










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.21 n.3 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n3a5
ORTHOPAEDIC ONCOLOGY AND INFECTIONS
Epidemiology of primary bone tumours in Nigeria: a systematic review
Temitayo T KoyejoI, *; Opeyemi I OlusunmadeII; Olukemi T OlufemiIII
IDepartment of Orthopaedics and Trauma, National Orthopaedic Hospital, Igbobi, Lagos, Nigeria
IIOrthopaedic Oncology Unit, Department of Orthopaedics and Trauma, National Orthopaedic Hospital, Igbobi, Lagos, Nigeria
IIIArthroplasty Unit, Department of Orthopaedics and Trauma, National Orthopaedic Hospital, Igbobi, Lagos, Nigeria
ABSTRACT
BACKGROUND: Primary bone tumours, although rare, are an important rising cause of morbidity and mortality in Africa. Late presentation, delayed diagnosis and failure to obtain consent for surgical procedures are important causes of loss of limb and life especially in the West African subregion. Existing data on primary bone tumours in Nigeria have been based on studies performed at various regional levels. The aim of this study is to determine the epidemiological pattern of primary bone tumours in Nigeria in general, including demographics, predominant tumour types and predominant skeletal location by reviewing existing data
METHODS: A search of the following databases: University of Edinburgh Library, PubMed, CINAHL and SCOPUS from 2000 till January 2021 following PRISMA guidelines was conducted to identify studies conducted in Nigeria with relevant epidemiological data on primary bone tumours in Nigeria
RESULTS: The search yielded a total of 952 hits from which seven hospital-based retrospective studies met the inclusion criteria for review. The estimated incidence rate of primary bone tumours ranged from 0.08 to 0.31 per 100 000 population. All studies showed a male preponderance. The peak age group of individuals presenting with both benign and malignant primary bone tumours was 11-20 years. Overall, benign tumours were more common. Osteochondromas were the most common benign tumours, while the commonest malignant tumours identified were osteosarcomas. The most common location for both benign and malignant tumours were the tibia and fibula
CONCLUSION: Nigeria shares some similar epidemiological characteristics of primary bone tumour with other countries; however, some peculiar differences have been identified in this study. Population-based studies are required to obtain more accurate epidemiological data about this disease
Level of evidence: Level 2
Keywords: epidemiology, primary bone tumours, Nigeria
Introduction
The human bone consists of various cell types which are capable of proliferating and giving rise to an array of tumours.1 Bone tumours mainly arise from somatic mutations; however, some risk factors have been implicated which include irradiation, chemotherapy, foreign bodies and pre-existing bone lesions.2
Globally, bone sarcomas account for 0.2% of all malignancies with a five-year overall survival rate of 67.9%.3 The incidence of benign bone tumours is higher than primary malignant bone lesions which are usually asymptomatic and less likely to be clinically detected.3 In the United Kingdom, around 560 new cases of bone sarcomas are diagnosed yearly.4 In Italy, an average of 1.3 new malignant bone tumours are diagnosed per 100 000 males/ year and 1.1 per 100 000 females/year.3 The overall incidence rate for bone and joint malignancy in the United States is 0.9 per 100 000 persons per year.3 Trinidad and Tobago has an incidence of 1.125 per 100 000 population annually, while Cameroon has an average incidence of 27 tumours a year, or two per one million inhabitants.5,6 Nigeria has an estimated population of over 210 million people, making it the most populous country in Africa and the sixth most populous in the world.7 Patients with bone tumours in Nigeria usually present late as a result of poverty, ignorance and cultural beliefs.8 In a study by Dauda et al. at the Jos University Teaching Hospital, Nigeria, 13 cases of primary bone tumours were seen per year.2 Obalum et al. saw an average of ten new cases per year at the Lagos University Teaching Hospital, Nigeria.9
Primary bone tumours are classified according to their biological behaviour and form of differentiation. Globally, non-ossifying fibroma is the most common benign tumour of the bone usually found in the metaphyses of long bones, while osteosarcoma is the most common primary malignant tumour of bone with predilection for the metaphysis of long bones.10,11
Osteochondroma was identified as the most common benign bone tumour, while osteosarcoma was shown to be the most common primary malignant bone tumour in the study by Bahebeck et al. in Cameroon, and this was also observed in the study by Obalum et al. in Lagos, Nigeria.6,9 In the United Kingdom, osteosarcomas affects individuals mainly within the age group 10-25 years, with males constituting a larger proportion.11 The major skeletal locations of the tumours are the distal femur and proximal tibia.11 A study conducted in Ibadan, Nigeria revealed osteosarcoma as the most common malignant primary bone tumour affecting predominantly individuals younger than 20 years and being more common in males.12 The major skeletal location of the tumours were the femur and mandible.12 The epidemiological patterns of bone tumours in Nigeria in general has not been ascertained, as only retrospective hospital-based studies in different regions have been performed.
The aim of this study was to determine the epidemiology of primary bone tumours in Nigeria and compare the epidemiological patterns of primary bone tumours in Nigeria to those in other parts of the world.
Materials and methods
Literature search and eligibility criteria
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA), identifying Nigerian studies conducted on primary bone tumours. The data for this study were obtained following an extensive literature search of the University of Edinburgh Library, PubMed, SCOPUS and CINAHL electronic databases and looking through the reference lists of articles identified for relevant articles not indexed in the databases. No language limits were applied to the search strategy. The following search terms were used to search all databases: epidemiology, incidence, prevalence, pattern, 'primary bone tumours', Nigeria. The search was limited to studies published from January 2000. The limit 'nonhuman' was included in the search strategy to exclude all articles conducted in nonhumans. Studies were included if they: 1) were conducted in Nigeria between January 2000 to January 2021; 2) were studies on histologically confirmed primary bone tumours in all age groups and both sexes; 3) published data on demographic variables, tumour type and tumour location. Studies were excluded if they: 1) were not conducted in Nigeria; 2) were published prior to January 2000; 3) did not include histological confirmation of primary bone tumours; 4) were lacking data on demographic variables, tumour type and tumour location; 5) were not specific for primary bone tumours alone.
Data extraction
Two reviewers independently screened the publications to determine those to be included in the study based on the eligibility criteria. The process of study selection and extraction is presented in a PRISMA flow chart (Figure 1).13 Data was extracted by two reviewers independently including study design and year of publication, location of study, number of participants, demographic description, tumour type and tumour location.

Data analysis
The main purpose of the systematic review was to critically appraise the available data to give a broad understanding of the epidemiology of primary bone tumours in Nigeria. A quantitative synthesis of the results of the included studies (meta-analysis) was not conducted due to the retrospective nature of the studies which lacked sufficient data on key variables, but a narrative synthesis was performed. Data extracted from the selected studies which met the eligibility criteria were analysed. Individual assessment of key variables was performed. Graphs and charts were drawn for illustration of key findings. Inferences and conclusions were made based on findings from the selected studies.
Results
Description of studies
Seven hospital-based retrospective studies involving 773 cases of primary bone tumours were included in this systematic review.1,2,9,14-17 The studies were published between 2007 and 2018 involving four of the six geopolitical zones in Nigeria. The characteristics of the studies are shown in Table I.

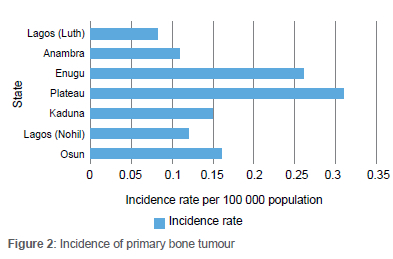
Incidence of primary bone tumours
The number of new cases of primary bone tumour per year varied widely across the institutions. Lagos University Teaching Hospital (LUTH), with ten cases per year, had the lowest incidence rate of 0.08 per 100 000 population, while National Orthopaedic Hospital, Igbobi (NOHIL), Lagos, had the highest incidence with 15.4 cases per year, representing an incidence rate of 0.12 per 100 000 population.9,15 Nnamdi Azikiwe University Teaching Hospital (NAUTH), Anambra, diagnosed 6.2 cases per year representing an incidence rate of 0.11 per 100 000 population (Figure 2).17
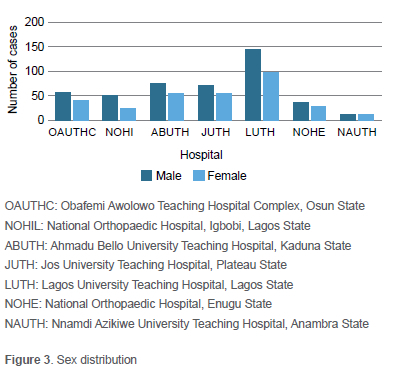
Sex distribution
All studies showed a male preponderance. The lowest male:female ratio was obtained from the study at NAUTH, Anambra, with a ratio of 1.1:1, while the highest ratio was from the study in NOHIL, Lagos, with a ratio of 2:1.15,17 The male:female ratio of other studies included in this systematic review are shown in Figure 3.
Age distribution
In most of the studies, the peak age group of individuals presenting with both benign and malignant primary bone tumours was 11-20 years. However, the study by Ugezu et al. in Anambra revealed the peak age group of patients with primary bone tumours to be 21-30 years with a mean age of 38.8 ± 1.2 years.17 At OAUTHC, Osun State, the peak age group for patients with
benign tumours and tumour-like lesions was 21-30 years, while for malignant tumours was 11-20 years.14
Tumour type
Overall, benign tumours were the most common, accounting for 79% of cases in NOHI, Lagos, and 64.8% of cases in JUTH, Plateau.2,15 In studies performed at LUTH, Lagos, and NOH, Enugu, benign tumours accounted for 53.7% and 41.2% of cases respectively.9,16 However, in the studies performed at Osun, Kaduna and Anambra, malignant tumours were found to be more common than benign tumours accounting for 50%, 39.4% and 58.1% of cases respectively.1,14,17
Among the benign tumours, osteochondroma was found to be the most common, accounting for 32.1%, 55.7% and 40.8% of cases in studies performed at Osun, Lagos (NOHIL) and Kaduna respectively.1,14,15 In Plateau, Lagos (LUTH), Enugu and Anambra, osteochondroma accounted for 27.7%, 27.7%, 75% and 30.8% of benign bone tumours respectively.2,9,16,17 Giant cell tumour was the next most common benign tumour, accounting for 17.9%, 29.5%,16.3% and 12% of cases in studies done in Osun, Lagos (NOHIL), Kaduna and Plateau respectively.1,2,14,15 In studies performed at Lagos (LUTH), Enugu and Anambra, giant cell tumour represented 21.5%, 14.3% and 23.1% of cases respectively.9,16,17
Osteosarcoma was identified as the most common malignant tumour responsible for 42%, 43.8%, 34% and 55.6% of cases in studies performed at Osun, Lagos (NOHIL), Kaduna and Plateau states.1,2,14,15 While in Lagos (LUTH), Enugu and Anambra, osteosarcoma represented 58.9%, 81%% and 50% of cases respectively.9,16,17 Chondrosarcoma was next most common malignant bone tumour responsible for 12%, 6.3%, 6% and 20% of cases in studies performed at Osun, Lagos (NOHIL), Kaduna and Plateau respectively.1,2,14,15 While in Lagos (LUTH), Enugu and Anambra, chondrosarcoma represented 21.4%, 14.3% and 16.7% of cases respectively.9,16,17
For tumour-like lesions, fibrous dysplasia was the most common accounting for 36.3%, 92.8% and 57.8% of cases in studies performed at Osun, Kaduna and Enugu states.1,14,17
Tumour location
The most common malignant tumour location from the studies available were the tibia and fibula, accounting for 47.6%, 26.7% and 2.2% of cases in studies performed in Enugu, Plateau and Kaduna respectively.1,2,16 Craniofacial bones accounted for 58.7%, 6.7% and 4.8% of cases in studies done in Kaduna, Plateau and Enugu respectively.1,2,16
Osteosarcoma, the most common malignant tumour, was found to occur more commonly in the tibia and fibula accounting for 52.9%, 36%, 28.6% and 5.9% of cases in Enugu, Plateau, Osun and Kaduna studies respectively.1,2,14,16 The femur accounted for 47.6%, 36%, 17.6% and 11.8% of cases in Osun, Plateau and Enugu respectively.2,14,16
Benign tumours were found mainly in the tibia and fibula responsible for 60.7%, 18% and 2% of cases in studies performed in Enugu, Plateau and Kaduna.1,2,16 Craniofacial bones accounted for 32.7%, 30.1% and 3.6% of cases in studies done in Kaduna, Plateau and Enugu respectively.1,2,16 Tumour-like lesions were found mostly in the craniofacial bones, accounting for 71.4% and 66.7% of cases in studies performed in Kaduna and Enugu respectively.1,16 Among the benign bone tumours, osteochondroma was found mostly in the tibia accounting for 33.3%, 21.7%, 52.4% of cases in Osun, Plateau and Enugu.2,14,16 The humerus was the next most common site, accounting for 26%, 14.3% and 10% of cases in Plateau, Enugu and Kaduna studies respectively.1,2,16 Fibrous dysplasia, the most common tumour-like lesion, was found mainly in the craniofacial bones in 73% and 63.6% of cases in Kaduna and Enugu studies respectively.1,16
Discussion
The estimated annual incidence rate from this study ranged from 0.11 to 0.31 per 100 000 population. The variation in incidence may be due to the population difference across the states and patterns of health-seeking behaviour among the populace in that state.17 In Cameroon, Bahebeck et al. revealed an annual incidence of 27 tumours a year, while the study by Negash et al. in Ethiopia revealed an annual incidence of 41 tumours a year.6,18 In Italy, the annual incidence rate for bone tumours is 1.3 per 100 000 per year for males, while females have an incidence rate of 1.1 per 100 000 per year.3 Worldwide, the annual incidence rate of primary bone tumours is 0.9 per 100 000 persons per year.3 The figures obtained for the incidence rate for this systematic review are hospital based and may not reflect the true incidence in the population. Patients with bone tumours in this environment may not seek medical attention due to ignorance about the disease, poverty, religious beliefs, patronage of traditional bone setters and fear of ablative surgery.19
The seven selected studies for the systematic review showed a male preponderance. A similar study by Baena-Ocampo et al. in Mexico also showed a male preponderance, with males accounting for 54% and females 46% of cases with a male:female ratio of 1.16:1.20 Deka and Talukdar in India also revealed a male preponderance with a male to female ratio of 1.36:1, while Ramdass et al. in Trinidad and Tobago showed a male:female ratio of 2:1.5,21 Globally, the incidence of bone tumours is marginally higher in males than females, though no reason has been adduced.10
From this study, the adolescent age group was found to be most at risk of developing both benign and malignant primary bone tumours with a peak age incidence of 11-20 years. The peak age incidence for both benign and malignant bone tumours was 11-20 years in a study by Deka and Talukdar in India, which is similar to what was deduced by this study.21 The study by Solooki et al. in Shiraz, Iran, revealed a peak frequency of malignant tumours in patients aged between 5 and 25 years while benign tumours were more commonly seen in those younger than 25 years.22 Worldwide, primary malignant bone tumours have a bimodal distribution with the first peak occurring in the second decade of life and the second peak in patients over 60 years.23 However, the life expectancy of 60 years in Nigeria may be responsible for the lack of bimodal distribution of bone tumours seen.7 The pubertal growth spurt that occurs in adolescence has been linked to the increased incidence of osteosarcoma seen in that age group.24
Benign tumours were the most common among patients diagnosed with bone tumours in this study accounting for 41.2-79% of cases in four of the studies.2,9,15,16 A study by Niu et al. in China also revealed a higher incidence of benign tumours, accounting for 58.7% of all cases in a hospital-based retrospective study.25 Benign bone tumours were also found to be more common in a study by Bahebeck et al. in Cameroon accounting for 48.1% of cases. Among the benign tumours, osteochondroma was found to be the commonest, followed by benign giant cell tumour.6 In a similar study in Mexico by Baena-Ocampo et al., osteochondroma was the most common benign bone tumour representing 43.7% of cases, followed by benign giant cell tumour accounting for 14.6% of cases.20
A study in Minnesota, United States of America, also revealed osteochondroma as the most common benign bone tumour followed by benign giant cell tumour.25 However, Niu et al. showed benign giant cell tumour as the most common benign tumour followed by osteochondroma.25 Three centres, namely OAUTHC, ABUTH and NAUTH, had a higher incidence of malignant bone tumours. This may be due to more patients presenting as a result of pain, swelling, restriction of limb movement and pathological fractures that occur more commonly in malignant bone tumours.26
Osteosarcoma was identified as the most common malignant tumour, while chondrosarcoma was the next most common malignant tumour in this study. However, Bahebeck et al. revealed osteosarcomas as the most common malignant tumour followed by non-Hodgkin's bone lymphoma, while Ramdass et al. in Trinidad and Tobago also had osteosarcoma as the commonest malignant tumour, followed by fibrosarcoma and plasmacytoma.5,6 In the Netherlands, osteosarcoma was identified as the most common malignant bone tumour, followed by chondrosarcoma from data derived from the Netherland Cancer Registry.27
Benign tumours were found mainly in the tibia and fibula, followed by craniofacial bones in this study. Whereas the study by Baena-Ocampo et al. revealed most benign tumours arose in the femur (37%) followed by the tibia (20%), similar to the results obtained by Niu et al. in China, Bahebeck et al. reported the tibia, followed by the femur and spine as the commonest location for benign primary bone tumours.6,20,25 The femur, tibia and bones of the hands were the most common location in the study by Solooki et al.22 However, the skull and femur were identified as the commonest location for benign tumours by Ramdass et al.5
The most common malignant tumour location from the studies available were the tibia and fibula followed by craniofacial bones. These figures are different from those reported by Baena-Ocampo et al. in Mexico which showed the femur (47.8%) as the commonest location for malignant bone tumours followed by the vertebrae (18%).20 Niu et al., in their study in China, revealed the femur followed by the tibia and pelvis as the most common location for malignant primary bone tumours.25 Bahebeck et al. in Cameroon showed the tibia, followed by the femur and spine, as the commonest location for malignant primary bone tumours.6 The femur, humerus and tibia were the most common site for malignant tumours in the study by Solooki et al. in Iran.22
Among the benign bone tumours, osteochondroma was found mostly in the tibia, followed by the humerus. In the United kingdom, the most common site for osteochondroma was the distal femur and proximal tibia, followed by the proximal humerus and proximal fibula.28 Osteosarcoma, the most common malignant tumour, was found to occur mostly in the tibia and fibula, followed by the femur. However, this contrasts with the figures in the United Kingdom where osteosarcoma is commonly found in the metaphyses of long bones, affecting the femur (40%, usually distal), tibia (20%), humerus (10%) and pelvis (8%).26 The study by Pillay et al. in South Africa showed that osteosarcoma involved the distal femur in 44.7% of cases, with the proximal tibia accounting for 34.2% of cases.29
The study was limited due to the hospital-based nature of the studies which may not reflect the true epidemiological nature of disease in the Nigerian population. The studies used were retrospective studies and information obtained by individual studies may have been incomplete due to missing records, poor documentation and inaccurate data entry.
Conclusion
Nigeria shares some similar epidemiological characteristics of primary bone tumour with other countries; however, some peculiar differences have been identified in this study. Population-based studies are required to obtain more accurate epidemiological data about this disease.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. This article does not contain any studies performed by any of the authors on human participants or animals. For this study, formal consent was not required.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
TTK: study conceptualisation, data capture, data analysis, first draft preparation,
manuscript preparation, manuscript revision
OIO: study design, data capture, data analysis, manuscript revision
OTO: study design, data analysis, manuscript revision
ORCID
Koyejo TT https://orcid.org/0000-0002-8976-8467
Olusunmade Ol https://orcid.org/0000-0002-2999-3638
Olufemi OT https://orcid.org/0000-0002-9014-8142
References
1. Mohammed A, Isa HA. Pattern of primary tumours and tumour-like lesions of bone in Zaria Northern Nigeria: A review of 127 cases. West Afr J Med. 2007;26(1):37-41. https://doi.org/10.4314/wajm.v26i1.28301 [ Links ]
2. Dauda AM, Akpa PO, Barka KV, et al. Primary bone tumours at a tertiary health centre in North Central Nigeria: a ten year retrospective review. Asian J Orthop Res. 2018;1(December 2015):1-8. [ Links ]
3. Franchi A. Epidemiology and classification of bone tumors. Clin Cases Miner Bone Metab. 2012;9(2):92-95. [ Links ]
4. Bone sarcoma statistics | Cancer Research UK [Internet]. Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/bone-sarcoma#heading-Zero Accessed 3 September 2019. [ Links ]
5. Ramdass MJ, Mooteeram J, Beharry A, et al. An 8-year analysis of bone tumours in a Caribbeanisland. Ann Med Surg. 2015;4(4):414-46. https://doi.org/10.1016/!.amsu.2015.10.009 [ Links ]
6. Bahebeck J, Atangana R, Eyenga V, et al. Bone tumours in Cameroon: Incidence, demography and histopathology. Int Orthop. 2003;27(5):315-17. https://doi.org/10.1007/s00264-003-0480-7 [ Links ]
7. Africa: Nigeria - The World Factbook - Central Intelligence Agency [Internet]. Available from: https://www.cia.gov/library/publications/the-world-factbook/geos/ni.html Accessed 8 February 2020. [ Links ]
8. Ode M, Misauno M, Nwadiaro H, et al. Pattern and distribution of primary bone tumours in Jos Nigeria. IOSR J Dent Med Sci. 2014;13(12):9-12. [ Links ]
9. Obalum DC, Giwa SO, Banjo AF, Akinsulire AT. Primary bone tumours in a tertiary hospital in Nigeria: 25 year review. Niger J Clin Pract. 2009;12(2):169-72. [ Links ]
10. Ashley B, David W, Michael WR, editors. Apley & Solomon's System of Orthopaedics and Trauma. 10th ed. Apley & Solomon's System of Orthopaedics and Trauma. Boca Raton: CRC Press Taylor & Francis Group; 2018. [ Links ]
11. MacDuff E, Reid R. Bone tumour pathology. Surgery [Internet]. 2009;27(2):55-62. https://doi.org/10.1016/j.mpsur.2008.12.012 [ Links ]
12. Omololu AB, Ogunbiyi JO, Ogunlade SO, et al. Primary malignant bone tumour in a tropical African University teaching hospital. West Afr J Med. 2002;21(4):291-93. https://doi.org/10.4314/wajm.v21i4.28001 [ Links ]
13. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264. https://doi.org/10.7326/0003-4819-151-4-200908180-00135 [ Links ]
14. Aina OJ, Adelusola KA, Orimolade AE, Akinmade A. Histopathological pattern of primary bone tumours and tumour-like lesions in Ile-Ife, Nigeria. Pan Afr Med J. 2018;29:1-9. https://doi.org/10.11604/pamj.2018.29.193.13111 [ Links ]
15. Abdulkareem FB, Eyesan SU, Akinde OR, et al. Pathological study of bone tumours at the National Orthopaedic Hospital, Lagos, Nigeria. West Afr J Med. 2007;26(4):306-11. https://doi.org/10.4314/wajm.v26i4.28332 [ Links ]
16. Lasebikan OA, Nwadinigwe CU, Onyegbule EC. Pattern of bone tumours seen in a regional orthopaedic hospital in Nigeria. Niger J Med. 2014;23(1):46-50. [ Links ]
17. Ugezu AI, Ofiaeli RO, Ihegihu C, Imo C. Pattern of presentation of primary bone tumors in Nnewi , South-East Nigeria. Orient J Med. 2018;30:81-85. [ Links ]
18. Negash BE, Admasie D, Wamisho BL, Tinsay MW. Pattern of bone tumours seen at Addis Ababa University, Ethiopia. East Cent African J Surg. 2009;14(2):25-32. Available from: http://www.bioline.org.br/request7js09030 Accessed 12 September 2019. [ Links ]
19. Salawu O, Babalola O, Ibraheem G, et al. Musculoskeletal tumors of the extremities: challenges and outcome of management in a Nigeria Tertiary Hospital. African J Med Heal Sci. 2018;17:20-25. [ Links ]
20. Baena-Ocampo L del C, Ramirez-Perez E, Linares-Gonzalez LM, Delgado-Chavez R. Epidemiology of bone tumors in Mexico City: retrospective clinicopathologic study of 566 patients at a referral institution. Ann Diagn Pathol. 2009;13(1):16-21. https://doi.org/10.1016/j.anndiagpath.2008.07.005 [ Links ]
21. Deka MK, Talukdar A. A retrospective analysis of bone tumors and tumor like lesions: a hospital based study of 76 cases. Int J Res Med Sci. 2017;5(11):4915. [ Links ]
22. Solooki S, Vosoughi AR, Masoomi V. Epidemiology of musculoskeletal tumorsin Shiraz, south of Iran. Indian J Med Paediatr Oncol. 2011;32(4):187-91. https://doi.org/10.4103/0971-5851.95138 [ Links ]
23. Dorfman H, Czerniak B, Kotz R, et al. Tumours of bone: introduction. WHO Classification of Tumours of Soft Tissue and Bone. 2013. p. 226-32. [ Links ]
24. Ottaviani G, Jaffe N. The epidemiology of osteosarcoma. In: Cancer Treatment and Research [Internet]. Kluwer Academic Publishers; 2009. p. 3-13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20213383 Accessed 22 March 2022. [ Links ]
25. Niu X, Xu H, Inwards CY, et al. Primary bone tumors: epidemiologic comparison of 9200 patients treated at Beijing Ji Shui Tan Hospital, Beijing, China, with 10 165 patients at Mayo Clinic, Rochester, Minnesota. Arch Pathol Lab Med. 2015;139(9):1149-55. https://doi.org/10.5858/arpa.2014-0432-oa [ Links ]
26. Freeman AK, Sumathi VP, Jeys L. Primary malignant tumours of the bone. Surg (United Kingdom). 2018;36(1):27-34. https://doi.org/10.10164.mpsur.2017.10.001 [ Links ]
27. Goedhart LM, Ho VKY, Dijkstra SPDS, et al. Bone sarcoma incidence in the Netherlands. Cancer Epidemiol. 2019;60:31-38. https://doi.org/10.10164.canep.2019.03.002 [ Links ]
28. Perera JR, Saifuddin A, Pollock R. Management of benign bone tumours. Orthop Trauma. 2017;31(3):151-60. https://doi.org/10.1016/j.mporth.2017.03.008 [ Links ]
29. Pillay Y, Ferreira N, Marais L. Primary malignant bone tumours: Epidemiological data from an orthopaedic oncology unit in South Africa. SA Orthop J. 2016;15(4):12-16. http://dx.doi.org/10.17159/2309-8309/2016/v15n4a1 [ Links ]
Received: September 2021
Accepted: December 2021
Published: August 2022
* Corresponding author: tayokoyejo@gmail.com
Editor: Dr Thomas Hilton, University of Cape Town, Cape Town, South Africa
Funding: No funding was received for the purposes of performing this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.

