels, such as those measured in this patient, have been found to increase the risk of secondary hyperparathyroidism. This would exacerbate the resorption of calcium from bone, further contributing to the development of osteomalacia in such patients.9
Fanconi syndrome is a rare but known complication of TDF contributing to the loss of BMD. TDF is primarily excreted renally and excreted unchanged. It has been noted to cause damage to the proximal tubules, resulting in excess excretion of calcium and phosphates in the urine. Management of Fanconi syndrome typically entails replacing lost minerals through supplements.10
TDF's mechanism of impact on BMD is complex and not yet fully understood; however, this implies that it is not solely driven by the renal excretion of calcium and phosphates. A recent study has found that TDF inhibits the activity of human osteoblasts, interfering with osteoblast function in bone mineralisation and osteoblast differentiation. These effects were found to be dose dependent.11
Osteoclast formation is also stimulated as the secretion of adenosine triphosphate is inhibited as a side effect of TDF, thus leading to a decrease in extracellular adenosine levels, which would typically inhibit osteoclast formation.12 The current patient's bone scan was suggestive of osteomalacia, showing an increased bone uptake in multiple areas. This implies that a similar process was at work in our patient.
The gold standard for diagnosing osteomalacia is a bone biopsy of the iliac crest. Visualised under fluorescence microscopy via tetracycline administration, it labels the bone through its binding to hydroxyapatite.13 Unfortunately, this investigation was declined by the patient.
The role of HIV clinics in identifying complications
The Centers for Disease Control and Prevention (CDC) provide well-outlined guidelines for the routine screening, treatment and monitoring of HIV infection, as follows:14
• A full blood count and comprehensive metabolic profile should be done every three to six months.
• Newly diagnosed HIV patients must be screened for renal disease. Baseline renal function is assessed through urinalysis, creatinine clearance and glomerular filtration rate. Screening must be done at the time of diagnosis and then biannually.
• A full lipogram is advised to be done annually.
• In patients older than 50 years, attending clinicians should consider dual-energy X-ray absorptiometry (DEXA) scan.
Patient adherence to ARV therapy should be addressed at every point of care. Poor compliance is often multifactorial, ranging from social, financial, behavioural, neuropsychiatric and side-effect related issues.15
What orthopaedic surgeons need to know about ARVs
Currently, recommended regimens typically consist of one NNRTI or a protease inhibitor (PI) and two NRTIs,7 with TDF, an NRTI, forming the backbone of many of these regimens.
HIV-infected patients more commonly present with osteopaenia, osteoporosis and vitamin D deficiency compared to uninfected patients.16 Among HIV-infected individuals, the approximate frequency of osteopaenia and osteoporosis is 44% and 13%, respectively.17
If a pathological fracture is encountered in a patient on ARVs, consider an endocrine workup, a DEXA scan and radiographs of weight-bearing or symptomatic long bones to assess potential fractures.
Orthopaedic surgeons should consider prophylactic fixation of long bones and use intramedullary fixation where possible. Always try to use an antegrade femoral nail and protect the femoral neck. Supplementary distal plating may be required in distal femur fractures. If there has been a very low energy fracture, then have a low threshold for prophylactic intramedullary fixation. Aim to stage procedures by two to three weeks. Multiple bone intramedullary nailing poses a high risk of blood loss and release of proinflammatory mediators such as IL-6, IL-10 and TNF-alpha.
At discharge, give vitamin D and calcium supplementation, and highlight the need to review ARV medications.
Conclusion
This case study demonstrates the far-reaching and debilitating effect of unmonitored TDF-induced osteomalacia and osteopaenia. While the mechanisms of pathophysiology are not yet fully understood, the presentation of this case, in conjunction with the available literature, suggests that the process is multifactorial and exacerbated by existing risk factors and comorbidities.
Patients on TDF must be screened for additional comorbidities and risk factors, especially concerning renal function, in order to amend their ARV regimen accordingly. Those with pathological fractures should be considered for endocrine workup, radiographs and a DEXA scan. It is advisable to use intramedullary fixation where possible.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. Prior to the commencement of the study ethical approval was obtained from the following ethical review board: Stellenbosch University Health Research Ethics Committee (C22/08/023).
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed written consent was obtained from the patient for being included in the study. Consent was obtained from the patient for the use of clinical photographs, and these images were adequately anonymised.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
MT: contributed to the study conceptualisation, design and manuscript preparation WDH: contributed to the study conceptualisation, design and manuscript preparation NF: contributed to the study conceptualisation, design and manuscript preparation
ORCID
Theron M https://orcid.org/0000-0003-4211-165X
Harrison WD https://orcid.org/0000-0003-4713-5239
Ferreira N https://orcid.org/0000-0002-0567-3373
References
1. Hajiani E, Parsi A, Seyedian S, et al. Comparing the frequency of osteoporosis and osteopenia in chronic hepatitis B patients with and without tenofovir treatment. Clin Epidemiology Glob Health. 2020;8(2):428-31. [ Links ]
2. Hamzah L, Tiraboschi J, Iveson H, et al. Effects on vitamin D, bone and the kidney of switching from fixed-dose tenofovir disoproxil fumarate/emtricitabine/efavirenz to darunavir/ ritonavir monotherapy: a randomized, controlled trial (MIDAS). Antivir Ther. 2015;21(4):287-96. [ Links ]
3. Gupta S, Yeh E, Kitch D, et al. Bone mineral density reductions after tenofovir disoproxil fumarate initiation and changes in phosphaturia: a secondary analysis of ACTG A5224s. J Antimicrob Chemother. 2017;72(7):2042-48. [ Links ]
4. Noe S, Heldwein S, Jaeger H, et al. Tenofovir disoproxil fumarate/emtricitabine is associated with a higher risk of hypocalcemia compared to abacavir/lamivudine - results from a German cohort study. Int J STD AIDS. 2019;30(5):447-52. [ Links ]
5. Emma E. Improved outcomes associated with an early mobilization protocol among hip and knee replacement patients [Internet]. HSRC. 2017 [cited 16 May 2022]. Available from: https://hsrc.himmelfarb.gwu.edu/son_dnp/1 [ Links ]
6. Patel P, Zulfiqar H. Reverse transcriptase inhibitors [Internet]. Ncbi.nlm.nih.gov. 2022 [cited 12 December 2021]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551504/ [ Links ]
7. Komatsu A, Ikeda A, Kikuchi A, et al. Osteoporosis-related fractures in HIV-infected patients receiving long-term tenofovir disoproxil fumarate: an observational cohort study. Drug Safety. 2018;41(9):843-48. [ Links ]
8. Wang Y, Huang X, Wu Y, et al. Increased risk of vitamin D deficiency among HIV-infected individuals: a systematic review and meta-analysis. Front Nutr. 2021;8. [ Links ]
9. Masiâ M, Padilla S, Robledano C, et al. Short communication: Early changes in parathyroid hormone concentrations in HIV-infected patients initiating antiretroviral therapy with tenofovir. AIDS Res Hum Retroviruses. 2012;28(3):242-46. [ Links ]
10. Keefe P, Bokhari S. Fanconi syndrome [Internet]. Ncbi.nlm.nih.gov. 2022 [cited 8 January 2022]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534872/ [ Links ]
11. Barbieri AM, Chiodini I, Ragni E, et al. Suppressive effects of tenofovir disoproxil fumarate, an antiretroviral prodrug, on mineralization and type II and type III sodium-dependent phosphate transporters expression in primary human osteoblasts. J Cell Biochem. 2018;119(6):4855-66. [ Links ]
12. Conesa Buendia F, Llamas Granda P, Larrañaga Vera A, et al. Tenofovir causes bone loss via decreased bone formation and increased bone resorption, which can be counteracted by dipyridamole in mice. J Bone Miner Res. 2019;34(5):923-38. [ Links ]
13. Osteomalacia: Case report and literature review [Internet]. Consultant360. 2019;59(9). [cited 16 December 2021]. Available from: https://www.consultant360.com/article/consultant360/osteomalacia-case-report-and-literature-review [ Links ]
14. Chu C, Pollock LC, Selwyn PA. HIV-associated complications: a systems-based approach. Am Fam Physician. 2017 Aug 1;96(3):161-69. PMID: 28762691. [ Links ]
15. Initiation of Antiretroviral Therapy | NIH [Internet]. Clinicalinfo.hiv.gov. 2022 [cited 9 May 2022]. Available from: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv/initiation-antiretroviral-therapy [ Links ]
16. Cazanave C, Dupon M, Lavignolle-Aurillac V, et al. Reduced bone mineral density in HIV-infected patients: prevalence and associated factors. AIDS. 2008;22(3):395-402. [ Links ]
17. Katzenstein T, Wessman M, Moseholm E, et al. Prevalence of low bone mineral density among people living with HIV. Cogent Medicine. 2021;8(1). [ Links ]
Received: November 2022
Accepted: January 2023
Published: August 2023
* Corresponding author: nferreira@sun.ac.za
Editor: Prof. Theo le Roux, University of Pretoria, Pretoria, South Africa
Copyright: © 2023 Theron M. This is an open-access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}
{kind=link}