










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.22 no.3 Centurion 2023
http://dx.doi.org/10.17159/2309-8309/2023/v22n3a1
LETTER TO THE EDITOR
Orthopaedic surgery training in a post COVID-19 era: a Smith & Nephew travelling fellow perspective
Sven StrydomI, *; Philani NtombelaII
IDepartment of Orthopaedics, University of Pretoria, Kalafong Tertiary Hospital, Pretoria, South Africa
IIDepartment of Orthopaedics, University of the Witwatersrand, Johannesburg, South Africa
A global cause for concern
The first case of COVID-19 was reported in December 2019, and shortly thereafter, the World Health Organization declared it a worldwide pandemic by March 2020.1 The effects of the pandemic on healthcare systems and its subsequent quarantine provisions posed significant challenges to teaching institutions and clinical training worldwide.
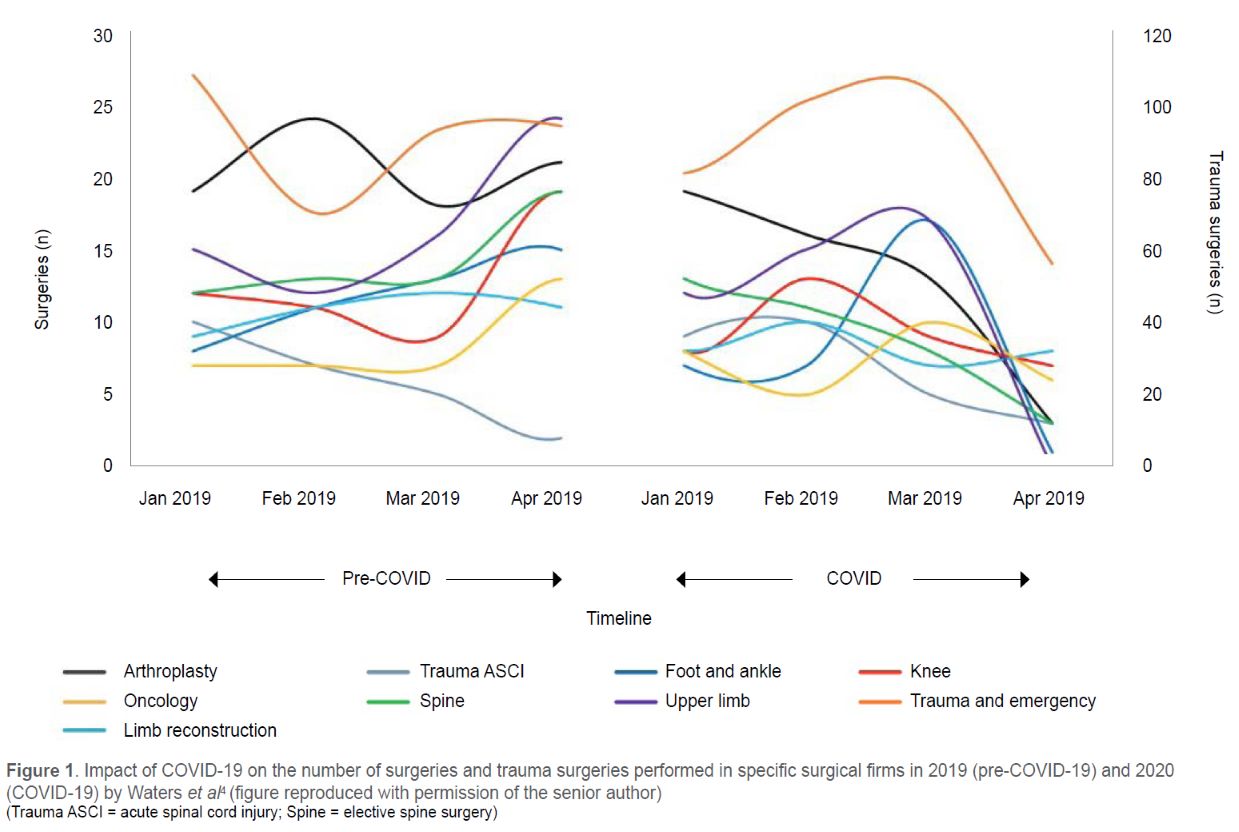
A big concern has been the impact on the training of orthopaedic surgeons worldwide, and lockdown periods resulted in elective lists being significantly reduced or cancelled.2-5 Even countries with no official lockdown period, such as Sweden, reported a 54% drop in elective joint replacement surgery rate during the first wave of COVID-19.2 Most countries, including South Africa, also reported a decrease in trauma cases.3,4 In the UK, this resulted in an 86% reduction in theatre time for orthopaedic trainees.3 In South Africa, a drastic decrease in elective and trauma surgeries performed in tertiary hospitals was noted in various orthopaedic subspecialty firms, as Waters et al. showed in Figure 1.4 This supports the similar reduction in theatre exposure indicated by Botha et al. in a separate single-centre study in South Africa.5
Doctors were also redeployed to assist in treating COVID-19 patients, with between 20% and 50% of orthopaedic trainees diverted to medical and ICU services unrelated to orthopaedic surgery training.2,3 Locally, even more (65.7%) surgical registrars were removed from their field of study.5 Treatment practices also changed in certain regions to limit the time spent in theatre. This ranged from a shift to conservative treatment of cases which would under normal circumstances have been treated surgically to consultants performing cases which would otherwise have been a cutting opportunity for a registrar.3
Internationally there was a move towards virtual training methods. The number of educational webinars, both local and international, increased to help with training. However, concerns were raised about its limitations in practical-based training and the acquisition of clinical skills. A study evaluating the effect of this sudden change in curriculum delivery in a postgraduate chiropractic course compared the test scores of two groups, comparing theory and practical test scores. They demonstrated that the group who received online teaching scored higher on the theory test but lower on their practical examination. This group was found to be unprepared and lacked the hands-on clinical experience to put theoretical knowledge into practice.6 Globally it was also noted that satisfaction with virtual training has been significantly lower than with traditional teaching methods in orthopaedic surgery.2
Worldwide, both the reduction in clinical exposure and the initial lockdown policies caused several institutions and individuals to postpone their final exams or to extend their training.3 The Colleges of Medicine of South Africa (CMSA) postponed the 2020 first semester clinical exam while cancelling the 2020 second semester exam.
Despite these considerations and adaptations to training, a global survey found that 58.6% of orthopaedic trainee respondents felt that their surgical training was severely hindered and that one in four hoped to have one additional year of training to meet their needs and training goals.2
The local experience
We were fortunate to be selected as the Smith & Nephew travelling fellows for 2023, the first group to travel after the last remaining COVID-19 restriction had been lifted in South Africa. We were both registrars before and during the COVID-19 pandemic and experienced the uncertainty and subsequent changes in how we were taught and later examined. Early in our tour, we realised that all the universities had to adapt their training programmes to various degrees and that the new adaptations were not without challenges.
In our attempt to objectively analyse this unprecedented situation, we endeavoured to ask the following three questions at each university of both consultants and registrars we met on our tour:
1. How did their training change during the COVID-19 pandemic?
2. Did any registrars choose to postpone writing their final exam?
3. Have any of the teaching platforms/methods implemented during the COVID-19 pandemic remained?
Changes in training
With the limitations placed on personal contact, all the departments followed the global trend of virtual meetings but differed in their implementation. The first challenge to be identified was the lack of communications infrastructure in most of the units. Thus, money and time were needed to set up the systems before teaching could resume. Even then, many registrars mentioned that the teaching sessions felt less beneficial compared to in-person sessions, stating reasons from lost connections, poor audio at times and the difficulty for consultants to describe or highlight areas of interest on X-rays. Despite most departments attempting to be completely virtual, some only used the virtual platform to limit the number of people physically in the room. This allowed only senior registrars and the firm hosting the session to be present, while the more junior registrars attended virtually.
The start of informal online small group discussions, usually with participants in the comfort of their own homes, was a welcome addition for most registrars. The increase in time that could be spent with family in an already rigorous training programme such as orthopaedics was reported by some registrars to reduce the feelings of burnout and stress.
Clinical and theatre exposure appears to have been reduced across all the departments following the cancellation of elective lists for several weeks to months at a time. Despite several departments claiming that clinics still exposed registrars to a wide variety of pathology, the reduction in theatre access has left some registrars nearing the end of their training feeling less prepared than they had aimed to be. Only a few departments have access to virtual reality training modalities to help registrars practise the surgical steps. Although this cannot replace real-time surgical experience, it could aid registrars in shortening their learning curve with procedures such as hip or knee arthroplasty, given the limited elective lists available.
The volume of COVID-19 patients also resulted in most departments having to 'donate' doctors to help treat these patients. Some departments opted to send people for a few days and then swap them out, which made it difficult to stay in an orthopaedic-focus routine. The alternative was to send someone for an entire month, which meant a longer orthopaedic work exposure missed but with fewer interruptions.
Postponing exams
Despite the abrupt changes in the training programmes and reduced theatre exposure at all the universities, it seems none of the registrars opted to postpone writing their final exams. Several reasons were mentioned, and it seems multiple factors contributed to this trend. It was mentioned that the time that would have been spent in theatre and clinics was now spent on reading and studying for the written component of the final exams, which most of the registrars consider the most challenging component of the exams. Secondly, the decision by the CMSA to postpone the exams during lockdown left many registrars with extra study time. Thus, they believed they could adequately prepare for this component of the exam.
A number of registrars have made arrangements to spend additional time in units/sub-specialities which interest them after their exams in an attempt to bolster their clinical skills before moving to other opportunities in state or private settings. Certainly, the value of a fellowship or mentor-mentee arrangements after graduating has become more apparent.
Post COVID-19 pandemic teaching
As COVID-19 eventually became less severe and restrictions began to lift, all the departments made great strides to maximise the training of their registrars. However, it seems that no amount of virtual training can fully substitute for in-person training, which has always been a cornerstone in surgical training programmes. For departments/satellite hospitals separated physically by long distances at Wits, UCT and KZN, some form of hybrid meeting is still being offered to improve the attendance of academic discussions. The remainder of the institutions have abandoned the virtual meetings and teaching methods and returned to in-person meetings only. However, some registrars have expressed disappointment at the cessation of the small group discussions, which could be done from home.
The change in exam format that followed the COVID-19 pandemic does, however, appear to have been met with positive feedback. The single-best-answer (SBAs) papers and short-answer questions are ideally suited for computer-based exams and were welcome changes to the written component as registrars felt that it broadened the spectrum of the exam. Most registrars who attended the online oral component stated that it felt less intimidating than the in-person examination. The ability to standardise the patients/ cases is also providing a feeling of fairness and equality, which aids registrars in managing the stress load experienced during the final exams.
A final reflection
Even though orthopaedic surgery as a speciality was not directly involved in the frontlines of treating COVID-19, there is no denying that our field and the training have been affected. While most of us were able to adjust to the 'new' normal, the journey was not easy, and the fear remains that we may have left some of our colleagues and friends behind while trying to finish the already stressful road to becoming a specialist.
With all the challenges imposed by the pandemic, it also presented some opportunities. Institutions were forced to develop communications infrastructure and now have it available when needed. While some institutions still utilise hybrid meetings with a positive effect on attendance rates, considering how few of the departments we visited kept any virtual teaching modalities they solely relied on for teaching during the COVID-19 pandemic, one cannot help but wonder how effective the training was.
Unfortunately, registrars were exposed to fewer educational opportunities during the COVID-19 pandemic. It may be several years before we fully appreciate the effect of this disruption on the training of orthopaedic surgeons. Each of us who trained during this period will need to reflect on possible skills and experience that may be lacking and actively try to fill the gaps, yet this group should not have to bear the burden alone. This period only highlighted the importance of teaching institutions, both locally and abroad, to bolster their training systems to continue to produce competent and skilled orthopaedic surgeons. Endeavours such as mentor-mentee programmes and fellowships, especially local opportunities, are becoming more crucial for us as a profession to continue to grow and develop.
ORCID
Strydom S https://orcid.org/0000-0002-6288-4388
Ntombela P https://orcid.org/0000-0002-4301-1899
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727-33. http://dx.doi.org/10.1056/NEJMoa2001017 [ Links ]
2. Hsu C-H, Huang H-T, Chen C-H, et al. Global impact of the COVID-19 pandemic on orthopedics and the implications of telemedicine: A systematic review of the literature. J Clin Med. 2022;11(11):2983. http://dx.doi.org/10.3390/jcm11112983 [ Links ]
3. Abdelazeem AH, Khedr AM, Scarlat MM. Orthopaedic training during COVID-19 pandemic: Should action be taken? Int Orthop. 2022;46(2):159-64. http://dx.doi.org/10.1007/s00264-022-05307-2 [ Links ]
4. Waters R, Dey R, Laubscher M, et al. Drastic reduction of orthopaedic services at an Urban Tertiary Hospital in South Africa during COVID-19: Lessons for the future response to the pandemic. S Afr Med J. 2021;111(3):240. http://dx.doi.org/10.7196/SAMJ.2021.v111i3.15263 [ Links ]
5. Botha R, Cardoso JH, Lombard A, et al. Surgical training during the COVID-19 pandemic - a single institution's trainee survey. S Afr J Surg. 2022;60(1):40-43. http://dx.doi.org/10.17159/2078-5151/2022/v60n1a3604 [ Links ]
6. Frutiger M, Whillier S. Effects of a sudden change in curriculum delivery mode in postgraduate clinical studies, following the COVID-19 pandemic. J Chiropr Educ. 2022;36(2):132-41. http://dx.doi.org/10.7899/JCE-21-31 [ Links ]
* Corresponding author: svenstrydom@gmail.com


{kind=link}