










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.22 n.1 Centurion 2023
http://dx.doi.org/10.17159/2309-8309/2023/v22n1a6
CURRENT CONCEPTS REVIEW
Intertrochanteric femur fractures: a current concepts review
Falethu M SukatiI, *; Jaco ViljoenII; Alwich AlexanderIII
ITrauma and Spine Units, Department of Orthopaedics, Steve Biko Academic Hospital, University of Pretoria, Pretoria, South Africa
IITrauma and Tumour Limb Reconstruction and Sepsis Units, Department of Orthopaedics, Steve Biko Academic Hospital, University of Pretoria, Pretoria, South Africa
IIITrauma and Foot Units, Department of Orthopaedics, Steve Biko Academic Hospital, University of Pretoria, Pretoria, South Africa
ABSTRACT
Intertrochanteric fractures are common injuries around the hip, especially among the elderly. With the rising incidence of these injuries, they are expected to double by 2050. Incidence rates are higher in females than males and in white patients than black African patients. Osteoporosis weakens the local trochanteric anatomic support leading to an increased susceptibility to fractures. Disruption of the posteromedial calcar region results in fracture instability. Optimal lag screw position and fracture reduction are significant determinants for postoperative outcomes. The tip apex distance and reduction criteria determine lag screw cut-out risk and fracture reduction quality, respectively. A calcar-referenced tip apex distance is comparable if not better than the tip apex distance in predicting cut-out risk. Optimal reduction is in slight valgus, a positive medial cortex apposition and smooth anterior cortex apposition.
High mortality rates are observed with non-surgical treatment. Surgical management is therefore the gold standard for intertrochanteric fractures. Treatment options are categorised into extramedullary fixation, intramedullary fixation and proximal femur replacement. They include the dynamic hip screw (DHS), cephalomedullary nails (CMN) and arthroplasty. Although still in use, the proximal femur locking plate is falling out of favour due to high complication rates. Fracture stability and pattern influence the treatment choice. There is, however, a growing use of CMNs which has been attributed to surgical training background. Modification of older CMN designs has improved treatment outcomes. Systematic meta-analyses of randomised controlled trials (RCTs) do not show superiority of one treatment option over another; therefore, there is no consensus on the best treatment choice.
The proximal femur nail antirotation (PFNA) has better outcomes compared to other fixation options with respect to intraoperative blood loss and Harris hip scores. As a group, CMNs have a better 120-day postoperative quality of life compared to the DHS. No significant difference in complications has been found between treatment options. In light of the anticipated increased incidence of intertrochanteric fracture, more work is needed in planning national resource allocation, devising preventative methods and improving clinical interventions in South Africa.
Level of evidence: Level 5
Keywords: intertrochanteric femur fracture, dynamic hip screw, cephalomedullary nail, arthroplasty
Introduction
The intertrochanteric region is defined as the extracapsular portion of the proximal femur between the intertrochanteric line and a horizontal line at the lower end of the lesser trochanter.1 The fractures occur due to high or low energy trauma, the latter being common in patients with osteoporotic bone. With the use of computed tomography (CT) scans, understanding of intertrochanteric fracture patterns and management thereof has improved. In this paper we review the current knowledge on this injury, its management options and outcomes, and relate these to the South African context.
Epidemiology
Intertrochanteric femur fractures have a bimodal distribution, occurring as high energy injuries in young adults and more commonly as low energy, osteoporotic fractures in elderly patients.2,3 Dela et al. recently reported a hip fracture incidence rate of 68.6 per 100 000 for the total South African population, with 87.5 and 46.2 per 100 000 for females and males, respectively.4 This represents a significant increase from the incidence rate of 5.6 per 100 000 reported by Solomon in 1968.5 Based on sex and ethnicity, the incidence rate for females was 175.9, 43.6, 73.2 and 147.7 in the white, black African, Coloured and Indian groups, respectively. For males the incidence rate was 76.5, 31.1, 39.7 and 69.2 in the white, black African, Coloured and Indian groups, respectively. Of note is the average age at fracture in that study was lower than in developed countries.4
Anatomical considerations
The intertrochanteric region is a well-vascularised region connecting the femoral neck with the diaphysis, and to fully understand the fixation of fractures in the intertrochanteric region, one needs to be cognisant of the alignment of the femoral neck to the shaft. In the coronal plane, the neck shaft angle of a normal adult ranges from 120° to 135°. In the transverse plane, alignment of the femoral neck to shaft is 10° to 15° of anteversion relative to the femoral condyles. The intertrochanteric region is highly dependent on the structural integrity of a cancellous bony arcade, stretching from the femoral head to the lesser trochanter where the solid nature of this area transitions to the tubular femoral canal.6 The vertical column originates in the lower medial femoral neck and ascends vertically into the femoral head and conveys compression forces.7 The horizontal column originates at a bony buttress in the inner anterior upper femoral shaft from which it extends horizontally towards the anterior aspect of the femoral head, conveying tension force.7 The calcar and beams of bone trabeculae (compression, tension, oblique/secondary compression) form a loading system-truss system.8 The calcar is a vertical plate composed of multiple layers of compact bone, typically no thicker than 1 mm, which is situated deep to the lesser trochanter but posterior to the neutral axis of the femoral neck.9 It contributes to the strength of the femoral neck and can bear compressive load, redistributing the load from the femoral head to the proximal femur shaft. During single limb stance, the proximal femur simultaneously bears bending and torsional moment and the femur grows to adapt to these mechanical requirements.9 The posteromedial lesser trochanter calcar fragment frequently extends to the posterior cortex.7,8 Disruption of the calcar results in decreased efficiency in transforming bending and torque moments, affecting the stress pattern in the proximal femur and thus rendering fractures that involve this portion of the proximal femur unstable.9,10
Technical and surgical factors
Reduction
Baumgaertner and colleagues proposed what is currently the most widely used criteria for assessing the risk for failure of fixation.11 More recently Chang et al. proposed criteria for assessing the quality of fracture reduction between the head-neck fragment and femur shaft. The point-based system categorises a reduction as good, acceptable or poor.12 A good intertrochanteric reduction has a normal or slight valgus alignment and positive medial apposition on the anteroposterior (AP) X-ray view. On a lateral view, there is central axial alignment with smooth anterior cortex contact. Medial displacement > 4 mm of any fragment on AP and angulation > 20° on lateral view are not acceptable. The maximum cortical thickness is 4 mm, therefore a reduction with < 4 mm translation ensures cortical contact. A reduction is considered acceptable when it meets either the alignment or displacement criteria. A poor reduction does not meet any of the criteria.12
Poor reduction quality and loss of medial wall support are independent factors for implant failure.13 Application of a circumferential cerclage cable after intramedullary fixation of reverse oblique intertrochanteric fractures reduces the risk of implant failure.14,15 The quantity and range of the posteromedial fragment significantly correlates with postoperative telescoping and varus collapse of the femoral head and neck component.2
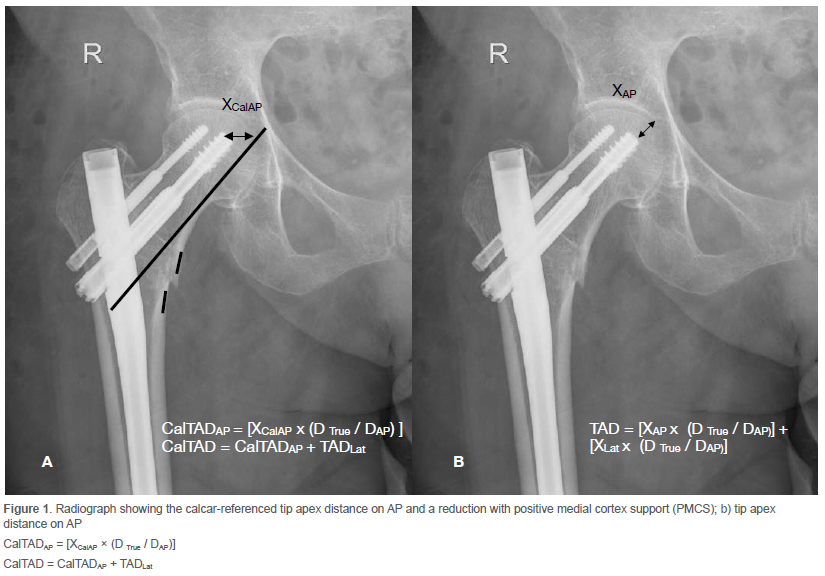
Anteromedial cortical support reduction for unstable intertrochanteric fractures introduced by Chang and colleagues in 2015 is an extension of the nonanatomic positive cortex buttress concept by Gotfried et al.12,16 This reduction aims at using the medial wall of the femur shaft fragment as a functional buttress for the medial cortex of the neck fragment. It enables a controlled fracture impaction leading to axial and torsional stability. The reduction is termed positive, neutral or negative depending on the anteromedial cortical alignment on AP and lateral views. If the head-neck fragment is medial on AP or anterior on lateral view to the shaft fragment, it is deemed positive reduction (Figure 1). A negative reduction arises when the head-neck fragment is lateral on AP or posterior on lateral view in relation to the shaft fragment. The ideal reduction is positive on both AP and lateral views. Chang's group further combined their concept with that of Baumgaetner's group to develop a postoperative stability scoring system.17
TAD and Cal-TAD
Optimal position of the lag screw has been defined by various methods, one of which is the tip-apex distance (TAD) introduced by Baumgaetner and colleagues in 1995.11 Other methods used to assess the position of the cephalic fixation are the Cleveland zone system, Parker's ratio index and calcar-referenced tip-apex distance (CalTAD). The Cleveland zone system and Parker's ratio index effectively illustrate the location of the cephalic fixation in relation to the rest of the head by assigning it to a zone or calculating a ratio. The TAD measures the depth of the cephalic fixation. By referencing the TAD to the calcar, the CalTAD combines illustration of the cephalic fixation location with measurement of its depth.18 The first component of the CalTAD is measured in the anteroposterior radiograph using a line drawn adjacent to the femoral calcar and parallel to the neck axis. The second component is measured on the lateral view and is similar to that of the TAD as shown in Figure 1.19
The risk of cut-out is influenced by the quality of intraoperative reduction, positioning of the screw in the femoral head and the type of fracture. In biaxial cepalomedullary nail fixation, the calcar-referenced TAD is a better predictor for cut-out than the TAD.20 Regarding CalTAD, although there was a tendency for more failure with CalTAD > 25 mm (p = 0.06) and even with CalTAD > 20 mm (p = 0.07), this difference did not reach statistical significance (p = 0.05). In light of the finding by Lopes-Coutinho et al., the femur head size is an important factor.21
In the biomechanical study by Kane et al., no significant difference was found in screw placement between the centre-centre and low-centre positions. However, it must be noted that the study was powered to detect a 20% difference in the magnitude of loading cycles or fracture translation between treatment groups. Even though the results did not show statistical significance, the low-centre position consistently had better results. Based on kinematic evaluation, the authors then inferred that the low-centre position may provide a more stable fixation than the centre-centre position.22 Lopes-Coutinho et al. did not explore the influence of implant choice, which may have influenced their findings.21 As the nail is driven deeper in the shaft to achieve a low-centre position for the cephalic screw, there is a risk of lateralising the proximal end of the nail. This can lower the integrity of the lateral wall and precipitate varus collapse. The same proximal valgus angulation of the nail can also result in vulgarisation of the neck-shaft angle in patients with stronger bone, thus conferring an advantage.
By combining the illustration of cephalic fixation location with depth measurement, the CalTAD becomes a better predictor of implant failure as shown by Yang et al.18 In this study on intertrochanteric fractures in geriatric patients fixed with cephalomedullary nails, they found no significant difference between the failure and non-failure groups for the Cleveland zone system, and Parker's ratio index in the univariate and multivariate analysis. For the TAD, significant differences were found in univariate analysis but not multivariate analysis. The CalTAD showed significant differences in both univariate and multivariate analysis. Furthermore, it showed an almost perfect interclass correlation coefficient. They therefore concluded that among the tools for measuring cephalic fixation position, the CalTAD is the only significant predictor for implant failure in geriatric intertrochanteric fractures with cephalomedullary nail (CMN) fixation.18 These findings are similar to those of Kashinga et al., whose study was not limited to geriatric patients.23
The TAD is still considered a reliable predictor for screw cut-out. A lower value of 20 mm may be even better than the original value of 25 mm. The CalTAD is equally reliable if not better than the TAD.
Management options
Dynamic hip screw
The dynamic hip screw (DHS), also known as a sliding hip screw (SHS), has historically been considered the mainstay for fixing intertrochanteric fractures but some now consider cephalomedullary devices (CMDs) to be the gold standard.24 Fracture fixation with the DHS is recommended by the NICE guidelines for AO 31A1 and A2 fractures and AAOS for unstable intertrochanteric fractures.25,26 Both recommendations are not evidence-based as most meta-analyses have not shown superiority between the DHS and the intramedullary nail (IMN).27-31
A key factor for using the DHS is lateral wall integrity described as wall greater than 20.5 mm. Absence of an intact lateral wall renders intertrochanteric fractures unstable for management with a DHS. A DHS, through its angular construct, maintains the neck shaft angle while the lag screw slide creates a compression force at the fracture site. Flattened sides of the lag screw limit rotational forces (Figure 2). An intact lateral wall acts as a buttress, limiting further lateral displacement. Addition of an antirotation screw reduces lag screw migration and cut-out.32

Advantages of the DHS are cost effectiveness, fracture stability, an option to add a trochanteric stabilisation plate, and early mobilisation of patients. Disadvantages are its limited use to stable fractures and more prominent hardware that may need removal later.
Proximal femur locking plate
The proximal femur locking plate (PFLP) is another extramedullary device for intertrochanteric fracture fixation (Figure 3). It is a fixed-angle, static construct and the plate offers lateral wall buttress. A precontoured design enables anatomical reduction and fixation against the plate, and the convergent proximal locking screws enhance fixation stability (Figure 4).33 Advantages versus the DHS in unstable fractures are that it can address complications like shortening, medialisation of the distal fragment, implant cut-out, lateralisation of proximal fragment and varus collapse. Adductor muscle pull tends to medially displace the distal fragment in unstable intertrochanteric fractures and a PFLP resists this deforming force. The locking mechanism in a PFLP creates a non-collapsing implant which overcomes the forces that otherwise develop at the screw-plate junction in a DHS with coaxial collapse of the proximal fragment. Bone preservation is an important factor for fracture union, and the PFLP is superior to the DHS in this respect owing to the smaller screw size.34


Compared to CMNs the PFLP is better at keeping free bone fragments in the greater trochanter together. In such patterns the lateral trochanteric wall usually shatters, and cleavage occurs in the coronal plane. Furthermore, insertion of an IMN may worsen the instability through additional lateral wall damage.35
Indications for the PFLP are limited, e.g. unstable intertrochanteric (IT) fractures in patients with a narrow femoral canal. Some surgeons use it for patients with reverse oblique fractures and those exiting at the greater trochanter thereby compromising nail entry. Poorly defined indications and application beyond the limits contribute to high failure rates. Application of the PFLP may be justified for its superior abilities to restore and maintain anatomy. This especially holds true for a younger subgroup of patients. However, if anatomical reduction is not achieved and patient compliance is low, the use of a PFLP should be carefully weighed against other implants especially in unstable intertrochanteric or subtrochanteric fractures.33 Moreover the recent paper by Parker et al. concluded that unstable intertrochanteric fractures should not be treated with fixed/static plates. PFLP are therefore not the first choice in unstable intertrochanteric fractures.31,36
Cephalomedullary nails
The cephalomedullary nail (CMN) was introduced in the 1980s and its use over the years has increased. This increasing use of the CMN is higher among younger surgeons and is influenced by training, setting and postgraduate experience. However, it is not supported by literature as there is no superiority demonstrated between the CMN and DHS.27-31
CMNs resist the deforming forces in intertrochanteric fractures which otherwise lead to medialisation and varus collapse of the proximal fragment. The medullary placement of a CMN creates a buttress which resists medialisation, and the fixed angle construct helps in preservation of the neck-shaft angle. This is more important in unstable intertrochanteric fractures. In the treatment of unstable fractures, patients fixed with CMN are more likely to maintain reduction, avoid limb length discrepancy and fully weight bear earlier. The advantage of a CMN over DHS in improved mobility was demonstrated by Hardy as limited to the first three postoperative months in stable fractures and persisting to the twelfth month in unstable fractures.37
In studies that showed no superiority of CMN over DHS, the findings have been attributable by some authors to a failure to distinguish between stable and unstable fractures, differences in the general health of patients and variations in postoperative rehabilitation protocols.38 However, more recent Cochrane reviews have also found no superiority of CMN over fixed angle extramedullary devices like the DHS.39,40
Mismatch of radii of curvature between femur and nail is a known problem, with long femur nails commonly resulting in complications such as anterior cortical abutment, encroachment, erosion and penetration.41 Consideration of the anatomical variations led to the development of short nails and further modifications thereof.42 Modifications to the short nail have reduced the complication rate. Zhang et al. modified the short nail in three key areas. They changed the proximal diameter to 16.5 mm, introduced an anterior curve below the 4° valgus angle and fluted the distal 30 mm of the nail.43,44
Numerous studies have shown the superiority of short versus long nails with regard to reoperation rate, radiation exposure, estimated blood loss and operative time.43-45 With this background, there are still some scenarios where long nails are recommended. These include fractures with primary lateral wall rupture (AO 31 A3, with subtrochanteric extension (AO 31 A2.3), with wider proximal medullary canal, large coronal fractures of the lateral wall and revision for a short nail.17 Essentially the preference for long nails is in unstable fracture patterns where reduction is unlikely to be maintained with short nails.
Some recent studies have shown that short nails can be comparable with long nails in treating unstable fractures. In a biomechanical study Blum et al. found no significant difference in axial load to failure values between long and short IMN fixation in unstable intertrochanteric fracture patterns. Fractures fixed with short nails showed greater torsional stiffness than with long nails. They hypothesised that this was due to the shorter working length in short nails.45 Similarly Hulet et al. showed that there was no difference in overall complications between short and long CMN treatment for unstable intertrochanteric fractures.46 Once a decision is made to use a CMD, current evidence favours a short nail but surgeons should consider the factors listed above to judge if the reduction is likely to be lost.
Most of the studies comparing locked versus unlocked nails or static versus dynamic locking are based on short CMNs, the mean age of the study populations being over 70 years. In the biomechanical study by Lacroix, the addition of a distal screw led to a 35.7% decrease of the mean failure to load in torsion.47 The authors postulated that the drill holes acted as stress risers. In stable fractures a distal screw has no effect on the load distribution as shown by the lack of pattern in proximal femur strain pattern.48 This is due to the axial load being transferred from the trochanteric region to the femur cortex.
A few recently published meta-analyses have shown superior results in stable fractures for the unlocked nail with significant differences in operation time, fluoroscopy exposure time, blood loss and total incision length.49-51 There are differences in the complication profile between locked and unlocked nails. Distal locking is associated with iatrogenic fractures, thigh pain, vascular injury, delayed union and non-union. The most frequent among these is thigh pain.52 Lil et al. found distal locking in long nails to be associated with a gradual decrease in neck-shaft angle which led to varus collapse and construct failure in 21.4% of patients.53 The authors described how distal locking blocks migration of the nail, ultimately leading to a windshield effect of the cephalic screw and cut-out.
Significantly lower rates of thigh pain and other complications have been demonstrated with unlocked nails.51,54 Peri-implant fractures and anterior cortical impingement occur but are not unique to unlocked nails. Skála-Rosenbaum et al. found a higher peri-implant fracture rate in unlocked nails compared to dynamically locked nails for AO 31-A1 and A2 fractures. The authors described two types of fracture patterns, both of which can be attributed to surgical planning and/or technique errors.55 Techniques for eliminating these complications have been described. It is important to check for rotational instability. After placing the cephalic screw in rotationally stable fractures, the femur moves as one unit.51 Rotationally unstable fractures do better with distal locking.50 Stable trochanteric fractures can be adequately treated with distally unlocked nails.49-51,56-58
Another decision to be made when using a CMN is whether to use a mono- or biaxial lag screw device. Screw cut-out and migration of the proximal fragment are known complications for CMNs. The development of biaxial screws was aimed at improving these outcomes. Common devices available in the market are the InterTan for biaxial screws and the Gamma3 Nail for monoaxial screws. The InterTan shows less screw cut-out and migration compared to the Gamma3 Nail or PFNA. A meta-anaylsis by Nherera et al. found the InterTan had fewer complications, fewer revisions and fewer patients complaining of pain compared to the PFNA.59 However the meta-analysis by Ma et al. found the two to be comparable when assessing blood loss, revision rate, fluoroscopy time, union and length of hospital stay. Although they found lower cut-out and femur fracture rates with the Intertan, these did not translate to statistically significant lower revision rates.60 Current evidence therefore indicates that biaxial CMN has lower cut-out rates compared to monoaxial CMN but is equally comparable on other factors. Comparison between a lag screw and helical blade shows no difference in cut-out rate.61
Arthroplasty
Surgical stabilisation that quickly restores pre-injury mobilisation and avoids complications offers the ideal outcome in intertrochanteric fractures. At times internal fixation does not meet these goals. High failure rates due to fracture instability and osteoporosis with internal fixation have led others to consider arthroplasty as a treatment option. Numerous authors have shown that hemiarthroplasty (HA) and total hip arthroplasty (THA) are viable treatment options for unstable intertrochanteric fractures.62-64 However, meta-analysis of several randomised controlled studies have not demonstrated superiority of arthroplasty over internal fixation.65-67 The metaanalysis by Kumar et al. concluded that internal fixation with a proximal femur nail was superior to HA for management of AO/OTA A2 and A3 intertrochanteric femur fractures in the elderly.68 Interest in arthroplasty for intertrochanteric fractures has been low in the past partly due to low non-union and avascular necrosis rates after internal fixation. Currently there is an increasing interest. Patients who sustain intertrochanteric fractures with pre-existing significant hip osteoarthritis, rheumatoid arthritis or proximal femur and periacetabular pathological fractures may be better managed with arthroplasty.69 With recent meta-analysis studies favouring internal fixation with a proximal femur nail over arthroplasty for unstable intertrochanteric fractures, the latter should be used with caution in carefully selected patients.65-68 Furthermore, resource constraints must be considered in those countries where they are a significant factor.
Outcomes
Zha et al. proposed three requirements for an ideal internal fixation for intertrochanteric fracture: 1) femoral neck screw with at least three-dimensional structures of the fixed system; 2) minimal angle between the femoral neck screw axis and the femoral shaft and thus maximum alignment between the angle of normal hip joint weight-bearing line and the femoral graft axis (normally 25°); and 3) ability of the implant to prevent the rotation of the femoral head. Unfortunately, none of the currently used devices can fully meet these three criteria.70 Consequently implant-related complications arise. Cui et al. reported a pooled estimate of the one-year mortality rate at 17.47% after femoral intertrochanteric fracture and 9.83% after femoral neck fracture.71 These are still better than the mortality rate of 34.6% in conservatively treated intertrochanteric fractures.72
In the largest network meta-analysis to date, the PFNA was the most preferable surgical method with less blood loss and higher Harris hip score. This study included 36 RTCs and compared eight intramedullary and extramedullary internal fixation methods. The PFNA and Gamma nail had lower operative times than the DHS. No significant differences were found with respect to complications.73 Marks et al. found the 120-days postoperative quality of life significantly favoured the CMN over the SHS (DHS).74
Although arthroplasty has not proven to be superior to internal fixation, it still offers some benefits such as early postoperative weight bearing, a shorter hospital stay, and lower implant-related complications and reoperation rate.65,66 Internal fixation has shorter operative times and lower blood loss. Data on Harris hip scores and one-year mortality rate favour internal fixation in some studies and show no difference in others.
South African context
In 2021, the elderly (60+ years) were estimated to be at 5.51 million, 9.15% of the South African population. This is an increase from 4.89 million (8.5%) in 2018, in keeping with the improving life expectancy. The Eastern Cape has the highest proportion of elderly patients in South Africa (11.5%) and Gauteng has the second lowest at 8.5%.75 By 2050, it is predicted that the elderly will constitute 24.3% of the South African population, more than double the current numbers.76 High levels of income inequality in South Africa place more than half the population below the poverty line. Among this population there is a high level of communicable diseases (e.g. HIV/AIDS), protein calorie malnutrition and suboptimal daily calcium intake. These lead to low bone mineral density (BMD). On the other end of the economic spectrum, high alcohol use and smoking are significant contributors to a low BMD.4,77 All these factors will lead to a rise in fragility hip fractures.
A two-tiered healthcare system, higher urban distribution of orthopaedic surgeons, higher rural distribution of elderly patients and the absence of an event-based funding model in the public sector make delivery of optimal care for intertrochanteric fractures to the most affected patients difficult at a national level. Clinicians can still improve care at a more local level by developing units that are geared to handle these patients, e.g. an ortho-geriatrics unit as shown by Li et al.78 Furthermore costs can be reduced by as much as 18% without reduction of quality measures through the use of an algorithm for intertrochanteric fracture treatment.78 More work still needs to be done to understand local fracture patterns.
Conclusion
Operative management of intertrochanteric fractures is essential for optimal outcomes. Stable fractures can be managed by either a DHS or CMN, depending on surgical expertise and resources. There is currently no evidence favouring one option over the other. The PFLP should be avoided in these injuries. Unstable intertrochanteric fractures require a good understanding of the fracture pattern and careful implant selection for good outcomes. Available meta-analyses of randomised controlled trials (RCTs) have not shown superiority between the DHS and CMN or CMN and arthroplasty. CMNs have better outcomes compared to the DHS and arthroplasty with respect to operative time and blood loss. Similar outcomes have been shown for CMNs on Harris hip scores compared to the DHS and to a certain extent in arthroplasty. The lack of superiority for arthroplasty over CMNs and a more recent RCT showing superiority of the proximal femur nail over hemiarthroplasty further limit the use of arthroplasty as a surgical option for unstable intertrochanteric fractures.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
FMS: literature review, epidemiology, technical and surgical factors, dynamic hip screw, cephalomedullary nails, outcomes, South African context, first draft preparation, manuscript preparation JV: introduction, arthroplasty
AA: anatomical considerations, proximal femur locking plate
ORCID
Sukati FM https://orcid.org/0000-0002-1235-3597
Viljoen J https://orcid.org/0000-0002-8775-6913
Alexander A https://orcid.org/0000-0002-4023-7550
References
1. Parker MJ. Trochanteric hip fractures. In: Tornetta P III, editor. Rockwood and Green's fractures in adults. 9th ed. Philadelphia: Wolters Kluwer; 2020. p. 2285-317. [ Links ]
2. Ren H, Ao R, Wu L, et al. Effect of lesser trochanter posteromedial wall defect on the stability of femoral intertrochanteric fracture using 3D simulation. J Orthop Surg Res. 2020 Jul 3;15(1):242. https://doi.org/10.1186/s13018-020-01763-x [ Links ]
3. Tsabasvi M, Davey S, Temu R. Hip fracture pattern at a major Tanzanian referral hospital: focus on fragility hip fractures. Arch Osteoporos. 2017 Dec;12(1):47. [ Links ]
4. Dela SS, Paruk F, Brown SL, et al. Ethnic and gender-specific incidence rates for hip fractures in South Africa: A multi-centre study. Bone. 2020 Apr;133:115253. https://doi.org/10.1016/j.bone.2020.115253 [ Links ]
5. Solomon L. Osteoporosis and fracture of the femoral neck in the South African Bantu. J Bone Joint Surg Br. 1968 Feb;50(1):2-13. [ Links ]
6. Sheehan SE, Shyu JY, Weaver MJ, et al. Proximal femoral fractures: what the orthopedic surgeon wants to know. Radiographics. 2015;35(5):1563-84. [ Links ]
7. Le Corroller T, Dediu M, Pauly V, et al. The femoral calcar: a computed tomography anatomical study. Clin Anat. 2011 Oct;24(7):886-92. [ Links ]
8. Zhang Q, Chen W, Liu HJ, et al. The role of the calcar femorale in stress distribution in the proximal femur. Orthop Surg. 2009 Nov;1(4):311-16. [ Links ]
9. Hammer A. The calcar femorale: A new perspective. J Orthop Surg (Hong Kong). 2019 May-Aug;27(2):2309499019848778. [ Links ]
10. Cech O, Kostál R, Váchal J. [Unstable pertrochanteric fractures, biomechanic, classification and therapy]. Acta Chir Orthop Traumatol Cech. 2000;67(1):17-27. [Czech]. [ Links ]
11. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995 Jul;77(7):1058-64. [ Links ]
12. Chang SM, Zhang YQ, Ma Z, et al. Fracture reduction with positive medial cortical support: a key element in stability reconstruction for the unstable pertrochanteric hip fractures. Arch Orthop Trauma Surg. 2015 Jun;135(6):811-18. [ Links ]
13. Fan J, Xu X, Zhou F, et al. Risk factors for implant failure of intertrochanteric fractures with lateral femoral wall fracture after intramedullary nail fixation. Injury. 2021 Nov;52(11):3397-403. [ Links ]
14. Imerci A, Aydogan NH, Tosun K. The effect on outcomes of the application of circumferential cerclage cable following intramedullary nailing in reverse intertrochanteric femoral fractures. Eur J Orthop Surg Traumatol. 2019 May;29(4):835-42. [ Links ]
15. Hantouly AT, Salameh M, Toubasi AA, et al. The role of cerclage wiring in the management of subtrochanteric and reverse obliqueintertrochanteric fractures: a meta-analysis of comparative studies. Eur J Orthop Surg Traumatol. 2022. https://doi.org/10.1007/s00590-022-03240-z [ Links ]
16. Gotfried Y, Kovalenko S, Fuchs D. Nonanatomical reduction of displaced subcapital femoral fractures (Gotfried reduction). J Orthop Trauma. 2013 Nov;27(11):e254-9. [ Links ]
17. Chang SM, Hou ZY, Hu SJ, Du SC. Intertrochanteric femur fracture treatment in Asia: What we know and what the world can learn. Orthop Clin North Am. 2020 Apr;51(2):189-205. [ Links ]
18. Yang YF, Huang JW, Gao XS. CalTAD is the key evaluation tool for measurement of cephalic fixation position for predicting cut-out in geriatric intertrochanteric fracture patients with internal fixations after achieving acceptable reduction. Geriatr Orthop Surg Rehabil. 2022 Mar 29;13:21514593221083820. https://doi.org/10.1177/21514593221083820 [ Links ]
19. Kuzyk PR, Zdero R, Shah S, et al. Femoral head lag screw position for cephalomedullary nails: a biomechanical analysis. J Orthop Trauma. 2012 Jul;26(7):414-21. [ Links ]
20. Puthezhath K, Jayaprakash C. Is calcar referenced tip-apex distance a better predicting factor for cutting outin biaxial cephalomedullary nails than tip-apex distance? J Orthop Surg (Hong Kong). 2017 Sep-Dec;25(3):2309499017727920. https://doi.org/10.1177/2309499017727920 [ Links ]
21. Lopes-Coutinho L, Dias-Carvalho A, Esteves N, Sousa R. Traditional distance 'tip-apex' vs. new calcar referenced 'tip-apex' - which one is the best peritrochanteric osteosynthesis failure predictor? Injury. 2020 Mar;51(3):674-77. [ Links ]
22. Kane P, Vopat B, Heard W, et al. Is tip apex distance as important as we think? A biomechanical study examining optimal lag screw placement. Clin Orthop Relat Res. 2014 Aug;472(8):2492-98. [ Links ]
23. Kashigar A, Vincent A, Gunton MJ, et al. Predictors of failure for cephalomedullary nailing of proximal femoral fractures. Bone Joint J. 2014 Aug;96-B(8):1029-34. [ Links ]
24. Kaplan K, Miyamoto R, Levine BR, et al. Surgical management of hip fractures: an evidence-based review of the literature. II: intertrochanteric fractures. J Am Acad Orthop Surg. 2008 Nov;16(11):665-73. [ Links ]
25. Hip fracture: management. London: National Institute for Health and Care Excellence (NICE); 2017 May. [ Links ]
26. Roberts KC, Brox WT, Jevsevar DS, Sevarino K. Management of hip fractures in the elderly. J Am Acad Orthop Surg. 2015 Feb;23(2):131-37. [ Links ]
27. Arirachakaran A, Amphansap T, Thanindratarn P, et al. Comparative outcome of PFNA, Gamma nails, PCCP, Medoff plate, LISS and dynamic hip screws for fixation in elderly trochanteric fractures: a systematic review and network meta-analysis of randomized controlled trials. Eur J Orthop Surg Traumatol. 2017 Oct;27(7):937-52. [ Links ]
28. Savio SD, Susila IMA, Dharmayuda CGO. Functional outcome & revision rate of PFNA vs DHS for osteoporotic intertrochanteric femur fracture: a meta analysis. Combined Sixth Scientific Meeting of Indonesian Hip and Knee Society (IHKS), Asia Pacific Knee Society (APKS). Asia Pacific Infection So. Orthop J Sports Med. 2020;8:1. [ Links ]
29. Shu WB, Zhang XB, Lu HY, et al. Comparison of effects of four treatment methods for unstableintertrochanteric fractures: A network meta-analysis. Int J Surg. 2018 Dec;60:173-81. [ Links ]
30. Wang HH, Shu WB, Lan GH, et al. Network meta-analysis of surgical treatment for unstable femoral intertrochanteric fractures. Oncotarget. 2018 Jan 2;9(35):24168-77. [ Links ]
31. Parker M, Raval P, Gjertsen JE. Nail or plate fixation for A3 trochanteric hip fractures: A systematic review of randomised controlled trials. Injury. 2018 Jul;49(7):1319-23. [ Links ]
32. Kim CH, Chang JS, Kim JW. Clinical outcomes of dynamic hip screw fixation of intertrochanteric fractures: comparison with additional anti-rotation screw use. Eur J Orthop Surg Traumatol. 2019 Jul;29(5):1017-23. [ Links ]
33. Hodel S, Beeres FJP, Babst R, Link BC. Complications following proximal femoral locking compression plating in unstable proximal femur fractures: medium-term follow-up. Eur J Orthop Surg Traumatol. 2017 Dec;27(8):1117-24. [ Links ]
34. Dhamangaonkar AC, Joshi D, Goregaonkar AB, Tawari AA. Proximal femoral locking plate versus dynamic hip screw for unstable intertrochanteric femoral fractures. J Orthop Surg (Hong Kong). 2013 Dec;21(3):317-22. [ Links ]
35. Han L, Liu JJ, Hu YG, et al. Controlled study on Gamma nail and proximal femoral locking plate for unstable intertrochanteric femoral fractures with broken lateral wall. Sci Rep. 2018 Jul 24;8(1):11114. [ Links ]
36. Kovalak E, Ermutlu C, Atay T, Bacal Ö. Management of unstable pertrochanteric fractures with proximal femoral locking compression plates and effect of neck-shaft angle on functional outcomes. J Clin Orthop Trauma. 2017 Jul-Sep;8(3):209-214. [ Links ]
37. Hardy DC, Descamps PY, Krallis P, et al. Use of an intramedullary hip-screw compared with a compression hip-screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients. J Bone Joint Surg Am. 1998 May;80(5):618-30. [ Links ]
38. Lorich DG, Geller DS, Nielson JH. Osteoporotic pertrochanteric hip fractures: management and current controversies. Instr Course Lect. 2004;53:441-54. [ Links ]
39. Lewis SR, Macey R, Lewis J, et al. Surgical interventions for treating extracapsular hip fractures in older adults: a network meta-analysis. Cochrane Database Syst Rev. 2022 Feb 10;2(2):CD013405. [ Links ]
40. Lewis SR, Macey R, Gill JR, et al. Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults. Cochrane Database Syst Rev. 2022 Jan 26;1(1):CD000093. [ Links ]
41. Chang SM, Song DL, Ma Z, et al. Mismatch of the short straight cephalomedullary nail (PFNA-II) with the anterior bow of the Femur in an Asian population. J Orthop Trauma. 2014 Jan;28(1):17-22. [ Links ]
42. Mukherjee K, Prashanth TKR, Thirunthaiyan MR, Kumar DR. Mismatch of short straight proximal femur nails with anterior bow of femur in Indian population - A radiological and functional analysis. J Orthop. 2022 Jan 29;29:65-70. [ Links ]
43. Zhang S, Zhang Y, Hu S, et al. Imaging study on design and geometric match of a new type of short femoral intertrochanteric nail with anterior curvature. 2016 Oct 8;30(10):1200-204. [Chinese] [ Links ]
44. Chang SM, Hu SJ, Ma Z, et al. Femoral intertrochanteric nail (fitn): a new short version design with an anterior curvature and a geometric match study using post-operative radiographs. Injury. 2018 Feb;49(2):328-33. [ Links ]
45. Blum LE, Yee MA, Mauffrey C, et al. Comparison of reamed long and short intramedullary nail constructs in unstable intertrochanteric femur fractures: A biomechanical study. OTA Int. 2020 May 5;3(2):e075. [ Links ]
46. Hulet DA, Whale CS, Beebe MJ, et al. Short versus long cephalomedullary nails for fixation of stable versus unstable intertrochanteric femur fractures at a level 1 trauma center. Orthopedics. 2019 Mar 1;42(2):e202-e209. [ Links ]
47. Lacroix H, Arwert H, Snijders CJ, Fontijne WP. Prevention of fracture at the distal locking site of the gamma nail. A biomechanical study. J Bone Joint Surg Br. 1995 Mar;77(2):274-76. [ Links ]
48. Rosenblum SF, Zuckerman JD, Kummer FJ, Tam BS. A biomechanical evaluation of the Gamma nail. J Bone Joint Surg Br. 1992 May;74(3):352-57. [ Links ]
49. Yan WS, Cao WL, Sun M, et al. Distal locked or unlocked nailing for stable intertrochanteric fractures? A meta-analysis. ANZ J Surg. 2020 Jan;90(1-2):27-33. [ Links ]
50. Buruian A, Silva Gomes F, Roseiro T, et al. Distal interlocking for short trochanteric nails: static, dynamic or no locking? Review of the literature and decision algorithm. EFORT Open Rev. 2020 Aug 1;5(7):421-29. [ Links ]
51. Chouhan D, Meena S, Kamboj K, et al. Distal locked versus unlocked intramedullary nailing in intertrochanteric fracture: a systematic review and meta-analysis of randomized and non-randomized trials. Bull Emerg Trauma. 2020 Apr;8(2):56-61. [ Links ]
52. Rosen M, Kasik C, Swords M. Management of lateral thigh pain following cephalomedullary nail: a technical note. Spartan Med Res J. 2020 Jun 8;5(1):12931. [ Links ]
53. Lil NA, Makwana VR, Patel TD, Patel AR. Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws. World J Orthop. 2022 Mar 18;13(3):267-77. [ Links ]
54. Hardy DC, Drossos K. Slotted intramedullary hip screw nails reduce proximal mechanical unloading. Clin Orthop Relat Res. 2003 Jan;(406):176-84. [ Links ]
55. Skála-Rosenbaum J, Dzupa V, Bartoska R, et al. Distal locking in short hip nails: Cause or prevention of peri-implant fractures? Injury. 2016 Apr;47(4):887-92. [ Links ]
56. Ciaffa V, Vicenti G, Mori C, et al. Is distal locking with short intramedullary nails necessary in stable pertrochanteric fractures? A prospective, multicentre, randomised study. Injury. 2016 Oct;47 Suppl 4:S98-S106. [ Links ]
57. Ciaffa V, Vicenti G, Mori CM, et al. Unlocked versus dynamic and static distal locked femoral nails in stable and unstable intertrochanteric fractures. A prospective study. Injury. 2018 Nov;49 Suppl 3:S19-S25. [ Links ]
58. Lanzetti RM, Caraffa A, Lupariello D, et al. Comparison between locked and unlocked intramedullary nails in intertrochanteric fractures. Eur J Orthop Surg Traumatol. 2018 May;28(4):649-58. [ Links ]
59. Nherera L, Trueman P, Horner A, et al. Comparison of a twin interlocking derotation and compression screw cephalomedullary nail (InterTAN) with a single screw derotation cephalomedullary nail (proximal femoral nail antirotation): a systematic review and meta-analysis for intertrochanteric fractures. J Orthop Surg Res. 2018 Mar 2;13(1):46. [ Links ]
60. Ma JX, Kuang MJ, Fan ZR, et al. Comparison of clinical outcomes with InterTan vs Gamma nail or PFNA in the treatment of intertrochanteric fractures: A meta-analysis. Sci Rep. 2017 Nov 21;7(1):15962. [ Links ]
61. Ng M, Shah NS, Golub I, et al. No difference between lag screw and helical blade for cephalomedullary nail cut-out a systematic review and meta-analysis. Eur J Orthop Surg Traumatol. 2021 Oct 19. [ Links ]
62. Fan L, Dang X, Wang K. Comparison between bipolar hemiarthroplasty and total hip arthroplasty for unstable intertrochanteric fractures in elderly osteoporotic patients. PLoS One. 2012;7(6):e39531. [ Links ]
63. Haentjens P, Casteleyn PP, De Boeck H, et al. Treatment of unstable intertrochanteric and subtrochanteric fractures in elderly patients. Primary bipolar arthroplasty compared with internal fixation. J Bone Joint Surg Am. 1989 Sep;71(8):1214-25. [ Links ]
64. Chan KC, Gill GS. Cemented hemiarthroplasties for elderly patients with intertrochanteric fractures. Clin Orthop Relat Res. 2000 Feb;(371):206-15. [ Links ]
65. Nie B, Wu D, Yang Z, Liu Q. Comparison of intramedullary fixation and arthroplasty for the treatment of intertrochanteric hip fractures in the elderly: A meta-analysis. Medicine (Baltimore). 2017 Jul;96(27):e7446. [ Links ]
66. Ju JB, Zhang PX, Jiang BG. Hip replacement as alternative to intramedullary nail in elderly patients with unstable intertrochanteric fracture: a systematic review and meta-analysis. Orthop Surg. 2019 Oct;11(5):745-54. [ Links ]
67. Chen WH, Guo WX, Gao SH, et al. Arthroplasty vs proximal femoral nails for unstable intertrochanteric femoral fractures in elderly patients: A systematic review and meta-analysis. World J Clin Cases. 2021 Nov 16;9(32):9878-88. [ Links ]
68. Kumar P, Rajnish RK, Sharma S, Dhillon MS. Proximal femoral nailing is superior to hemiarthroplasty in AO/OTA A2 and A3 intertrochanteric femur fractures in the elderly: a systematic literature review and meta-analysis. Int Orthop. 2020 Apr;44(4):623-33. [ Links ]
69. Waddell JP, Morton J, Schemitsch EH. The role of total hip replacement in intertrochanteric fractures of the femur. Clin Orthop Relat Res. 2004 Dec;(429):49-53. [ Links ]
70. Zha GC, Chen ZL, Qi XB, Sun JY. Treatment of pertrochanteric fractures with a proximal femur locking compression plate. Injury. 2011 Nov;42(11):1294-99. [ Links ]
71. Cui Z, Feng H, Meng X, et al. Age-specific 1-year mortality rates after hip fracture based on the populations in mainland China between the years 2000 and 2018: a systematic analysis. Arch Osteoporos. 2019 May 25;14(1):55. [ Links ]
72. Guo Y, Yang HP, Dou QJ, et al. Efficacy of femoral nail anti-rotation of helical blade in unstable intertrochanteric fracture. Eur Rev Med Pharmacol Sci. 2017 Jul;21(3 Suppl):6-11. [ Links ]
73. Cheng YX, Sheng X. Optimal surgical methods to treat intertrochanteric fracture: a Bayesian network meta-analysis based on 36 randomized controlled trials. J Orthop Surg Res. 2020 Sep 10;15(1):402. [ Links ]
74. Marks L, Pass B, Knobe M, et al. Quality of life, walking ability and change of living situation after trochanteric femur fracture in geriatric patients-Comparison between sliding hip screw and cephalomedullary nails from the registry for geriatric trauma. Injury. 2021 Jul;52(7):1793-800. [ Links ]
75. Mid-year population estimates. Pretoria: Statistics South Africa (Stats SA); 2021. Available from: http://www.statssa.gov.za/publications/P0302/P03022021.pdf. Accessed 14 Mar 2022. [ Links ]
76. Fuleihan G. The Middle East and Africa Audit (2011) International Osteoporosis Foundation. Available from: https://www.aub.edu.lb/fm/cmop/downloads/ME_audit-e.pdf. Accessed 14 Mar 2022. [ Links ]
77. Van Tonder E, Gardner L, Cressey S, et al. Adult malnutrition: prevalence and use of nutrition-related quality indicators in South African public-sector hospitals. South Afr J Clin Nutr. 2019;32(1):1-7. [ Links ]
78. Li XP, Zhang P, Zhu SW, et al. All-cause mortality risk in aged femoral intertrochanteric fracture patients. J Orthop Surg Res. 2021 Dec 20;16(1):727. [ Links ]
Received: March 2022
Accepted: June 2022
Published: March 2023
* Corresponding author: falethu.sukati@up.ac.za
Editor: Prof. Nando Ferreira, Stellenbosch University, Cape Town, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}