










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.21 no.2 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n2a6
CURRENT CONCEPTS REVIEW
Current concepts on the assessment of a patient with a traumatic anterior shoulder dislocation
Ntambue J Kauta*; Jean Pdu Plessis; Johannes J de Wet; Basil Vrettos; Stephen JL Roche
Adult Reconstruction, Shoulder and Elbow Unit, Groote Schuur Hospital Orthopaedic Research Unit, University of Cape Town, Cape Town, South Africa
ABSTRACT
Anterior shoulder dislocation is a common condition that most orthopaedic surgeons will have to deal with in their practice.
Nonoperative management of the initial traumatic anterior shoulder dislocation is likely to lead to a recurrent shoulder dislocation in more than 90% of cases in the younger active population. Recurrent anterior shoulder dislocation can persist even after instability surgery in certain cases. A detailed, accurate assessment of the patient is of paramount importance for successful treatment.
This review aims to provide insight into key concepts to consider in the assessment of an anterior shoulder dislocation. Predisposing factors, clinical examination and the role of imaging in the assessment of an anterior shoulder dislocation will be reviewed.
Level of evidence: Level 5
Keywords: anterior shoulder dislocation, anterior shoulder instability, recurrent shoulder dislocation, anterior shoulder instability assessment
Introduction
Anterior shoulder dislocation is the most common joint dislocation.1 Following nonoperative management of the initial episode, the recurrence rate varies from 70% to more than 90% in the adolescent population group.1-3 Recurrent instability has been reported in up to 30% of surgically treated adolescent traumatic anterior shoulder dislocation.4,5 Two-thirds of patients with recurrent dislocation will develop instability arthropathy within 25 years of the initial dislocation episode.6
There is, therefore, a need to identify patients who are likely to recur and who may need surgical stabilisation. An understanding of factors that predispose to recurrent anterior instability, a thorough clinical examination to define the instability characteristics and an analysis of bone loss pattern through imaging are the steppingstones to an appropriate treatment algorithm.
Assessment of the unstable shoulder
Risk factors for recurrence after nonoperative management of the index traumatic anterior dislocation
Well-defined factors have been recognised as independent risk factors for recurrent anterior shoulder dislocation. These factors include:
• young age at the initial dislocation3,7
• humeral or glenoid critical bone loss at initial dislocation8-11
• return to competitive contact sport activities12-15
• ligamentous laxity16-18
Recurrent dislocation after initial nonoperative management is closely related to age younger than 20 years at the time of the first dislocation.3,19 Roberts et al. prospectively observed a group of 133 adolescents who were treated nonoperatively for anterior shoulder dislocation and reported a 76% recurrence rate at two years.7
The presence and magnitude of humeral or glenoid bone loss is another consistent predisposing factor to recurrent shoulder dislocation.
An off-track Hill-Sachs lesion has been noted to predispose to recurrent dislocation in 100% of the cases. This recurrence rate drops to 58% and 27% respectively when dealing with an on-track Hill-Sachs lesion or no lesion at all in young first-time dislocators.8,9
Dickens et al. found that initial traumatic anterior shoulder dislocation could lead to minor glenoid bone loss (6.8% of the glenoid width), but this glenoid bone loss increased up to 22.8% in recurring dislocations.10
In the setting of glenoid bone loss, recurrence rates of 72% in the under 23-year-olds and 27% in the over 30-year-olds have been reported.11 Burkhart and De Beer reported that the inverted pear-shaped glenoid due to anteroinferior bone loss was associated with recurrence of instability after arthroscopic Bankart repair.20
For athletes who have been treated nonoperatively, it is accepted that return to play should be allowed after the injured shoulder has recovered more or less to equal strength and range of motion as the uninjured shoulder. This is often within two to three weeks of the dislocation.12 The rate of recurrence of anterior instability (dislocation and subluxation episodes) has been reported to vary between 30 and 90% when all professional sports are considered.12-14 Return to competitive sport is therefore considered an independent risk factor for recurrent dislocation. This risk is not only seen in nonoperative treatment but also following surgery as reported by Torrance et al., where they documented a 93% recurrence rate in rugby players younger than 16 years who had undergone an arthroscopic Bankart repair. The recurrence occurred following another traumatic event after return to play. The type of sport and the level of participation play important roles in the recurrence rate.15
The role of generalised ligamentous laxity as an independent predisposing factor for unidirectional anterior shoulder dislocation has been investigated. Some studies have suggested that generalised ligamentous laxity and increased external rotation of the shoulder to more than 85° predispose to acute and chronic shoulder injuries.16,17 Akhtar and Robinson found a 43% incidence of generalised ligamentous laxity in patients presenting with anterior shoulder dislocation suggesting that this condition could be a predisposing factor to both primary and recurrent anterior dislocation.18 Balg and Boileau21 have shown that patients with two or more of these risk factors were likely to fail an arthroscopic Bankart repair as a stabilising surgical procedure.
Clinical evaluation
The clinical examination of the unstable shoulder primarily aims to determine whether the shoulder instability is unidirectional (anterior, posterior or inferior), bidirectional (unstable in two directions) or multidirectional (unstable in more than two directions). An assessment of ligament laxity needs to be performed. Associated soft tissues injuries (capsulolabral injuries, cuff tears) and neurovascular injuries must also be assessed.
Information obtained from the clinical evaluation is as important as the information obtained from imaging in the formulation of the treatment strategy for the unstable shoulder.
Directed clinical history
Clinical history should focus on the age at the index dislocation, the mechanism of injury and ease of relocation of the index dislocation. If the index relocation did not require sedation and was relatively easy, ligamentous laxity should be suspected.
The number and frequency of recurrences as well as inciting events should be investigated. Pre-existing medical conditions such as epilepsy should be assessed for and strictly controlled before instability surgery is undertaken. Patients with more than two dislocations and limited bone loss on imaging should be assessed for a voluntary component to their instability since this may affect the management decision-making process.
Gerber and Nyffeler classified voluntary dislocators into three groups: i) dislocators without apprehension; ii) symptomatic voluntary dislocators or subluxators; and iii) psychiatric patients.22 This classification should be considered when assessing voluntary dislocators due to the failure of surgical treatment in this group.
General physical examination
The examination of the unstable shoulder begins with a comparative inspection of both shoulders (appropriately exposed) for asymmetry in shoulder contour, muscle bulk, and the presence or absence of signs of acute injury such as bruising. Inspection for scapula position is done in static and dynamic mode during range of motion to exclude subtle scapula dyskinesia. Palpation of bony prominences is done to exclude occult or missed fractures, especially of the coracoid process.
Comparative range of motion assessment is done in the most relevant planes including forward elevation, external and internal rotation with the arm to the side and the shoulder in 90° of abduction. Rotator cuff strength testing is done by isolating one muscle at a time according to standard clinical examination tests. Neurovascular assessment concludes the general examination and focuses on axillary nerve, brachial plexus assessment and pulse status.
Instability-specific examination
The specific shoulder instability evaluation starts with the assessment for generalised ligamentous hyperlaxity using the Beighton criteria.23 Specific shoulder hyperlaxity signs include a positive Walch test (shoulder external rotation of more than 90°), indicative of laxity of the anterior shoulder capsuloligamentous tissues, and positive Gagey's hyperabduction sign (more than 105° of passive abduction), indicative of inferior ligamentous laxity of the shoulder.24,25 At this step, the patient is asked to try and dislocate or subluxate their shoulder. This would help identify the habitual or voluntary dislocator.
Provocative testing is conducted to determine the direction of instability and confirm whether the patient presents with unidirectional, bidirectional or multidirectional instability.
The sulcus sign test assesses for the presence or absence of rotator interval laxity and inferior laxity. To elucidate the sulcus sign, the patient is first positioned upright with their arms resting at their side. The examiner then stabilises the shoulder and applies an inferiorly directed force on the elbow. Excessive downward displacement of the humeral head that does not improve with external rotation denotes a deficiency of the rotator interval and inferior instability.
The sulcus sign is graded by the amount of inferior translation: grade I is less than 1 cm translation, grade II is 1-2 cm translation, and grade III is greater than 2 cm translation.26 The higher the grade, the higher the degree of laxity of the rotator interval and inferior instability.
The apprehension test aims to ascertain the presence of anterior instability. As originally described by Rowe and colleagues, the test is performed either in standing or supine position, with the arm abducted 90°; the shoulder is externally rotated until the patient is apprehensive of a dislocation.27,28 Rowe et al. stated that all their patients tested positive when examined in this fashion; however, the test could be positive in other conditions with pain and weakness in the shoulder.28 The apprehension test has a specificity of 95.7-100% and a sensitivity of 50-55.6%.29,30 It has many variations, but all of them essentially aim to provoke the humeral head to go over the anterior edge of the glenoid.
The bony apprehension test is a variant of the traditional apprehension test and is used to detect bone loss, specifically, as a contributing cause of anterior glenohumeral instability.31 The test is performed with the shoulder positioned at 45° of abduction or less and at 45° of external rotation or less. A positive finding is a sensation of apprehension or symptoms of instability. The bony apprehension test has been shown to be more sensitive than preoperative plain radiographs for detecting bony lesions at time of surgery.31
The relocation test is performed for confirmation of the apprehension test. In Frank Jobe's original description of this test, the patient is supine with the shoulder over the edge of the examination table.32 The apprehension test is performed as described above; once positive apprehension or guarding (feeling of subluxation and not pain) is expressed, the examiner places a posteriorly directed force over the anterior aspect of the shoulder. The test is positive when the apprehension feeling is relieved.32,33 While the patient's shoulder is maintained in the apprehension test and a positive relocation test has been obtained, sudden removal of the examiner's relocating hand will cause a sudden apprehension feeling. This manoeuvre was described as the surprise test by Silliman and Hawkins.34 This test is a concern as the patient may dislocate and we seldom perform it.
The load and shift test evaluates the degree of shoulder laxity in the anterior to posterior plane.35 The test can be performed with the patient sitting with the arm at the side or with patient supine and the arm in 20° and 90° of abduction. The examiner grasps the patient wrist with one hand and with the other hand the examiner loads the humeral head into the glenoid fossa and pushes the humeral head forward. Translation is graded from 0 to 3. Grade 0 denotes no translation; grade 1 is translation to the glenoid rim; grade 2 is translation over the rim but humeral head reduces spontaneously; and grade 3 is translation over the rim but no spontaneous relocation.36 Tzannes and Paxinos reported that the load and shift was more positive with the arm abducted to 20 and 90° than with arm at 0° abduction with the patient sitting.37 Other variants of this test include the anterior drawer and the anterior jerk tests.38,39
Posterior instability testing must be done to exclude posterior instability before settling on the diagnosis of a unidirectional anterior instability. The jerk test, Kim test and posterior drawer tests are all common practice in the assessment of posterior instability.38,40,41
This specific shoulder assessment is concluded by assessing for associated biceps and labral pathologies. The '3-pack' examination, which includes the O'Brien sign, throwing test and bicipital tunnel palpation, has an excellent sensitivity, negative predictive value, and inter-rater reliability for comprehensive evaluation of the biceps/labral complex pathology, making it an ideal screening tool for this purpose.42
Imaging for anterior shoulder instability
It is recognised that common soft tissue injuries such as anteroinferior capsulolabral injuries (Bankart lesion) are an integral part of the pathology of anterior shoulder dislocation. The role of imaging is to detect uncommon soft tissue injuries such as humeral avulsion of the glenohumeral ligament (HAGL), superior labral anteroposterior (SLAP) lesions as well as bony lesions.
Plain radiographs (X-rays)
Plain radiography has shown a suboptimal sensitivity and reliability in the detection of glenoid and humeral bone loss, making this imaging modality a poor screening tool for bone loss in shoulder instability.43
Four standard views including a true anteroposterior view, axillary view, internally rotated and externally rotated views are initially obtained for the purpose of detecting bone loss. The diagnosis of a Hill-Sachs lesion on plain radiographs can be significantly increased if there is awareness that the internal rotation view may fail to show the injury, and if all four views are scrutinised.44 Rozing et al. demonstrated the role of a Stryker notch view in detecting Hill-Sachs lesion in their series of 27 cases.45 A loss of cortical line contour of anteroinferior glenoid on an anteroposterior view is suggestive of anteroinferior glenoid bone loss (Figure 1). Specialised views such as the West Point and Bernageau views have shown high correlation with computed tomography in detecting glenoid bone loss.46,47

Although bone loss can be detected on plain radiographs it cannot, however, be precisely measured on plain radiographs.48,49 When precise measurement of bone loss is desired, a CT scan of the affected shoulder is warranted.
Computed tomography scan (CT scan)
A three-dimensional (3D) CT scan is the gold standard for shoulder instability bone loss assessment. The humeral head subtraction technique and free body rotation of the entire scapula facilitate a precise en face sagittal oblique view of the glenoid surface. This allows accurate measurements of the magnitude of glenoid bone loss and allows for a distinction between a chronic attritional bone loss and an acute fracture. In addition, the humeral head can be rotated in different planes to visualise a Hill-Sachs lesion.50
Indications for obtaining a CT scan with 3D reconstruction on patients with shoulder instability include a history of multiple dislocations, a prior failed stabilisation procedure, relative ease of dislocation through low energy mechanisms or activities of daily living, mid-range instability, or concern for glenoid bone loss on radiographs or MRI.50
There are various methods described to assist in measuring or estimating glenoid bone loss. The first step in all methods is to establish an en face view of the glenoid on a 3D CT scan with humeral head subtraction (Figure 2). The two most common methods include the surface area loss measurements and the width loss measurements. In surface area loss measurements, a best-fit circle surface area (BCSA) is superimposed onto the affected glenoid based either on the contralateral side or based on the intact posteroinferior borders of the affected glenoid (Figure 2). In the BCSA methods, the surface area loss can be calculated using a software program or using a mathematical formula.51,52
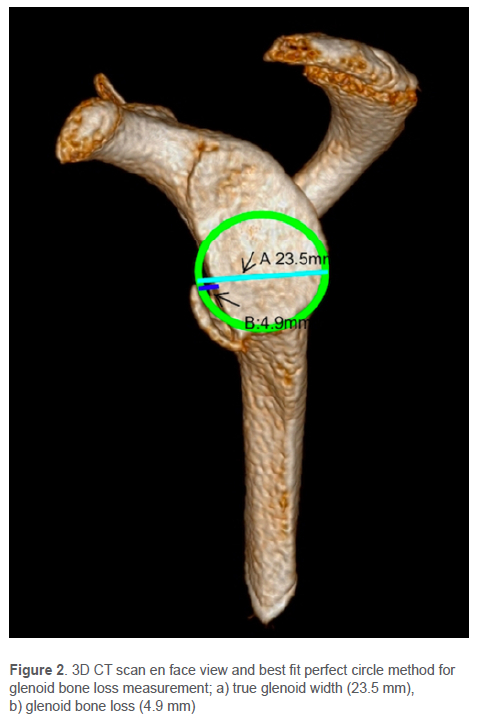
In essence, the percentage of glenoid bone loss using surface area techniques is performed by measuring the area of the true circle not occupied by the glenoid surface and dividing this area by the area of the best-fit circle. The Pico method is one example of the BCSA method commonly used. Originally described by Baudi et al., the Pico method has demonstrated good interobserver (ICC 0.90) and intraobserver (ICC0.94, 0.96-1.0) reliability as well as a low coefficient of variation (2.2-2.5 %).51,53 According to the Pico method, a perfect circle is first drawn on the inferior part of the healthy glenoid and then transferred to the injured glenoid. The surface of the missing glenoid part of the circle is measured; the size of the glenoid bone defect is expressed as a percentage of the entire circle. Width loss measurement methods measure width loss from a circle approximated to the inferior glenoid (based on either contralateral or ipsilateral glenoid) and have been found to have good reliability and accuracy (Figure 2).53,54 This is a simple calculation and advanced software calculations are not required.
Milano et al. have shown a strong correlation and agreement in detecting the presence, size and type of bone loss between referencing to the CT of the uninjured side and referencing from the posteroinferior margins of the injured glenoid.54 Parada et al. have cautioned against the use of measurement referencing from the uninjured side since their cadaveric anthropometric study showed side-to-side glenoid widths, heights and surface area were statistically different in some cadavers.55
A systematic review by Gottschalk et al. reported that several studies that had shown the limit of glenoid bone loss beyond which a Bankart repair was likely to fail varied between 20 and 25% of the glenoid width.56 Shin et al. disputed these values and showed that in their cohort, the critical glenoid bone loss value was 17.3%. Glenoid bone defect of larger surfaces than 17.3% suffered failure of arthroscopic Bankart repair.57 These glenoid bone loss critical values become irrelevant when an associated Hill-Sachs lesion is present.58
Assessment of Hill-Sachs lesions
The aim of Hill-Sachs lesion assessment is to determine whether it is an engaging lesion or not, depending on its width, length and depth. Various methods have been described and each with a different critical size above which the lesion may be deemed engaging.59-61
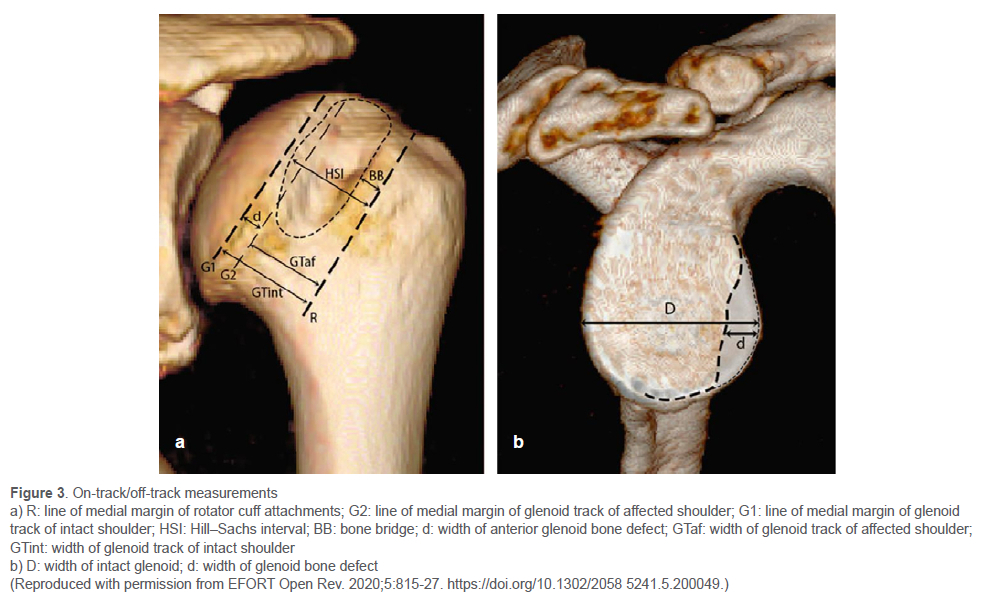
In the assessment of bifocal lesions (coexisting glenoid and humeral bone loss), the two lesions need to be assessed individually and then correlated to each other to determine whether recurrent instability or dislocation can be expected after arthroscopic soft tissue stabilising procedures. Di Giacomo et al. in 2014 introduced the on-track off-track method using CT with 3D reconstructions where lesions were considered engaging, or off track if the Hill-Sachs interval exceeded the glenoid track.61 The glenoid track consists of the contact area between the humeral head and glenoid during shoulder abduction and external rotation and it represents approximately 83% of the glenoid width. The Hill-Sachs interval represents the width of the Hill-Sachs lesion in millimetres plus the width of the intact bone bridge in millimetres between the rotator cuff attachment and the lateral margin of the Hill-Sachs lesion.
Di Giacomo et al.'s method consists of four evaluation steps: the first measures the diameter (D) of the inferior glenoid using the perfect circle method; the second measures the amount of glenoid anterior bone loss (d); the third calculates the width of the glenoid track (GT) = 0.83 χ D-d; and the last measures the width of the Hill-Sachs interval (HSI), which is the width of the Hill-Sachs lesion plus the width of the bone bridge between the lesion and the rotator cuff insertion. If HSI > GT, the lesion is off track; if HSI < GT, it is on track (Figure 3).61,62
Magnetic resonance imaging (MRI)
The routine use of MRI as a diagnostic tool in the diagnosis of anterior shoulder instability remains controversial. Despite cost and availability, the use of MRI in anterior shoulder dislocation is rising. Leland et al. reported an increased trend in the diagnosis of bony Bankart and/or Hill-Sachs on MRI, documenting an incidence of 96% in patients undergoing MRI in 2015-2018 compared to 52.9% in 1994-1999.63 The authors postulated that it may be associated with improved MRI modalities, increased focus on identifying bony Bankart and/or Hill-Sachs lesions, and increasing concern about glenoid bone loss.63
The main advantages of using an MRI scan in the setting of shoulder instability are twofold. First, it helps to exclude other soft tissue injuries, such as SLAP lesions, HAGL lesions, anterior labral periosteal sleeve avulsion (ALPSA), glenoid articular cartilage defect (GLAD), rotator cuff tendon tears and more extensive cartilaginous injuries. Secondly, it helps to confirm the diagnosis of dislocation. In patients who have had a dislocation which reduces spontaneously, there may be some uncertainty in the diagnosis. This can be confirmed on MRI scan by the presence of bony oedema in the posterior aspect of the humeral head (in the region of a Hill-Sachs lesion).
Burke et al. demonstrated glenoid bone loss measurements performed on 3D MRI reconstructions have close correlation with that of 3D CT, which is considered the gold standard.64 Leland et al. noted that MRI can estimate glenoid bone loss as accurately as CT scan.63
MR arthrography (MRA) has little or no role in the acute setting and the use of MRA has decreased over time due to the availability and quality of the modern 3T (3 tesla) MRI.64 Although not frequently used, it may still be an invaluable diagnostic tool in the young active patient with recurrent anterior shoulder instability with a subtle capsulolabral abnormality.64
Conclusion
This review outlines the role of a thorough clinical assessment and adequate imaging in identifying patients at higher risk of developing recurrent anterior shoulder instability and dislocation. Patients younger than 20 years of age, those with ligament hyperlaxity and those with considerable bone loss are at higher risk of recurrence. While the debate is still ongoing with regard to the best method to measure glenoid and humeral bone loss, a 3D CT scan remains the gold standard imaging modality to assess bone loss. The on-track vs off-track concept is the most accepted method of assessing bone loss when there is bipolar bone loss.
Awareness and identification of these risk factors during the assessment of a patient with a traumatic anterior shoulder dislocation will inform the management decision-making process and hopefully prevent recurrent dislocations and subsequent arthropathy.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. As this is a review article, no studies on humans or animals were conducted for this study. No ethics or institutional review board approval were required.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
NJK: first draft preparation, all revisions JPdP: manuscript revision JJdW: first draft preparation BV: manuscript revision SJLR: manuscript revision
ORCID
Kauta NJ https://orcid.org/0000-0002-7099
Du Plessis JP https://orcid.org/0000-0001-6469-7765
De Wet JJ https://orcid.org/0000-0001-5464-749X
Vrettos Β https://orcid.org/0000-0003-4226-0794
Roche SJL https://orcid.org/0000-0002-5695-2751
References
1. Dodson CC, Cordasco FA. Anterior glenohumeral joint dislocations. Orthop Clin North Am. 2008;39(4):507-18. https://doi.org/10.1016/j.ocl.2008.06.001. [ Links ]
2. Henry JH, Genung JA. Natural history of glenohumeral dislocation-revisited. Am J Sports Med. 1982;10(3):135-37. https://doi.org/10.1177/036354658201000301. [ Links ]
3. Bottoni CR, Wilckens JH, DeBerardino TM, et al. A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations. Am J Sports Med. 2002;30(4):576-80. https://doi.org/10.1177/03635465020300041801. [ Links ]
4. Murphy AI, Hurley ET, Hurley DJ, et al. Long-term outcomes of the arthroscopic Bankart repair: a systematic review of studies at 10-year follow-up. J Shoulder Elb Surg. 2019;28(11):2084-89. https://doi.org/10.1016/jjse.2019.04.057. [ Links ]
5. Rossi LA, Tanoira I, Gorodischer T, et al. Recurrence and revision rates with arthroscopic Bankart repair compared with the Latarjet procedure in competitive rugby players with glenohumeral instability and a glenoid bone loss <20%. Am J Sports Med. 2021;49(4):866-72. https://doi.org/10.1177/0363546520988154. [ Links ]
6. Hovelius L, Rahme H. Primary anterior dislocation of the shoulder: long-term prognosis at the age of 40 years or younger. Knee Surg Sports Traumatol Arthrosc. 2016;24(2):330-42. https://doi.org/10.1007/s00167-015-3980-2. [ Links ]
7. Roberts SB, Beattie N, McNiven ND. The natural history of primary anterior dislocation of the glenohumeral joint in adolescence. Bone Joint J. 2015;97-B(4):520-26. https://doi.org/10.1302/0301-620x.97b4.34989. [ Links ]
8. Dyrna FGE, Ludwig M, Imhoff AB, et al. Off-track Hill-Sachs lesions predispose to recurrence after nonoperative management of first-time anterior shoulder dislocations. Knee Surg Sports Traumatol Arthrosc. 2021;29(7):2289-96. https://doi.org/10.1007/s00167-020-06176-1. [ Links ]
9. Shijit KP, Sood M, Sud AD, Ghai A. Is CT scan a predictor of instability in recurrent dislocation shoulder? Chin J Traumatol. 2019;22(3):177-81. https://doi.org/10.1016/j.cjtee.2019.01.010. [ Links ]
10. Dickens JF, Slaven SE, Cameron KL, et al. Prospective evaluation of glenoid bone loss after first-time and recurrent anterior glenohumeral instability events. Am J Sports Med. 2019;47(5):1082-89. https://doi.org/10.1177/0363546519831286. [ Links ]
11. Hovelius L, Augustini BG, Fredin H, et al. Primary anterior dislocation of the shoulder in young patients. A ten-year prospective study. J Bone Joint Surg Am. 1996;78(11):1677-84. https://doi.org/10.2106/00004623-199611000-00006. [ Links ]
12. Hasebroock AW, Brinkman J, Foster L. Management of primary anterior shoulder dislocations: a narrative review. Sports Med Open. 2019;5(1):31. https://doi.org/10.1186/s40798-019-0203-2. [ Links ]
13. Watson S, Allen B, Grant JA. A clinical review of return-to-play considerations after anterior shoulder dislocation. Sports Health. 2016;8(4):336-41. https://doi.org/10.1177/1941738116651956. [ Links ]
14. Dickens F, Cameron KL, Svoboda SJ, et al. Return to play and recurrent instability after in-season anterior shoulder instability. Am J Sports Med. 2014;42(12):2842-50. https://doi.org/10.1177/0363546514553181. [ Links ]
15. Torrance E, Clark CJ, Monga P, et al. Recurrence after arthroscopic labra repair for traumatic instability in adolescent rugby and contact athletes. Am J Sports Med. 2018;46(12):2969-74. https://doi.org/10.1177/0363546518794673. [ Links ]
16. Saremi H, Yavarika A, Jafari N. Generalized ligamentous laxity: An important predisposing factor for shoulder injuries in athletes. Iran Red Crescent Med J. 2016;18(6):e38903. https://doi.org/10.5812/ircmj.38903. [ Links ]
17. Chahal J, Jeff L, McKee M, Whelan D. Generalized ligamentous laxity as a predisposing factor for primary traumatic anterior shoulder dislocation. J Shoulder Elbow Surg. 2010;19(8):1238-42. https://doi.org/10.1016/jjse.2010.02.005. [ Links ]
18. Akhtar A, Robinson CM. Generalised ligament laxity and shoulder dislocations after sports injuries. Br J Sports Med. 2010;44:i3. [ Links ]
19. Leland DP, Bernard CD, Keyt LK, et al. An age-based approach to anterior shoulder instability in patients under 40 years old: analysis of a US population. Am J Sports Med. 2020;48(1):56-62. https://doi.org/10.1177/0363546519886861. [ Links ]
20. Burkhart SS, De Beer JF. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16(7):677-94. https://doi.org/10.1053/jars.2000.17715. [ Links ]
21. Balg F, Boileau P. The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br.2007;89(11):1470-77. https://doi.org/10.1302/0301-620X.89B11.18962. [ Links ]
22. Gerber C, Nyffeler RW. Classification of glenohumeral joint instability. Clinical Orthop Relat Res. 2002;(400):65-76. Gerber C, Nyffeler RW. Classification of glenohumeral joint instability. Clinical Orthop Relat Res. 2002:400;65-76. [ Links ]
23. Smits-Engelsman B, Klerks M, Kirby A. Beighton score: a valid measure for generalized hypermobility in children. J Pediatr. 2011;158(1):119-23, 123.e1-4. https://doi.org/10.1016/j.jpeds.2010.07.021. [ Links ]
24. Walch G, Agostini J, Levigne C, Nové-Josserand L. Recurrent anterior and multidirectional instability of the shoulder. Rev Chir Orthop Reparatrice Appar Mot. 1995;81:682-90. [ Links ]
25. Gagey OJ, Gagey N. The hyperabduction test. J Bone Joint Surg Br. 2001;83(1):69-74. https://doi.org/10.1302/0301-620x.83b1.10628. [ Links ]
26. Lizzion VA, Meta F, Fidai M, et al. Clinical evaluation and physical exam findings in patients with anterior shoulder instability. Curr Rev Musculoskelet Med. 2017;10(4):434-41. https://doi.org/10.1007/s12178-017-9434-3. [ Links ]
27. Rowe CR, Zarins B. Recurrent transient subluxation of the shoulder. J Bone Joint Surg Am. 1981;63(6):863-72. [ Links ]
28. Rowe CR, Zarins B, Ciullo JV. Recurrent anterior dislocation of the shoulder after surgical repair. Apparent causes of failure and treatment. J Bone Joint Surg Am. 1984;66(2):159-68. [ Links ]
29. Jobe FW, Kvitne RS, Giangarra CE. Shoulder pain in the overhand or throwing athlete. The relationship of anterior instability and rotator cuff impingement. Orthop Rev. 1989;18(9):963-75. [ Links ]
30. Farber AJ, Castillo R, Clough M, et al. Clinical assessment of three common test for traumatic anterior shoulder instability. J Bone Joint Surg Am. 2006;88(7):1467-74. https://doi.org/10.2106/jbjs.e.00594. [ Links ]
31. Bushnell BD, Creighton RA, Herring MM. The bony apprehension test for instability of the shoulder: a prospective pilot analysis. Arthroscopy. 2008;24(9):974-82. https://doi.org/10.1016/j.arthro.2008.07.019. [ Links ]
32. Jobe FW, Gingarra CE, Kvitne RS, Glousman RE. Anterior capsulolabral reconstruction of the shoulder in athletes in overhand sports. Am J Sports Med. 1991;19(5):428-34. https://doi.org/10.1177/036354659101900502. [ Links ]
33. Speer KP, Hannafin JA, Altchek DW, Warren RF. An evaluation of shoulder relocation test. Am J Sports Med. 1994;22(2):177-83. https://doi.org/10.1177/036354659402200205. [ Links ]
34. Silliman JF, Hawkins RJ. Classification and physical diagnosis of instability of the shoulder. Clin Orthop.1993;(291):7-19. [ Links ]
35. Clarnette RG, Miniaci A. Clinical exam of the shoulder. Med Sci Sports Exerc. 1998;30(4 Suppl):S1-6. https://doi.org/10.1097/00005768-199804001-00001. [ Links ]
36. Tzannes A, Murrell GA. Clinical examination of the unstable shoulder. Sports Med. 2002;32(7):447-57. [ Links ]
37. Tzannes A, Paxinos A, Callanan M, Murrell GA. An assessment of the interexaminer reliability of tests for shoulder instability. J Shoulder Elbow Surg. 2004;13(1):18-23. https://doi.org/10.1016/j.jse.2003.09.002. [ Links ]
38. Gerber C, Ganz R. Clinical assessment of instability of the shoulder. With special reference to anterior and posterior drawer tests. J Bone Joint Surg Br. 1984;66(4):551-56. https://doi.org/10.1302/0301-620x.66b4.6746691. [ Links ]
39. Lerat JL, Chotel F, Besse JL, et al. Dynamic anterior jerk of the shoulder. A new clinical test for shoulder instability. Preliminary study. Rev Chir Orthop Reparatrice Appar Mot. 1994;80(6):461-67. [ Links ]
40. Matsen FA, Thomas SC, Rockwood CA, Wirth MA. Glenohumeral instability, in the shoulder. Philadelphia: Saunders; 1990. p. 611-755. [ Links ]
41. Kim SH, Park JS, Jeong WK, Shin SK. The Kim test: a novel test for posteroinferior labral lesion of the shoulder-- a comparison to the jerk test. Am J Sports Med. 2005;33(8):1188-92. https://doi.org/10.1177/0363546504272687. [ Links ]
42. Taylor SA, Newman AM, Dawson C, et al. The '3-pack' examination is critical for comprehensive evaluation of the biceps-labrum complex and the bicipital tunnel: a prospective study. Arthroscopy. 2017;33(1):28-38. https://doi.org/10.1016/j.arthro.2016.05.015. [ Links ]
43. Royle Ad, Balg F, Bouliane MJ, et al. Sensitivity and specificity of standard radiographs to predict bone defects after traumatic anterior glenohumeral instability. Am J Sports Med. 2017;5(10):2325967117733660. https://doi.org/10.1177/2325967117733660. [ Links ]
44. Riebe B, Micheas L, Crim J. Improving detection of Hill-Sachs fractures on radiographs. Skelet Radiol. 2021;50(9):1889-97. https://doi.org/10.1007/s00256-021-03763-2. [ Links ]
45. Rozing PM, De Bakker HM, Obermann WR. Radiographic views in recurrent anterior shoulder dislocation: comparison of six methods for identification of typical lesions. Acta Orthop Scand. 1986;57(4):328-30. https://doi.org/10.3109/17453678608994403. [ Links ]
46. Itoi E, Lee SB, Amrami KK, et al. Quantitative assessment of classic anteroinferior bony Bankart lesions by radiography and computed tomography. Am J Sports Med. 2003;31(1):112-18. https://doi.org/10.1177/03635465030310010301. [ Links ]
47. Edwards TB, Boulahia A, Walch G. Radiographic analysis of bone defects in chronic anterior shoulderinstability. Arthroscopy. 2003;19(7):732-39. https://doi.org/10.1016/s0749-8063(03)00684-4. [ Links ]
48. Itoi E, Lee SB, Amrami KK, et al. Quantitative assessment of classic anteroinferior bony Bankart lesions by radiography and computed tomography. Am J Sports Med. 2003;31(1):112-118. https://doi.org/10.1177/03635465030310010301. [ Links ]
49. Saliken DJ, Bornes TD, Bouliane MJ, et al. Imaging methods for quantifying glenoid and Hill-Sachs bone loss in traumatic instability of the shoulder: a scoping review. BMC Musculoskelet Disord. 2015;16:164. https://doi.org/10.1186/s12891-015-0607-1. [ Links ]
50. Provencher MT, Bhatia S, Ghodadra NS, et al. Recurrent shoulder instability: Current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg Am. 2010;92(Suppl 2):133-51. https://doi.org/10.2106/JBJSJ.00906. [ Links ]
51. Magarelli N, Milano G, Sergio P, et al. Intra-observer and interobserver reliability of the 'pico' computed tomography method for quantification of glenoid bone defect in anterior shoulder instability. Skeletal Radiol. 2009;38(1):1071-75. https://doi.org/10.1007/s00256-009-0719-5. [ Links ]
52. Barchilon VS, Kotz E, Barchilon Ben-Av M, et al. A simple method for quantitative evaluation of the missing area of the anterior glenoid in anterior instability of the glenohumeral joint. Skeletal Radiol. 2008;37(8):731-36. https://doi.org/10.1007/s00256-008-0506-8. [ Links ]
53. Baudi P, Righi P, Bolognesi D, et al. How to identify and calculate glenoid bone deficit. Chir Organi Mov. 2005;90(2):145-52. [ Links ]
54. Milano G, Saccomanno MF, Magarelli M, Bonomo L. Analysis of agreement between computed tomography measurements of the glenoid bone defects in anterior shoulder instability with and without comparison with the contralateral shoulder. Am J Sports Med. 2015;43(12):2918-26. https://doi.org/10.1177/0363546515608167. [ Links ]
55. Parada SA, Paynter JW, Pare DW, et al. Use of contralateral glenoid for calculation of glenoid bone loss. Arthroscopy. 2020;36(6):1517-22. https://doi.org/10.1016/j.arthro.2020.01.049. [ Links ]
56. Gottschalk LJ IV, Bois AJ, Shelby MA, et al. Mean glenoid defect size and location associated with anterior shoulder instability: a systematic review. Orthop J Sports Med. 2017;5(1):2325967116676269. https://doi.org/10.1177/2325967116676269. [ Links ]
57. Shin SJ, Kim RG, Jeon YS. Critical value of anterior glenoid bone loss that leads to recurrent instability after Bankart repair. Am J Sports Med. 2017;45(9):1975-81. https://doi.org/10.1177/0363546517697963. [ Links ]
58. Gowd AK, Liu JN, Cabarcas BC. Management of recurrent shoulder instability with bipolar bone loss. A systematic review to assess critical bone loss amounts. Am J Sports Med. 2019;47(10):2484-93. https://doi.org/10.1177/0363546518791555. [ Links ]
59. Gyftopoulos S, Hasan S, Bencardino J, et al. Diagnostic accuracy of MRI in the measurement of glenoid bone loss. AJR Am J Roentgenol. 2012;199(4):873-78. https://doi.org/10.2214/ajr.11.7639. [ Links ]
60. Maio M, Sarmento M, Moura N, Cartusho A. How to measure a Hill-Sachs lesion. A systematic review. EFORT Open Rev. 2019;4(4):151-57. https://doi.org/10.1302/2058-5241.4.180031. [ Links ]
61. Di Giacomo G, Itoi E, Burkhart SS. Evolving concept of bipolar bone loss and the HillSachs lesion: from 'engaging/non-engaging' lesion to 'on-track/off-track' lesion. Arthroscopy. 2014;30(1):90-98. https://doi.org/10.1016/j.arthro.2013.10.004. [ Links ]
62. Di Giacomo G, De Gasperis N, Scarso P. Bipolar bone defect in the shoulder anterior dislocation. Knee Surg Sports Traumatol Arthrosc. 2016;24(2):479-88. https://doi.org/10.1007/s00167-015-3927-7. [ Links ]
63. Leland DP, Parkes CW, Bernard CD, et al. Significant changes in the diagnosis, injury severity and treatment for anterior shoulder instability over time in a US population. Arthrosc Sports Med Rehabil. 2020;2(6):e761-69. https://doi.org/10.10164.asmr.2020.06.012. [ Links ]
64. Burke CJ, Rodrigues TC, Gyftopoulos S. Anterior instability: what to look for. Magn Reson Imaging Clin N Am. 2020;28(2):195-209. https://doi.org/10.1016/j.mric.2019.12.004. [ Links ]
Received: October 2021
Accepted: February 2022
Published: May 2022
* Corresponding author: jimmy.kauta@uct.ac.za
Editor: Dr Cameron Anley, Stellenbosch University, Cape Town, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}