










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.21 no.3 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n3a0
EDITORIAL
Artificial intelligence and spine surgery outcomes: the beginning of a new era
Evalina Burger*
Professor and Chair Robert D'Ambrosia Endowed Chair, Department of Orthopedics, University of Colorado Anschutz Medical Campus, Aurora, Colorado, United States of America

In 1950, Alan Turing believed if a machine could carry on a conversation through a teleprinter, the machine could be described as 'thinking'. In 1952, the Hodgkin-Huxley model of the brain as neurons forming an electrical network was published. At a conference sponsored by Dartmouth College in 1956, these concepts were discussed and helped to spark the concept of artificial intelligence.1,2
According to the SAS Institute (Statistical analysis system), 'Artificial intelligence (AI) makes it possible for machines to learn from experience, adjust to new inputs and perform human-like tasks'. Most AI examples that you hear about today - from chess-playing computers to self-driving cars - rely heavily on deep learning and natural language processing. Using these technologies, computers can be trained to accomplish specific tasks by processing large amounts of data and recognising patterns in the data.3
These systems will model human behaviour and thought, behave intelligently and rationally, and have applications that use techniques in machine learning, deep learning and other learning techniques. These machines can have semantic search engines (based on words) and mine data sets to find new relationships and can even recognise images. The machines' learning networks are based on pattern recognition. Arguably, these computers are smarter at cognitive problem solving, such as we find in only a small percentage of people who are smart test takers. Businesses are already using AI to predict customer behaviour, guard data and more efficiently analyse business opportunities.
So how do we use this in spine surgery and how does it help our patients? The concept is not foreign in spine surgery. Classifications have been developed for many decades in order to group together cohorts of patients that have similar disease traits. This allowed for scientific advancement as we could at least all speak the same language.
AI propels this thought process forward by utilising millions of data points to recognise patterns that we can translate in predicting outcomes for surgery. If we can accurately predict the risk factor for failure of fusion, proximal junctional kyphosis and infection, we could save many a patient from harm. Theoretically this can also help us to decide on the procedure needed to overcome failure.
Attempts at this synthetisation of mega data hold promise for us to educate our patients and make skilful unbiased decisions on the indications for and extent of surgery.4
With the embracement of technology, we can create personalised medicine. Studying multiple genetic samples at the CU-Anschutz School of Medicine (SOM), we were able to determine which patients lack the enzyme to metabolise non-steroidal anti-inflammatory drugs (NSAIDs) due to a genetic defect, hence the unpredictability of post-surgical kidney failure with administration of NSAIDs. These patients' charts were flagged.5
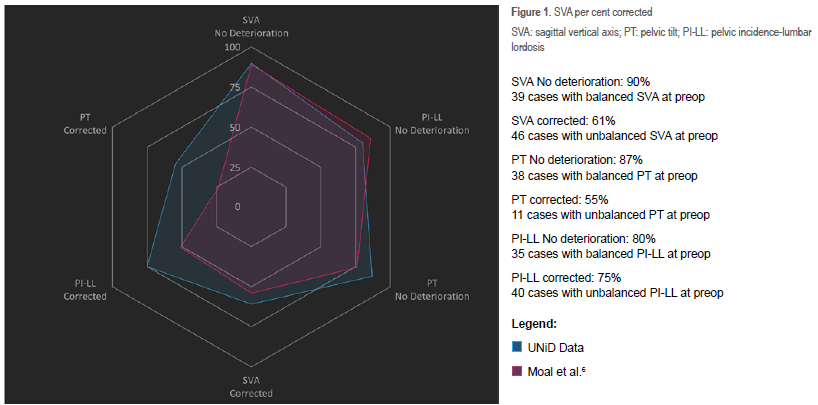
I vividly remember how I was told that 'nothing kills confidence like follow up'. When you start to incorporate data analytics into your practice and have a computer tell you outcome measures, it is sobering and really changes your thought process. Not only does it kill confidence but is unsettling and thought provoking. Figure 1 depicts a graph that is readily available and updated in real time with every patient visit and follow-up X-ray. Images are transferred to the hub where X-rays are analysed and up to 28 sagittal parameters recorded. Looking at this data, the surgery corrected the PI-LL (pelvic incidence-lumbar lordosis) value in 70% of cases (50% is standard in the literature) and showed that none of the patients that were balanced before were worsened by the surgery.7
The platform also allows for accurate planning of cases. The AI platform stores the data of thousands of patients and, via pattern rcognition, creates a predicitve model. The value in this is knowing how patients will compensate post surgery. Intuitively we know that patients will balance their spine over time. Prediction of where they will end is not only critical for the long-term outcomes but can help us to not harm the patient with over or under correcting deformity.
The example (Figure 2) is that of an unbalanced congenital curve, and planning the rod and the sagittal balance gave us the template to execute the surgery (Figure 3). These cases are complex and getting the sagittal balance correct in the face of a severe coronal deformity is always a challenge.


Figure 4 demonstrates an example of the predictive value that the model provides. We are able to see how the pelvis will relax and how much we should increase the thoracic kyphosis in order to balance the spine. This allows us to not only plan every osteomy but also order a patient-specific rod that guides the surgical correction. The rod is used as a template during surgery and the paradigm shifts to bringing the patient to the rod as opposed to placing the rod into the patient.

Collection of data on this scale will help to show value.
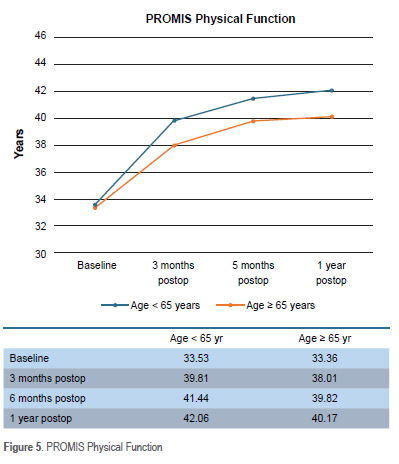
If we cannot demonstrate value-based care, we will not be able to negotiate reimbursement for what we do. In tracking our patients for functional improvement (Figure 5 and 6), the data demonstrate improvement of physical function and ODI at one year.8 This outcomes data, although generic, can be enormously valuable when we combine patient-specific outcome scores with patient-specific radiological outcomes, refining what we do to a science and not only an art.8

Many pitfalls will have to be negotiatied, including data integrity and protection of personal information. As data science evolves and platforms develop, this type of information will flow seamlessly and be available to every surgeon to constantly test their skills and push the boundaries to deliver the best care we can give to our patients. AI has found a home in medicine and surgery and will play a pivotal role in decision making in the future. The ethics of applying this knowledge in decision making has to be defined but the science will be undeniable.
References
1. Reynoso, R. A complete history of artificial intelligence. 2021. Available from: https://www.g2.com/articles/history-of-artificial-intelligence. Accessed 5 June 2022. [ Links ]
2. Foot K. A brief history of artificial intelligence. dataversity. 2022. Available from: https://www.healthdatacompass.org/#h.p_gQKTo03Q80Ri. Accessed 5 June 2022. [ Links ]
3. Knight M. What is artificial intelligence (AI)? 2021. Available from: https://www.dataversity.net/?s=What+Is+Artificial+Intelligence+%28AI%29%3F. Accessed 5 June 2022. [ Links ]
4. Ames CP, Smith Js, Pellise F, et al. Artificial intelligence based hierarchical clustering of patient types and intervention categories in adult spinal deformity surgery: towards a new classification scheme that predicts quality and value. Spine (Phila Pa 1976). 2019;44(13):915-26. https://doi.org/10.1097/brs.0000000000002974 [ Links ]
5. Colorado Center for Personalized Medicine. Infrastructure. c2022. The Regents of the University of Colorado. Available from: https://medschool.cuanschutz.edu/ccpm/infrastructure. Accessed 5 June 2022. [ Links ]
6. Moal B, Schwab F, Ames CP, et al.; International Spine Study Group. Radiographic outcomes of adult spinal deformity correction: a critical analysis of variability and failures across deformity patterns. Spine Deform. 2014;2(3):219-25. https://doi.org/10.1016/j.jspd.2014.01.003 [ Links ]
7. Available from: https://platform.medicrea.com/analytics/balance-analysis. Accessed 5 June 2022. [ Links ]
8. CU COSMOS (Colorado Orthopaedic Surgery Measurement of Outcomes System) patient outcomes data. [ Links ]
* Corresponding author: evalina.burger@cuanschutz.edu


{kind=link}