










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.22 no.3 Centurion 2023
http://dx.doi.org/10.17159/2309-8309/2023/v22n3a2
HAND
3D-printed cable tie-assisted static progressive splints for fixed flexion contractures of the proximal phalangeal joint: a proof of concept study
Antoine RocherI, *; Megan O'ConnorI; Leonard C MaraisII
IDepartment of Orthopaedics, School of Clinical Medicine, University of KwaZulu-Natal, Inkosi Albert Luthuli Central Hospital, Durban, South Africa
IIDepartment of Orthopaedics, School of Clinical Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Proximal interphalangeal joint (PIPJ) contractures are common sequelae following trauma to the hand and represent a treatment impasse in South Africa's resource-constrained setting. Various splinting techniques are advocated for first line management, but there is no consensus on the optimal splint, and many studies report equivocal outcomes between modalities with only moderate improvements. This proof-of-concept study aimed to describe the design, production and use in a single case, of a 3D-printed splint, within an environment with limited access to therapy.
METHODS: The evolution in the design idea that yielded the final concept is described and a case in which the splint was used for a patient with a PIPJ flexion contracture, secondary to soft tissue trauma of a single finger, outlined.
RESULTS: The splint was designed using computer-assisted design (CAD) software, printed to custom-fit the patient, applied, and contracture improvement serially monitored. The PIPJ contracture was fully corrected and maintained at three months post cessation of splint use. No complications were experienced by the patient.
CONCLUSION: We describe a custom 3D-printed cable tie-assisted static progressive splint from conception to application to a patient. The patient had a 15° flexion contracture of his PIPJ which corrected uneventfully. Further investigation is warranted to determine applicability and safety of the splint for use among patients with PIPJ contractures of variable severity, chronicity and aetiology.
Level of evidence: Level 5
Keywords: 3D printing, static progressive splinting, proximal interphalangeal joint flexion contracture, proof of concept
Introduction
In South Africa, hand injuries account for one-third of all traumatic injuries seen in the state hospital setting.1 Proximal interphalangeal joint (PIPJ) injury is one of the most common injuries to the hand, and these injuries regularly complicate with flexion contracture and stiffness.2,3 The maximal joint volume is found at a position of 30-40° of flexion; this position is passively assumed by unsplinted patients to minimise the pain of capsular stretch from the increased pressure of inflammatory infiltrate influx.4 At this degree of flexion, the volar plate check rein ligament complex is slack, and so when fibrosis and scarring ensues in this shortened position, it results in limitation of extension.2,4
An incorrect splinting technique or prolonged immobilisation of unaffected fingers can similarly result in stiff PIPJs.5 It is suggested that immobilisation be maintained for no longer than three weeks, and that rehabilitation be initiated timeously to prevent complications.2 Rehabilitation, however, in the South African context is a challenge. Occupational therapists can obtain a postgraduate qualification in hand therapy at one of only three tertiary training facilities, restricting routine access to this specialised care.6 The constrained access, combined with the high caseload and rapid turnover, thwart the therapists' ability to perform the rigorous rehabilitation protocols required to prevent or later treat these deformities.6
The PIPJ is estimated to contribute 85% toward total grip strength, so pathology in the joint significantly limits function.4,7 Most patients tolerate up to 15° of flexion contracture without much functional deficit. A greater contracture, however, warrants treatment.8 Therapeutic modalities in the chronic setting, where the contracture is established, include splinting or operative management. There is no gold standard. Most studies report only modest improvement in range of motion and no studies report consistent return of full range of motion.2,9 Data does, however, suggest improved outcomes the earlier the intervention is initiated.2 Surgery is generally reserved for more severe cases. Studies in which surgery has been effective report patients committed to postoperative rehabilitation within 48 hours of surgery, a benchmark that we are not able to achieve in our setting.5 Most studies advocate for surgery only when no improvement occurs through nonoperative measures or in cases where bony involvement is established.9,10
Nonoperative treatment includes joint range of motion exercises, continuous passive motion, casting and splinting. Splints may be static, serial static, static progressive or dynamic.5 A systematic review by Young et al. compared the two splint types with the most favourable outcomes (static progressive and dynamic splints) and showed no significant difference in outcomes between the two.11 Dynamic splinting involves the application of an elastic material across the PIPJ to effect a constant passive extensive force. In contrast to static splints, static progressive splinting, popularised by Schultz-Johnson, involves maintaining the tension across the joint as the contracture is corrected by repeated changes of an adjustable component.12
Due to the resource limitations of prefabricated splints, splint materials and access to therapists in our setting, a 3D-printed static progressive splint with a cable tie for progressive correction was conceptualised for management of this common pathology. To our knowledge there have been no investigations into 3D-printed static progressive splints. This proof of concept study describes the novel design and production of the splint and reports its use in a patient to effect an improvement in a single PIPJ contracture.
Methods
The CARE clinical case report guidelines informed the writing of this study, as there are no present standards proposed for proof-of-concept studies.13
The final design presented resulted from an evolution in design ideas and material changes. Occupational therapists can fashion serial static splints from thermoplastic which is applied to the volar aspect of the PIPJ and conforms to the position of the contracted finger. This splint is reheated and set in a slightly more extended position at serial visits. The author's initial idea utilised the thermoplastic in a modified modular design which incorporated the novel use of a cable tie. The cable tie was positioned perpendicular to the lever arm of the contracture, to effect progressive correction. The use of a cable tie helped to maintain constant tension, was not susceptible to stretch like the Velcro® used in commercially available splints, and ensured the splint could be re-applied with the same tension as when it was removed. Velcro® designs offered no simple way to maintain the previous tension of the adjustable strap. It was also found that the thermoplastic often failed from the tortional force, or if it is strengthened by increasing the thickness, became unwieldly.
The emerging 3D-printing technology offered cheaper alternative thermoplastic materials such as polylactic acid (PLA). With access to CAD software and a 3D printer, the splint components could be custom designed and printed such that only the parts of the splint under greatest tortional forces were thick, limiting the overall bulkiness. The final design described incorporated both 3D-printed components and the novel cable tie mechanism.
The splint was applied to a 51-year-old male patient with a PIPJ contracture once consent for participation was obtained and an information document issued (Figure 1). Correction of the contracture was monitored initially at a one week follow-up and 37 megapascals (MPA) and is more robust than the traditional splinting plastics. Due to its biocompatibility, PLA is used extensively in implantable devices.14 Each component's print took approximately 60 minutes to complete and several splints of various sizes were printed to ensure an appropriate size match for the patient.

Application of the splint followed a stepwise process (Figure 1). Initially the proximal component was placed over the contracture. The 's'-shaped radial and ulnar aspects of the 'ring' of this component were designed to accommodate severe contracture. In such cases the patient would apply this component initially with the volar flange in a dorsal position, then they would apply a twisting motion passing around the PIPJ so the flange would come to lie on the volar side again. This would not be possible with a simple 'ring' design. The second component was then applied, with the half cylinder volar to the middle and distal phalanges. Finally, the cable tie was placed. The point was advanced through the slit on the dorsal outrigger of the proximal component, and then around the bridge of the distal component, and clicked through the cable tie head. The tie was then pulled to effect the extension moment which was perpendicular to the lever arm of the contracture. The tension was set initially at the point where the patient appreciated stretch but was not experiencing discomfort. The patient was advised to adjust the tie by a single daily click, or alternate day clicks depending on their experience of discomfort. The splint was worn for at least eight hours a day.
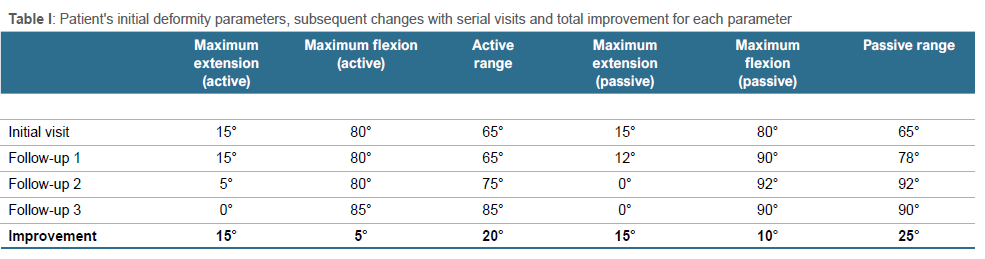
The patient presented with an inconvenient 15° flexion contracture of his right index finger PIPJ, six weeks after a hyperextension injury. After three weeks of using the static progressive splint, the deformity was corrected uneventfully (Table I). The patient continued using the splint as a static splint for another two weeks then at two weekly intervals until full correction was obtained. The final follow-up was telephonic, at three months from splint removal.
Results
The author used a CAD software, Fusion 360 (© 2020 Autodesk Inc.) to design the two components of the splint (Figure 2). The first component was designed to fit securely around the proximal aspect of the proximal phalanx. A volar flange was designed to extend proximal to the metacarpophalangeal joint to provide counter-pressure to the flexion moment of the long dorsal outrigger, the distal aspect of which would be the fulcrum through which the cable tie could exert the extension force for the progressive correction. The second component was designed as a lengthwise bisected cylinder, the distal aspect of which was circular in shape to conform to the fingertip. The length of this second component was designed to cross the distal interphalangeal joint (DIPJ), so that the extension force would be applied to both phalanges and the DIPJ as a unit (via the dorsally placed bridge), to mitigate the risk of developing a Boutonnière contracture. The design utilised scalable variables for the component's diameters and outrigger length, as opposed fixed values, allowing customisation for the individual patient.
The component designs were then converted into a 3D-printable version with Ultimaker Cura 4.8 slicing software (© 2011-2021 Ultimaker BV), an open-source product downloadable for use on both iOS and Microsoft operating systems. Printing was performed with the Creality CR10S Pro Printer (© 2021, Creality 3D) utilising 1.7 mm PLA filament. PLA is an inexpensive (between R3 and R5 per component in this case), non-toxic, thermoplastic, cornstarch-derived and biodegradable polyester. It has a tensile strength of to maintain the correction. Figure 3 demonstrates the initial flexion contracture and the correction with and without the splint.
Discussion
The idea of a 3D-printed cable tie-assisted static progressive splint was born out of necessity. PIPJ contractures encountered in the author's practice presented a management quandary. Access to surgical time was limited, there were no prefabricated splint options and access to therapists with the skill to produce static progressive splints inadequate. This led to conceptualisation of a splint that could be designed using previously acquired CAD skills and printed with the author's personal entry-level desktop 3D printer (purchased for about R10 000). It was cheap to make, able to effect the desired correction without involvement of a therapist and was tolerated by a patient. The splint can be reproduced with a low-end 3D printer and access to the .stl file. This study described the design, printing, application and ability of the splint to correct the soft tissue contracture in a single patient with no complication. The clinical application of this design still has to be investigated.
3D printers are advantageous in the context of prototyping and manufacturing unique objects, such as patient-specific implants.15,16 Unlike traditional manufacturing methods, the complexity of the 3D-print process is unchanged; regardless of the elaborateness of design, the prints can be easily scaled to different sizes, and a 3D printer has the capability to produce innumerable designs.16 Desktop 3D printers that print in plastic are more accessible than they were ten years ago, and there are many open-source software applications available for designing and conversion into printable files.17,18 While the design and conversion of the design to a printable format represent a significant learning curve, the printable '*.stl' format file can easily be shared for replication at the point of care should a 3D printer be available.17 Online 3D-printing communities such as www.thingiverse.com are another way to access open-source shared print designs and ideas. Customisation for individual patients can then be achieved by adjusting the print size on the open-source software, or alternatively, varying design size files can be shared.
Several studies have demonstrated benefit from 3D splints. Wang et al. reported on 13 stroke victims who had custom 3D fingerboards designed and fitted for their muscle spasm. These patients displayed improved range of motion and minimal complications.19 A case series of burn victims with finger contractures treated with 3D-printed static (non-progressive) splints found them to be of lower cost and faster fabrication than those standardly used to treat burn patients.20 Similarly, the single patient in our study managed with a static progressive 3D-printed splint, had a favourable outcome with full correction of his deformity and no complications as a result of the use of the splint. The reproducible design can be shared with other centres that have 3D printers, in consideration of further investigation of splint efficacy.
Conclusion
A customised 3D-printed cable tie-assisted static progressive splint was designed, 3D printed, and applied to a patient. The splint corrected the patient's PIPJ soft-tissue contracture without complication. Further investigation is warranted to determine applicability of the splint for use among patients with PIPJ contracture of variable severity, chronicity and aetiology.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. The study complied with the South African Department of Health ethics guidelines (2015), and the University of KwaZulu-Natal policy on research ethics. Prior to commencement of this research the appropriate ethical approval was obtained from the Biomedical Research Ethics Committee of UKZN (BREC/00002150/2020). The patient discussed in the report gave express permission for a publication to include non-identifying demographic information and the use of clinical photographs.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
AR: conceptualisation of splint, literature review, data capture, draft manuscript review and revision
MOC: study design, manuscript preparation and revision
LCM: study conceptualisation, expert manuscript review and revision
ORCID
Rocher A https://orcid.org/0000-0002-9710-5591
O'Connor M https://orcid.org/0000-0001-8864-4916
Marais LC https://orcid.org/0000-0002-1120-8419
References
1. Stewart A, Biddulph G, Firth GB. The aetiology of acute traumatic occupational hand injuries seen at a South African state hospital. SA Orthop J. 2017;16:49-53. https://doi.org/10.17159/2309-8309/2017/v16n4a8 [ Links ]
2. Kamnerdnakta S, Huetteman HE, Chung KC. Complications of proximal interphalangeal joint injuries: prevention and treatment. Hand Clin. 2018;34:267-88. https://doi.org/10.1016/j.hcl.2017.12.014 [ Links ]
3. Tocco S, Pedrazzini A, Pogliacomi F. Clinical approach in PIPj flexion contracture conservative treatment: our experience. Acta Biomed. 2016;87(Suppl 1):101-111. [ Links ]
4. Houshian S, Jing SS, Chikkamuniyappa C, et al. Management of posttraumatic proximal interphalangealjoint contracture. J Hand Surg Am. 2013;38:1651-58. https://doi.org/10.1016/j.jhsa.2013.03.014 [ Links ]
5. Yang G, McGlinn EP, Chung KC. Management of the stiff finger: evidence and outcomes. Clin Plast Surg. 2014;41:501-512. https://doi.org/10.1016/j..cps.2014.03.011 [ Links ]
6. De Klerk S, Badenhorst E, Buttle A, et al. Occupation-based hand therapy in South Africa: challenges and opportunities. S Afr J Occup Ther. 2016;46:10-14. http://doi.org/http://dx.doi.org/10.17159/2310-3833/2016/v46n3a3 [ Links ]
7. Leibovic SJ, Bowers WH. Anatomy of the proximal interphalangeal joint. Hand Clin. 1994;10:169-78. [ Links ]
8. Mangelson JJ, Stern P, Abzug JM, et al. Complications following dislocations of the proximal interphalangeal joint. J Bone Joint Surg Am. 2013;95:1326-32. [ Links ]
9. Tuffaha SH, Lee WPA. Treatment of proximal interphalangeal joint contracture. Hand Clin. 2018;34:229-35. https://doi.org/10.1016/j.hcl.2017.12.012 [ Links ]
10. Weeks PM, Wray RC, Jr, Kuxhaus M. The results of non-operative management of stiff joints in the hand. Plast Reconstr Surg. 1978;61:58-63. https://doi.org/10.1097/00006534-197801000-00010 [ Links ]
11. Young N, Terrington N, Francis D, et al. Orthotic management of fixed flexion deformity of the proximal interphalangeal joint following traumatic injury: A systematic review. Hong Kong J Occup Ther. 2018;31:3-13. https://doi.org/10.1177/1569186118764067 [ Links ]
12. Schultz-Johnson K. Static progressive splinting. J Hand Ther. 2002;15:163-78. [ Links ]
13. Gagnier JJ, Kienle G, Altman DG, et al. The CARE guidelines: consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013;2013:bcr2013201554. https://doi.org/10.1136/bcr-2013-201554 [ Links ]
14. Arefin AME, Khatri NR, Kulkarni N, Egan PF. Polymer 3D printing review: materials, process, and design strategies for medical applications. Polymers 2021;13(9):1499. https://doi.org/10.3390/polym13091499 [ Links ]
15. Waldburger L, Schaller R, Furthmuller C, et al. 3D-printed hand splints versus thermoplastic splints: a randomized controlled pilot feasibility trial. Int J Bioprint 2022;8:474. 20211202. https://doi.org/10.18063/ijb.v8i1.474 [ Links ]
16. Pereira T, Kennedy JV, Potgieter J. A comparison of traditional manufacturing vs additive manufacturing, the best method for the job. Procedia Manufacturing 2019;30:11-18. https://doi.org/10.1016/j.promfg.2019.02.003 [ Links ]
17. Meyer-Szary J, Luis MS, Mikulski S, et al. The role of 3D printing in planning complex medical procedures and training of medical professionals: cross-sectional multispecialty review. Int J Environ Res Public Health. 2022;19:3331. [ Links ]
18. Antreas K, Piromalis D. Employing a low-cost desktop 3D printer: challenges, and how to overcome them by tuning key process parameters. Int J Mech Appl. 2021;10:11-19. [ Links ]
19. Wang K, Shi Y, He W, et al. The research on 3D printing fingerboard and the initial application on cerebral stroke patient's hand spasm. Biomed Eng Online. 2018;17:92. 2018/06/27. https://doi.org/10.1186/s12938-018-0522-4 [ Links ]
20. Nam HS, Seo CH, Joo SY, et al. The application of three-dimensional printed finger splints for post hand burn patients: a case series investigation. Ann Rehabil Med. 2018;42:634-38. 2018/09/06. https://doi.org/10.5535/arm.2018.42.4.634 [ Links ]
Received: April 2022
Accepted: March 2023
Published: August 2023
* Corresponding author: rocher@ukzn.ac.za
Editor: Dr Duncan McGuire, University of Cape Town, Cape Town, South Africa
Copyright: © 2023 Rocher A. This is an open-access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Funding: The author personally funded the purchase of the 3-D printer and materials required to fabricate the splint. There was no external funding received for the project.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}
{kind=link}
{kind=link}