










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.21 no.4 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n4a1
PAEDIATRIC ORTHOPAEDICS
Access gate-related lower limb fractures in children and adolescents: a review of injury patterns and evaluation of associated injuries
Mashupse P PhalaI; Pududu A RachueneII, *; Bongani SocutshanaI; Khetani S BilaIII
IDepartment of Orthopaedics, Sefako Makgatho Health Sciences University, Dr George Mukhari Academic Hospital, Pretoria, South Africa
IIDepartment of Orthopaedics, Shoulder and Elbow Unit, Sefako Makgatho Health Sciences University, Dr George Mukhari Academic Hospital, Pretoria, South Africa
IIIDepartment of Orthopaedics, Paediatric Orthopaedic Unit, Sefako Makgatho Health Sciences University, Dr George Mukhari Academic Hospital, Pretoria, South Africa
ABSTRACT
BACKGROUND: Lower limb fractures occurring in and around the home environment and caused by collapsing access gates present frequently to our emergency unit. There is currently limited literature evaluating injuries resulting from access gate accidents. The aim of this study was to evaluate the patterns of lower limb fractures, management options offered and concomitant injuries in children as well as adolescents presenting with access gate-related lower limb traumas.
METHODS: A retrospective cross-sectional review of 43 children with 46 lower limb fractures was conducted between 1 January 2017 and 31 December 2020. Hospital records and radiology archives of all children and adolescents under 12 years of age (24 males and 8 females) with lower limb fractures sustained following an access gate injury were reviewed and included for analysis. Data was analysed descriptively using SAS (SAS Institute Inc, Carey, NC, USA), Release 9.4.
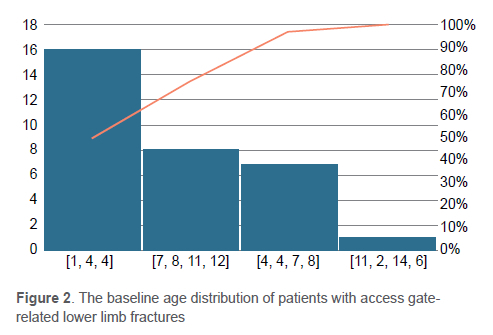
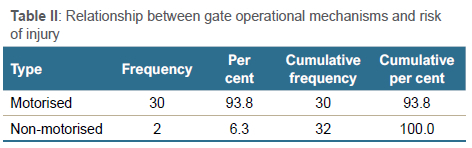
RESULTS: The prevalence of access gate-related injuries for all lower limb fractures in children and adolescents treated during the four-year period was 11%. The findings revealed that femur fractures are more common, accounting for 50.0% of the cases. The majority of cases were of patients younger than 6 years (71.9%), and predominantly affecting males (3:1). The fractures occurred in a home environment and were commonly related to non-motorised gates, in 93.8% of cases. The oblique fracture patterns comprised 40.6% of the fractures, and 68.8% of the fractures were located in the diaphysis. Open fractures constituted 50.0% of the tibia fractures. Mild head injuries associated with lower limb fractures were observed in 12.5% of the cases.
CONCLUSION: The results demonstrated the prevalence of lower limb fractures above all injuries related to access gates. The majority of the injuries observed in this study occurred in manually operated gates, and commonly affected younger patients. In light of these findings, further studies are required into the reasons for these injuries and preventative measures
Level of evidence: Level 4.
Keywords: access gate, lower limb fractures, children, adolescents
Introduction
Fenced yards and access gates are a common security feature in most homes in middle- to low-income countries, due to high levels of crime and house break-ins (Figure 1). It is the norm to find this kind of security measure in suburban and rural homes in these countries. The gates in these societies are often automatically operated (motorised) or manually operated (non-motorised). The accidental derailment and collapse of these gates may result in injuries during the operation (closing or opening) or climbing of the gate.

Numerous injury mechanisms are described in childhood fractures which can occur at home or the surrounding environment.
The majority of these injuries occur at home. These include falls, non-accidental injuries (NAI) and crush injuries resulting from falling objects.1,2 Injuries related to access gates are not extensively reported in literature. Studies have shown that children and adolescents from deprived socio-economic areas have a three to eight times higher risk of sustaining femur fractures compared to those in well-off areas.3,4 Falling objects are reported to be responsible for about 10% of paediatric femur fractures.2,4 Mughal et al. found that the median age of patients struck by falling objects was 4.8 years.4 The fracture patterns observed in the study are often related to the causative injury mechanism and have an impact on the treatment modality and outcomes of the fracture.
This study was conducted to assess the prevalence of lower limb fractures, demographic distribution, fracture and injury patterns, and concomitant injuries in these population groups after observing a high number of cases presenting with access gate-related lower limb injuries. We believe that this research is critical in informing the public and clinicians about the dangers of access gates.
Methods
This study is a retrospective review of the hospital records of 403 paediatric and adolescent patients with lower limb fractures treated at our unit during the four-year period 1 January 2017 to 31 December 2020, with the objective to identify those with access gate-related lower limb fractures. Forty-three patients with lower limb fractures following access gate accidents from this cohort were identified. We included all children and adolescents (aged 12 years and below) with lower limb fractures sustained following an access gate accident or any other incident. Patients with incomplete records were excluded (n = 11) from the final analysis. Incomplete records included lost radiological images and clinical notes.
The data collected from the clinical records and radiology archives included demographic characteristics (age, sex and geographical location of residence), mechanisms of injury, diagnosis, site of fracture, anatomical location (diaphyseal, epiphyseal or metaphyseal), descriptive fracture patterns (transverse, oblique, spiral or comminuted), concomitant injuries, methods of treatment and complications (Figures 2 and 3). The accounts on mechanisms of injury were recorded in the clinical notes of these patients. The picture archiving and communication system (PACS, Carestream Health Vue Motion Inc 2022) was used to retrieve and evaluate the X-ray images of all the participants. This evaluation was conducted by a single observer on one occasion and the patients had a minimum of three months follow-up. The patients were also assessed for clinical and radiological complications related to the treatment methods used to treat their injuries. A complication was defined as a worsening of the patient's outcome on clinical and radiological evaluation or intervention-related adverse events following the intervention. The anatomical axis of the affected bone was measured on two-view X-rays using computer software, and shortening was determined by the degree of fracture ends overlap. This was further correlated with findings recorded in the clinical notes. The potential for bone remodelling and catch-up growth were not evaluated because they were outside the scope of this study. The accounts of the depth of infection were taken from the clinical notes due to the retrospective nature of the study, and the treating surgeons' criteria were not specified.

The data collected were compiled in a Microsoft Excel spreadsheet for analysis. Demographic and clinical characteristics of the patients were summarised descriptively. Continuous variables (e.g., age) were summarised by mean (± standard deviation [SD]), and/or median (interquartile range [IQR]) with the minimum and maximum values. Categorical variables (e.g., sex, mechanism of injury, fracture patterns, fracture site, head injuries, etc.) were summarised by frequency counts and percentage calculations. Statistical tests were two-sided and p-values < 0.05 were considered significant. All the statistical procedures were performed on SAS (SAS Institute Inc, Carey, NC, USA), release 9.4 or higher, running on Microsoft Windows for a personal computer.
The study sample consisted of patients from predominantly low-income communities. The collation and transcription of medical information and X-ray results from medical records to the data collection form was carried out by the researcher. Collected data was stored in a secured database and anonymised data prepared for final analysis.
Results
Demographic distribution and mechanisms of injury
The lower limb fractures related to access gate accidents accounted for 11.0% (n = 43) of all lower limb fractures in children and adolescents admitted during the study period. The male proportion of patients with lower limb fractures was higher than the female proportion at a ratio of 3:1. The median age of the cohort was 4.5 years (IQR 3-8 years). The youngest and the oldest patients were 1 year and 12 years respectively. Children were categorised into two age groups of 0-6 and 7-12 years for description purposes. Seventy-two per cent of the patients in this study were aged between 0 and 6 years of age. The gate falling on the child was a predominant mechanism of injury and occurred in 93.8% of the study sample. Only 6.3% of the entire whole cohort reported being knocked by the gate (Table I). Manually operated gates accounted for the majority of the injuries (Table II).

Fracture patterns and distribution
Femur fractures were the most commonly observed injuries (50%), followed by tibia/fibula (12.5%) and ankle fractures respectively (9.4%) (Table III). Open fractures mostly involved the tibia/fibula whereas all the ankle fractures involved the physis. Table IV indicates that the fractures of the diaphyseal segment was significantly more common (68.8%) than other bone segments. The involvement of both the metaphysis and diaphysis was found in a setting of a single patient with two fractures. All physeal fractures involved the ankle and were type II Salter-Harris fractures. The majority of the fractures had an oblique fracture pattern, 40.6% (n = 13), followed by a spiral fracture pattern at 25.0% (n = 8). The prevalence of transverse and comminuted fracture patterns was the same at 15.6% (n = 5). Mild head injury was the only associated injury found in this study. Femur fractures were present in 75% (n = 3), while tibia/fibula fractures were present in 25% (n = 1) of the study participants with head injuries.


Interventions and complications
Surgical treatment was offered to 93.8% (n = 30) of the patients. The titanium elastic nail system (TENS) was the most common treatment method used in 53% (n = 17) of the patients with length unstable diaphyseal femur fractures, followed by close reduction (C/R) and plaster of Paris (POP) in 22% (n = 7). Cerclage wire was used as an adjunct in one case whereas the K-wires were used in the treatment of metatarsal fractures of the foot. The non-surgical treatment in the form of skin traction was offered to only 6.3% (n = 2). The study shows a complication rate of 12.5%. The types of complications encountered were shortening, implant migration plus shortening and infection. These were seen in length unstable and open fractures respectively.
Discussion
Lower limb fractures are less common than those affecting the upper limb in children and adolescents. This is related to the prevalence of mechanisms of injury in these population groups, with falls being the most common and sports-related injuries noted in adolescence.3,4 Among those with lower limb fractures, femur fractures are reported to be the commonest. Access gate-related injuries are commonly observed in our setting, accounting for 11% of all lower limb injuries in children and adolescents treated at our unit. These are commonly associated with non-motorised, manually operated gates (94%). While this remains under-reported in the literature, similar observations have been reported by some authors with similar injury mechanisms. Cheng et al. reported an annual rate of 1 794 baby gate-related injuries in children aged < 2 years between the years 1990 and 2010.5 Sex distribution in our study was similar to those reported in the literature with a male-to-female ratio of 3:1.4,6,7 Comparable to other studies, boys were more likely to sustain femoral fractures.8,9 The behavioural difference related to the sex of the child is thought to explain the male predominance, with high-risk playing activities being more common in boys than in girls.8,10,11
The majority (72%) of the children in our cohort were younger, aged between 0 and 6 years of age. This is consistent with findings by Mughal et al., who found that the median age of patients struck by falling objects was 4.8 years.4 However, other researchers reported bimodal age distribution.2 In addition to the increased mobility in younger children, their femurs have decreased cortical thickness due to a higher ratio of woven bone compared to lamellar bone, which explains why a low-energy mechanism can easily result in femur fracture.12 Additionally, toddlers have not yet fully developed their physical capabilities, and outpace judgment skills and protective reflexes.11
The majority of the fractures in this study occurred in a home or neighbourhood environment, similar to published literature.2,13 We posit this is due to inadequate supervision of these children at home or lack of safe playing areas, such as public parks, in these poor communities. Ng'ang'a et al. noted that most children from low-income households are looked after by older siblings or unqualified nannies as parents go to work.2
Fracture distribution in this study involved the femur more commonly (n = 16), followed by tibia/fibula fractures at 18.8% (n = 6). The diaphyseal segment of the bone is more commonly affected, representing 68.8% (n = 22) of cases, and aligning with the literature.2,4 Lower limb fractures in these age groups often follow a torsional force resulting in an oblique or a spiral fracture pattern.3,14 This has a bearing on the choice of fracture treatment, despite the most common injury mechanism being a direct force from the falling gate. Similar fracture patterns were, however, commonly observed in this study. Hedström et al. and Ng'ang'a et al. respectively found that 14.8% and 12% of fractures in children involved the growth plate.2,15 This is comparable to the 12.5% (n = 4) that was observed in our study. These were all type II Salter-Harris ankle fractures. Open fractures were observed in 50% (n = 4) of the tibia fractures. This is comparable to the observations of the other authors.15,16
In their review of the 37 673 cases of access gate-related injuries, Cheng et al. found head injuries to be the commonest presenting injury following gate-related events.5 We observed head injury in 12.5% (n = 4) of the study population. These observations did not vary significantly from the usual patterns of associated injuries reported in paediatric and adolescent lower fractures. However, a high association of abdominal injury followed by closed head injury is often reported.17-19 Our findings are consistent with those of a local study by Setati et al., reported in their unpublished Master of Medicine in Orthopaedics dissertation. Setati and colleagues found that access gates were the cause of accidental head injury in 9.3% of children.20
Surgical treatment was offered in 93.8% (n = 30) of patients, mostly with length unstable fractures. A quarter of the patients who underwent surgery had minor complications not requiring further surgery.
This study has several limitations. Because of the retrospective design, we had to rely on hospital records to collect data. Therefore, this is subject to recording error. We also acknowledge that a significant number of patients (25.6%) qualifying for inclusion criteria were excluded from this study due to incomplete records. This may have an impact on the results. Furthermore, because these incidents included children and toddlers, the mechanisms of injury narratives were gathered through the narration of parents or caregivers who would not have been present when the injury occurred, making it prone to reporting and interpretation problems.
This study was conducted in a single centre and it involves a small sample group, thus affecting the validity of our results. Furthermore, we did not investigate whether the injuries were caused by sliding or swinging gates. It is, however, important to note that the results of this study potentially highlight a public health hazard posed by the access gates.
Conclusion
Access gate-related lower limb fractures are less commonly observed compared to other injury mechanisms in children and adolescents. However, they are still commonly seen in our setting. Most of these fractures are isolated diaphyseal length unstable injuries, commonly affecting younger children. Manually operated gates are likely to result in lower limb fractures compared to motorised gates. The use of motorised gates and appropriate child supervision at home may reduce the chance of these injuries.
Acknowledgement
We would like to acknowledge and thank Dr Gezani Freeman Mabasa for his involvement in the early phases of this project.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. Prior to commencement of the study, ethics approval was obtained from the Postgraduate Studies, Research Development, Integrity & Ethics Sefako Makgatho Research Ethics Committee: SMUREC/M/53/2021: PG.
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki
Declaration of 1975, as revised in 2008. Informed written consent was not obtained from the participants due to the retrospective nature of this study.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
MPP: study conceptualisation, manuscript review, revisions and production of final manuscript
PAR: literature review, data collection and compilation of first draft, manuscript review, revisions and production of final manuscript
BS: literature review, data collection and compilation of first draft, manuscript review, revisions and production of final manuscript
KSB: study conceptualisation, manuscript review, revisions and production of final manuscript
ORCID
Phala MPhttps://orcid.org/0000-0002-8013-8290
Rachuene PA https://orcid.org/0000-0003-4045-5301
Socutshana B https://orcid.org/0000-0003-2845-5122
Bila KS https://orcid.org/0000-0001-7130-7307
References
1. Ong MEH, Ooi SBS. A review of 2,517 childhood injuries seen in a Singapore Emergency Department in 1999 - Mechanisms and injury prevention suggestions. Available from: https://www.researchgate.net/publication/10746286. Accessed 10 January 2022. [ Links ]
2. Ng'ang'a E, Mutiso VM, Mwangi JC. Pattern of long bone fractures in a paediatric population at Kenyatta National Hospital. East African Orthop J. 2018;11(2):54-60. [ Links ]
3. Menon MRG, Walker JL, Court-Brown CM. The epidemiology of fractures in adolescents with reference to social deprivation. J Bone Jt Surg - Ser B. 2008;90(11):1482-86. https://doi.org/10.1302/0301-620X.90B11.21163 [ Links ]
4. Mughal MA, Dix-Peek SI, Hoffman EB. The epidemiology of femur shaft fractures in children. SA Orthop J. 2013;12(4):23-27. [ Links ]
5. Cheng YW, Fletcher EN, Roberts KJ, McKenzie LB. Baby gate-related injuries among children in the United States, 1990-2010. Acad Pediatr. 2014;14(3):256-61. https://doi.org/10.1016/J.ACAP.2013.12.006 [ Links ]
6. Loder RT, O'Donnell PW, Feinberg JR. Epidemiology and mechanisms of femur fractures in children. J Pediatr Orthop. 2006;26(5):561-66. https://doi.org/10.1097/01.BPO.0000230335.19029.AB [ Links ]
7. Von Heideken J, Svensson T, Blomqvist P, et al. Incidence and trends in femur shaft fractures in Swedish children between 1987 and 2005. J Pediatr Orthop. 2011;31(5):512-19. https://doi.org/10.1097/BPO.0B013E31821F9027 [ Links ]
8. Joeris A, Lutz N, Wicki B, et al. An epidemiological evaluation of pediatric long bone fractures - a retrospective cohort study of 2716 patients from two Swiss tertiary pediatric hospitals. BMC Pediatr. 2014;14(1):1-11. https://doi.org/10.1186/S12887-014-0314-3/TABLES/6 [ Links ]
9. Capra L, Levin AV, Howard A, Shouldice M. Characteristics of femur fractures in ambulatory young children. Emerg Med J. 2013;30(9):749-53. https://doi.org/10.1136/EMERMED-2012-201547 [ Links ]
10. Cooper C, Dennison EM, Leufkens HG, et al. Epidemiology of childhood fractures in Britain: a study using the general practice research database. Wiley Online Libr. 2004;19(12):1976-81. https://doi.org/10.1359/JBMR.040902 [ Links ]
11. Hinton RY, Lincoln A, Crockett MM, et al. Fractures of the femoral shaft in children. J Bone Jt Surg. 1999;81(4):500-507. [ Links ]
12. Beaty JH, Kasser JR. Rockwood and Wilkin's fractures in children. Philadelphia: Lippincott, Williams & Wilkins; 2010. p. 1076-76. [ Links ]
13. Valerio G, Gallè F, Mancusi C, et al. Pattern of fractures across pediatric age groups: Analysis of individual and lifestyle factors. BMC Public Health. 2010;10(1):1-9. https://doi.org/10.1186/1471-2458-10-656/TABLES/6 [ Links ]
14. Pierce MC, Bertocci GE, Vogeley E, Moreland MS. Evaluating long bone fractures in children: A biomechanical approach with illustrative cases. Child Abus Negl. 2004;28(5):505-24. https://doi.org/10.1016/j.chiabu.2003.01.001 [ Links ]
15. Hedström EM, Svensson O, Bergström U, Michno P. Epidemiology of fractures in children and adolescents. Acta Orthop. 2010;81(1):148-53. https://doi.org/10.3109/17453671003628780 [ Links ]
16. Tandon T, Shaik M, Modi N. Paediatric trauma epidemiology in an urban scenario in India. J Orthop Surg (Hong Kong). 2007;15(1):41-45. https://doi.org/10.1177/230949900701500110 [ Links ]
17. Dodd A, Paolucci EO, Parsons D. Paediatric femoral shaft fractures: What are the concomitantinjuries? Injury. 2013;44(11):1502-06. https://doi.org/10.1016/J.INJURY.2013.02.012 [ Links ]
18. Liu H, Wang H, Shao B, et al. Epidemiological evaluation of traumatic lower limb fractures in children Variation with age, gender, time, and etiology. Medicine. 2019;98(38):e17123. https://doi.org/10.1097/MD.0000000000017123 [ Links ]
19. Rewers A, Hedegaard H, Lezotte D, et al. Childhood femur fractures, associated injuries, and sociodemographic risk factors: a population-based study. Pediatrics. 2005;115(5):e543-52.https://doi.org/10.1542/peds.2004-1064 [ Links ]
20. Setati S, Lekgwara PL, Kelly A. An audit of the epidemiology of head injuryin children (post-graduate thesis) at Dr George Mukhari Academic Hospital, Sefako Makgatho Health Sciences University, Pretoria, South Africa. 2017. [ Links ]
Received: April 2022
Accepted: August 2022
Published: November 2022
Editor: Dr Jacques du Toit, Stellenbosch University, Cape Town, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.
* Corresponding author: archie.pududu@gmail.com

