










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.21 no.2 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n2a4
RESEARCH
Orthopaedic research in Zimbabwe: a seminal bibliometric analysis
Cosmas SibindiI, *; Akimu MagezaII; Adrienne SocciIII
IMedical student, Yale School of Medicine, New Haven, Connecticut, United States of America
IIParirenyatwa Group of Hospitals and University of Zimbabwe, Harare, Zimbabwe
IIIDepartment of Orthopaedics, Yale School of Medicine, New Haven, Connecticut, United States of America
ABSTRACT
BACKGROUND: To provide a bibliometric analysis of published orthopaedic research in the form of peer-reviewed articles as well as non-indexed articles from Zimbabwe in the past six decades.
METHODS: We carried out a literature search of the 'Clarivariate Analytics' Web of Science database, specific journals not included in the database and the University of Zimbabwe repository. We then selected articles focused on research in orthopaedic pathology in Zimbabwe. These articles were then classified by year of publication; focus of research; first and last author country of origin; collaboration type between high-, middle- and low-income countries; journal title; journal country; methodology; and level of evidence.
RESULTS: A total of 27 articles published from 1965 to 2020 were found in the search with 26 having a single focus of research and one multiple foci. The highest focus of research was osteoporosis with six articles (22%), while trauma was second with five articles (19%). A majority, 19/27 (70%), of studies had a first author from Zimbabwe, while a plurality, 10/27 (37%), had a Zimbabwean last author. Most collaborations, 12/27 (44%), were high-income-low-income countries, with most studies being concomitantly published in the United States, 13/27 (48%). Cross-sectional descriptive studies represented the most common methodology with 13/27 articles carried out in this method (48%). The majority of these articles, 14/27 (52%), represented a low level of evidence at level 4, while 11/27 articles (41%) of articles were of a high level of evidence (levels 1 or 2).
CONCLUSION: There is a limited amount of published orthopaedic surgery research work from Zimbabwe, highlighting the need for more and higher quality research from Zimbabwe. Among different models, partnerships between Zimbabwean researchers and researchers from other international institutions appear to be the most productive in terms of research output and hence should be replicated more broadly.
Level of evidence: Level 4
Keywords: orthopaedic surgery research, bibliometric analysis, research collaborations, Zimbabwe, Africa
Introduction
Musculoskeletal pathology accounts for an increasing proportion of deaths in sub-Saharan low- and middle-income countries (LMICs) as other leading causes of death such as communicable diseases have been effectively targeted.1,2 Musculoskeletal pathology, specifically due to road traffic injuries (high-energy trauma), has also experienced an absolute increase in incidence due to increased motorised vehicle use in an environment of limited infrastructure and lax traffic law enforcement.3,4 Trauma and other musculoskeletal pathology, which require orthopaedic surgery for definitive management, are particularly concerning as already limited surgical capacity has not grown at the same rate to face the increased incidence of the orthopaedic trauma.4 Murray et al. projected in 1997 that by 2020, up to seven out of ten deaths would be due to non-communicable diseases (NCDs), with motor vehicle accidents accounting for a significant portion in LMICs, a fact already seen in individual country studies.2,5,6 Zimbabwe is one such country facing a trauma epidemic in sub-Saharan Africa.
While increasing surgical capacity represents the most salient aspect of addressing this orthopaedic trauma epidemic, training programmes and associated orthopaedic research in these programmes complement this effort.7 Training provides for the next generation of surgeons.7,8 Research, on the other hand, allows for stakeholders to craft better-aligned local solutions as well as guide policy decision making. For instance, trauma registries and protocols as well as resource allocation guidelines developed in high-income countries may not be applicable to a local Zimbabwean environment.7 As such, orthopaedic surgery research in Zimbabwe can be expected to generate output with immediate relevance to Zimbabwean surgeons and other clinicians.
According to Hedt-Gauthier et al., orthopaedic surgery research in LMICs can proceed in three main partnerships: local research only, LMIC-LMIC partnership or high-income country to low- and middle-income country collaboration (HIC-LMIC).9 All models are utilised in most countries as they allow for knowledge sharing in complex projects via HIC-LIC collaboration and increased independence of local researchers in LMIC-LMIC partnerships. In the most recent survey of orthopaedic surgery research using Web of Science, Graham et al. found only four peer-reviewed papers from Zimbabwe.10 The nature of the collaborations involved was not explored. With such limited research, a bibliometric analysis of existing literature provides a deeper view of the orthopaedic research work from the country showing specific numbers in areas of active research and potential collaboration, current partnership trends and providing guidance for research questions.7
To our knowledge, there has been no bibliometric analysis work looking at research work on musculoskeletal disease and specifically orthopaedic surgery only from Zimbabwe. With the increasing rates of musculoskeletal disease and orthopaedic trauma; increased resources dedicated to the same; increased training of Zimbabwean clinicians into orthopaedic specialist surgeons through the College of East, Central and Southern African Surgeons Association (COSECSA); and the increased likelihood of a postgraduate training programme being established in Zimbabwe, there is a clear need for a review of the current state of orthopaedic research in Zimbabwe.
This paper aims to provide a bibliometric analysis of published orthopaedic research in the form of peer-reviewed articles as well as non-indexed articles from Zimbabwe in the past six decades. It explores the numbers, author origins, nature of partnerships and orthopaedic subspecialties for this research work. It then discusses areas of current collaboration as well as areas that are in urgent need of increased research. We hypothesise that there will be a small body of orthopaedic surgery work following research trends seen in other LICs along the metrics such as author origins, research focus and methodology.
Methods and materials
We carried out a literature search of the 'Clarivariate Analytics' Web of Science database for indexed studies published in all years up to and including in 2020. We also searched journals which are not included in the Web of Science website, specifically Tropical Doctor, and the East and Central African Journal of Surgery, where articles may have been published. We also searched the University of Zimbabwe online academic repository for thesis articles as it was the only institution with a medical school until 2009, the only one with an accessible online portal and also the one with the most developed surgery faculty.
We searched in English using the terms: orthopaedics or orthopedics or musculoskeletal or trauma or surgery or bone or spine or hip or knee or neck or shoulder or pelvis. We then Altered by the research material country of origin for Zimbabwe as well as selected for medical categories excluding non-medical categories. We included articles whose area of research work was Zimbabwe regardless of author origin. In spite of this, all the articles we found had at least one author from Zimbabwe. This process is shown in the flow chart in Figure 1.
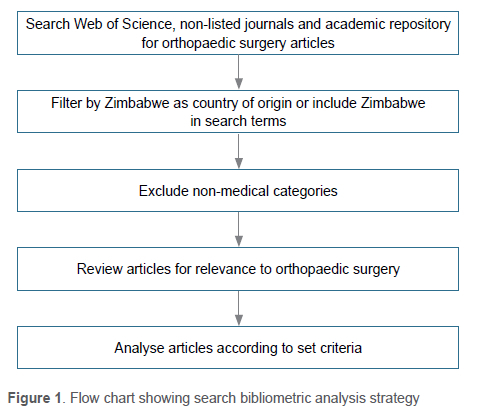
Although VOSviewer software was utilised to visualise data networks, the number of included papers was too limited to contribute any value to the analysis.11 As such, we read the articles individually to determine their relevance to orthopaedic surgery versus other medical areas. This was carried out initially by a medical student and then by two orthopaedic surgeons with a broad focus on articles examining orthopaedic pathology and orthopaedic surgery. These were then reviewed identifying for each article, the title, year of publication, first and last author country of origin, collaboration type as between high-income countries (HIC), middle-income countries (MIC) or low-income countries (LIC), journal title, journal country of publication, focus of research, methodology and level of evidence.12 The foci of research were based mainly on orthopaedic subspecialities: trauma, spine, paediatrics, sports medicine, foot and ankle, hand surgery and limb reconstruction. We also had a distinct field titled HIV-related pathology which combined research on osteoporosis, bone mineral density and monoarticular arthritis as these distinct orthopaedic topics were all researched and related to HIV/AIDS infection. Paediatrics was labelled as 'paediatric-clubfoot' specifically as it reflects all but one article in the field of paediatric orthopaedics in Zimbabwe. The authors' country of origin was established by looking at the primary affiliation of the author's location. Country income status was determined using World Bank classifications as of 2020 with income less than $1 035 representing low-income status, $1 035 to $12 535 middle income and above $12 535 representing high-income status.13
Results
Quantity and foci of research
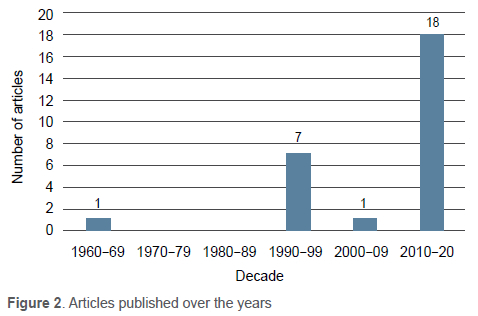
Twenty-seven articles were identified which had research focused on orthopaedic surgery research in Zimbabwe. Twenty-four articles were from indexed journals, two from non-indexed journals and one identified as a thesis. They ranged in years from 1965-2020. The highest decade of research productivity was 2010-2020, with 18 articles published, while the period 1970-1989 had no indexed articles. There was a significant drop from seven articles in 1990-1999 to only one article in 2000-2009 (Figure 2). Notably, there was an Oxford-University of Zimbabwe clubfoot research collaboration to introduce the Ponseti method led by Professor Christopher Lavy and graduate students at the time, that led to a total of three out of the four articles within paediatric orthopaedics.
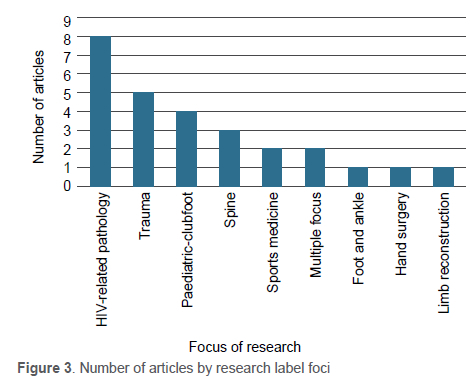
Twenty-seven papers had a singular focus under orthopaedic surgery, while one had multiple foci. The highest focus of research was HIV-related pathology with eight articles while trauma was second with five articles (Figure 3).
Levels of evidence and methodology
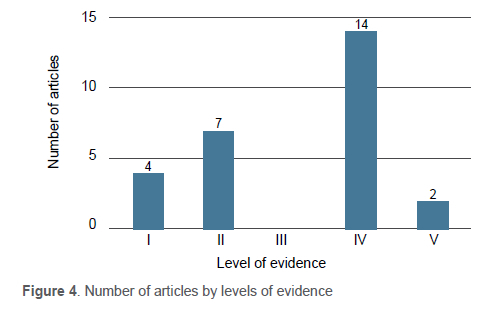
There was a broad distribution of articles by levels of evidence. The majority of articles were of a lower level of evidence (levels 4 and 5). Most articles showed level 4 evidence, while there were four level 1 articles (Figure 4).
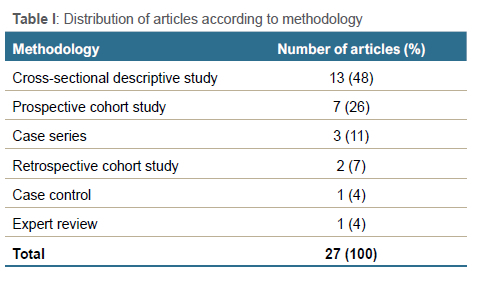
Most papers (14/27) relied on cross-sectional descriptive methodology, with prospective cohort studies representing the second-largest proportion at 7/27 articles. There were no randomised clinical trials identified (Table I).
Author origins
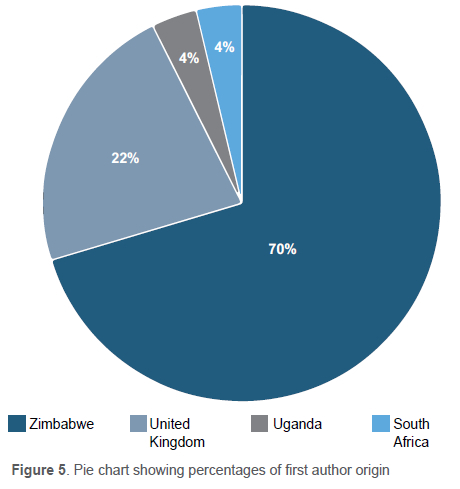
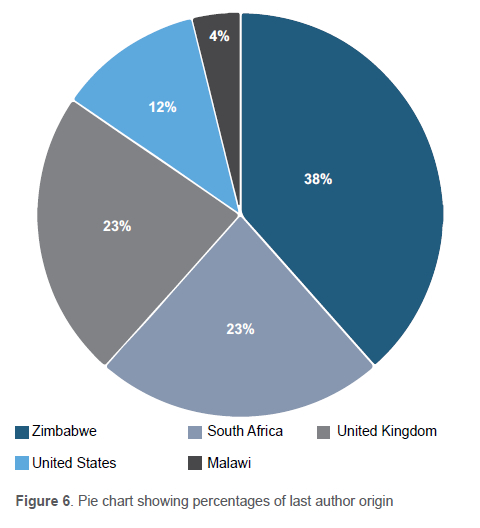
The majority of papers (19/27) were first authored by Zimbabwean authors with six papers from the United Kingdom (UK) and one each from Uganda and South Africa. There was a Zimbabwean last author for a plurality of articles (10/26). South Africa and the UK each had six last authors, with the United States (US) having three and Malawi one. There were only 26 papers under the last author designation as one of the papers had only one author (Figures 5 and 6).
We also found the countries that collaborated the most with Zimbabwean authors on orthopaedic research articles aligned directly with the last author origin for the articles, for example, if the last author was from South Africa, then the article country of collaboration would be South Africa.
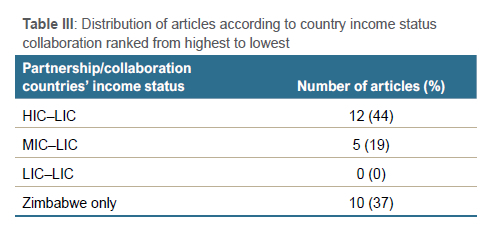
Partnerships and collaborations
There were 12 collaborations between Zimbabwean authors and HICs and five with MICs. While there were no LIC-LIC collaborations, there were 10/27 papers authored solely by Zimbabwean authors.
These articles were published in 23 different journals, with the highest number (3/27) being at the University of Zimbabwe-based Central African Journal of Medicine. The joint highest numbers beyond Zimbabwe were at the Archives of Osteoporosis and BME Musculoskeletal Disorders (2/27).
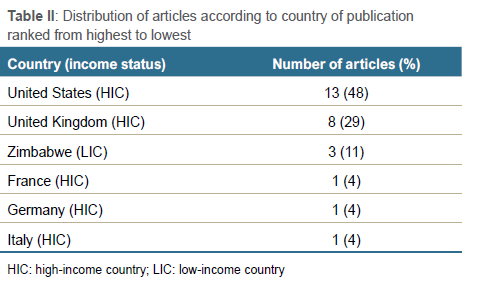
In terms of country income status, most articles (13/27) were published in US-based journals and UK-based journals (8/27), both HICs, with only three articles published in an LIC-based journal, Zimbabwe.
Discussion
We provide here a seminal bibliometric analysis on orthopaedic surgery research work from Zimbabwe. As hypothesised, the overall orthopaedic research output represents a low number of publications researched using lower levels of evidence methodologies. Due to this limited number of publications, classic bibliometric analysis techniques had significantly limited applicability. Broadly, the research work has been appropriately dominated by work focused on HIV/AIDS and antiretroviral therapy-related orthopaedic pathology (Figure 3). Beyond this, there is no commensurate increase in other research foci, specifically trauma, in recent years to address the growing trauma epidemic. While Zimbabwe had a higher proportion of both Zimbabwean first-authored articles as well as Zimbabwean published articles compared to LMIC average proportions, according to Graham et al.,10 the overwhelming majority of articles were still published in HIC-based journals (Table II). However, the authorship proportion drops significantly when looking at last author origin suggesting the prevalence of Zimbabwe-HIC collaborations as being the backbone of most publications. In this light, South Africa and the UK are clearly the most frequent collaborators, although there are a growing number of collaborations from other English-speaking nations such as the US and Canada.
The limited number of orthopaedic publications was the most salient finding in this study. According to the latest World Bank data, Zimbabwe has only 0.2 doctors per 1 000 people, while HICs like the US have an over ten-fold higher rate, at 2.74 doctors per 1 000 people.14 This ratio places pressure on surgeons and trainees to be more focused on clinical work.15 This, paired with the fact that Zimbabwe did not have an orthopaedic training programme until COSECSA inaugurated its training programme in 1999, is the likely explanation for the significantly limited quantity and quality of research articles and, more generally, academic research productivity.7,16,17
In terms of research foci, HIV-related pathology is appropriately the highest focus as a consequence of Zimbabwe and the southern African region having a high HIV/AIDS prevalence rate. Accounting for this, trauma being the second-highest focus of research is consistent with other LMICs as found by Graham et al. as well as other studies.10,18 The other trends in research work such as levels of evidence, methodology and authorship also followed a pattern similar to that seen in other LMICs.18 Regardless of the limited body of work, the distribution across foci was similar to other LMICs suggesting that the research output needs to increase across all foci rather than particular ones.10 The noted longitudinal Oxford-University of Zimbabwe clubfoot collaboration which generated both improved clinical benefit for patients as well as research output on clubfoot can be considered a model to undertake such increases.19 Indeed, such longitudinal academic collaborations have been identified by the Lancet Global Surgery and other systematic reviews as some models to boost both the clinical and research capacity of LICs such as Zimbabwe.7,20 It can be expected that adoption of this model across more fields by HICs considering work in Zimbabwe as well as Zimbabwean researchers looking to partner with HIC partners would lead to increased research output.
With regard to partners, South Africa and the UK were Zimbabwe's largest collaborators as represented in authorship, most likely because of the strong academic ties between these countries as a consequence of geographic and colonial relationships, respectively.21,22 South Africa has historically aided with Zimbabwean academic development due to the geographical and political proximity of the two countries as members of the Southern African Development Community (SADC).23 The partnership with the UK is consistent with trends seen in other countries such as Kenya which were colonised by the UK and is similarly seen in Francophone countries, with France.22 Such ties need to be nurtured, especially if they remain equitable and build Zimbabwean research capacity while maintaining a clinical impact such as the clubfoot programme. In line with these trends, and looking at evidence from multiple studies, Zimbabwean researchers should continue pursuing collaborations with other English-speaking countries as the shared language and background enhances collaboration productivity.24,25
The nature of research methodology with cross-sectional descriptive studies (Table I) of a lower level of evidence being the most common is consistent with trends in other LMICs.10,20,26 This is likely to be due to a number of factors common to LMICs. For instance, like most LMICs, Zimbabwe has only just begun implementing a national electronic medical record.27 This paired with the absence of a dedicated orthopaedic faculty as well as a complement of experienced research staff hinders longitudinal research, favouring cross-sectional or retrospective studies. The two longitudinal prospective cohort studies that were carried out corroborate these explanations as they were carried out under well-funded and staffed HIV-research programmes looking into HIV-related orthopaedic pathology or the Oxford-clubfoot longitudinal collaboration (HIC-LIC).19,28 It can be hoped that infrastructure and lessons related to HIV/AIDS-related research could be utilised in the future for other fields of research in Zimbabwe, including orthopaedics. On the other hand, HIC-LIC partnerships were found by Wu et al.26 to be associated with higher quality and quantity of output providing more support for their promise in increasing orthopaedic research methodology and level of evidence quality in Zimbabwe.
With literature showing that the majority of funding HIC-LIC collaborations comes from HICs, the significant drop in the proportion of authorships when considering the first author versus the last author can be better understood.29,30 The last author is normally a senior author leading the team with funding and intellectual contributions while the first author carries out most of the day-to-day research.31 As such, the funding from HIC leads to more last authors from HICs. Outside of funding, the absence of a dedicated orthopaedic faculty in Zimbabwe also leads to the absence of local mentors for trainees, leading to more international mentors and hence international last authors.7 It is hoped that these first authors, mostly trainees, will one day become faculty and provide local Zimbabwe-based mentorship, growing the local orthopaedic research ecosystem and increasing last name authorship. More support can be provided to these early career researchers with a view to increase research productivity in the long run.
Over a third of articles were authored by Zimbabwe-based authors only (Table III). These proportions are also consistent with those found by Graham et al. for LMICs globally.10 However, this trend in articles by Zimbabwean-only authors drops precipitously with Zimbabwean economic output which dropped in the 2000-2009 decade (Figure 2). Additionally, most of these exclusively Zimbabwean papers were from the decades earlier than 2000 when the country had a higher GDP per capita.32 This suggests that there has been some local funding for research work, most likely through governmental sources or better economic prosperity driving some Zimbabwean-based private-funded research work. This scenario suggests the need for the development of robust local research funding systems which can be more insulated from economic shocks allowing Zimbabwean orthopaedic research to consistently flourish.
While our findings results are based on Zimbabwe, it can expected that similar findings would be seen in countries of similar LIC profile. As Wu et al.26 have found, successful models for academic productivity are similar, mainly centred on HIC-LIC partnerships. We also speculate that reasons proffered for research constraints would be applicable to other such nations. While it is clear from this study that there is an aggregate need for increased research across all fields in Zimbabwe, limited resources constrain this. Given this constraint, an area of future work could ascertain prioritisation of the fields within orthopaedic surgery for research, likely through interviews with orthopaedic surgeons and other stakeholders supported by more data on Zimbabwe's needs.
Our study was limited by a few factors. First, since our search was carried out using the Web of Science portal with articles Altered by geographic origin of Zimbabwe, we may have missed articles published on Zimbabwe but not tagged on the geographic origin. In a similar vein, we could also have missed articles published in other languages and not translated into English. Second, while we were able to access the repository for the University of Zimbabwe theses, the sole medical school in the country until 2009, we were not able to And any papers. It is possible that we missed some theses which have not been digitised or were stored in other ways. Third, in conversations with local orthopaedic surgeons, we also learnt about a number of projects which are not published in peer-reviewed journals or repositories but were presented at local meetings. These unpublished works also represent a limitation to developing an accurate picture of orthopaedic projects carried out in Zimbabwe. Lastly, we utilised liberal criteria to classify articles as being related to orthopaedic surgery centred on their examination of orthopaedic pathology versus strictly surgical work. This liberal classification may lead to differences in results with other articles examining orthopaedic work but we felt such liberal criteria were key for a seminal work on which more studies can then be built.
Conclusion
To our knowledge, this is the first bibliometric analysis of orthopaedic surgery research from Zimbabwe. Our analysis shows that there is a limited amount of published orthopaedic surgery research work from Zimbabwe, highlighting the need for more and higher quality research from Zimbabwe across all foci of research. Among different models, partnerships between Zimbabwean researchers and researchers from other international institutions appear to be the most productive in terms of research output and hence should be replicated more broadly. Lastly, while there are many first authors who are Zimbabwe-based, there is also a need for an increased proportion of Zimbabwe-based last authors, suggesting a need for more locally devised work and sustainable ways of supporting such research.
Acknowledgements
We thank the Yale School of Medicine Medical Student Research Fellowship for funding part of this study.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. No ethical review was required for this bibliometric analysis of existing published literature, with no human subjects involved.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
CS: study conceptualisation, design, data analysis and manuscript preparation AM: study conceptualisation, design, data analysis and manuscript preparation AS: study conceptualisation, design, data analysis and manuscript preparation
ORCID
Sibindi C https://orcid.org/0000-0003-2424-2904
Mageza A https://orcid.org/0000-0002-1505-586X
Socci A https://orcid.org/0000-0001-9935-6928
References
1. Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet. 2007;370(9603):1929-38. https://doi.org/10.1016/s0140-6736(07)61696-1. [ Links ]
2. Haagsma JA, Graetz N, Bolliger I, et al. The global burden of Injury: Incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj Prev. 2016;22(1):3-18. https://doi.org/10.1136/injuryprev-2015-041616. [ Links ]
3. Beveridge M, Howard A. The burden of orthopaedic disease in developing countries. J Bone Joint Surg Am. 2004;86(8):1819-22. https://doi.org/10.2106/00004623-200408000-00029. [ Links ]
4. Mock C, Cherian MN. The global burden of musculoskeletal injuries: challenges and solutions. Clin Orthop Relat Res. 2008;466(10):2306-16. https://doi.org/10.1007/s11999-008-0416-z. [ Links ]
5. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study. Lancet. 1997;349(9064):1498-504. https://doi.org/10.1016/s0140-6736(96)07492-2. [ Links ]
6. Stewart KA, Groen RS, Kamara TB, Farahzad MM, Samai M, Cassidy LD, Kushner AL, Wren SM. Traumatic injuries in developing countries: report from a nationwide cross-sectional survey of Sierra Leone. JAMA Surg. 2013;148(5):463-69. https://doi.org/10.1001/jamasurg.2013.1341. [ Links ]
7. Meara JG, Leather AJ, Hagander L, Alkire BC, Alonso N, Ameh EA, Bickler SW, Conteh L, Dare AJ, Davies J. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569-624. https://doi.org/10.1016/s0140-6736(15)60160-x. [ Links ]
8. Jain AK. Orthopedic services and training at a crossroads in developing countries. Indian J Orthop. 2007;41(3):177-79. https://doi.org/10.4103/0019-5413.33677. [ Links ]
9. Hedt-Gauthier BL, Riviello R, Nkurunziza T, Kateera F. Growing research in global surgery with an eye towards equity. Br J Surg. 2019;106:e151-55. https://doi.org/10.1002/bjs.11066. [ Links ]
10. Graham SM, Brennan C, Laubscher M, Maqungo S, Lalloo DG, Perry DC, Mkandawire N, Harrison WJ. Orthopaedic research in low-income countries: A bibliometric analysis of the current literature. SICOT J. 2019;5:41. https://doi.org/10.1051/sicotj/2019038. [ Links ]
11. Van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523-38. https://doi.org/10.1007/s11192-009-0146-3. [ Links ]
12. Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. 2011;128(1):305-10. https://doi.org/10.1097/prs.0b013e318219c171. [ Links ]
13. World Bank. 4 December 2020. Country Classification. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. [ Links ]
14. World Bank. 4 December 2020. Physicians (per 1000 people). Available from: https://data.worldbank.org/indicator/SH.MED.PHYS.ZS?locations=ZW. [ Links ]
15. Sun J, Ding R, Ma T, Shi X, Bao C, Guan H. Worldwide research productivity in fracture surgery: A 10-year survey of publication activity. Exp Ther Med. 2017;14(2):1260-64. https://doi.org/10.3892/etm.2017.4585. [ Links ]
16. Kakande I, Mkandawire N, Thompson M. A review of surgical capacity and surgical education programmes in the COSECSA region. ECAJS. 2011;16:6-34. [ Links ]
17. Wang H, Chu MWA, Dubois L. Variability in research productivity among Canadian surgical specialties. Can J Surg. 2021;64(1):E76-83. https://doi.org/10.1503/cjs.016319. [ Links ]
18. Elharram M, Pauyo T, Coughlin R, Bergeron S. Trends, deficiencies and levels of evidence of orthopaedic research in low-income countries: a systematic review. Orthop Proc. 2016;98-B(Suppl 20). [ Links ]
19. Smythe T, Gova M, Muzarurwi R, Foster A, Lavy C. A comparison of outcome measures used to report clubfoot treatment with the Ponseti method: results from a cohort in Harare, Zimbabwe. BMC Musculoskeletl Disord. 2018;19(1):450. https://doi.org/10.1186/s12891-018-2365-3. [ Links ]
20. Franzen SR, Chandler C, Lang T. Health research capacity development in low and middle income countries: reality or rhetoric? A systematic meta-narrative review of the qualitative literature. BMJ Open. 2017;7(1):e012332. https://doi.org/10.1136/bmjopen-2016-012332. [ Links ]
21. Eichbaum QG, Adams LV, Evert J, Ho MJ, Semali IA, Van Schalkwyk SC. Decolonizing global health education: rethinking institutional partnerships and approaches. Acad Med. 2021;96(3):329-35. https://doi.org/10.1097/acm.0000000000003473. [ Links ]
22. Boshoff N. Neo-colonialism and research collaboration in Central Africa. Scientometrics. 2009;81:413. [ Links ]
23. Mhlanga S, Matope S, Mugwagwa L, Phuthi N, Moyo VS. Academic staff development strategies in engineering fields of study: case study of Zimbabwe. 2013. Proceedings of the 2nd Biennial Conference of the South African Society for Engineering Education, Cape Town. [ Links ]
24. Hoekman J, Frenken K, Tijssen RJ. Research collaboration at a distance: Changing spatial patterns of scientific collaboration within Europe. Res Policy. 2010;39:662-73. [ Links ]
25. Hou L, Pan Y, Zhu JJ. Impact of scientific, economic, geopolitical, and cultural factors on international research collaboration. J Informetr. 2021;15:101194. [ Links ]
26. Wu HH, Liu M, Patel KR, Turner W, Baltus L, Caldwell AM, Hahn JC, Coughlin RR, Morshed S, Miclau T, Shearer DW. Impact of academic collaboration and quality of clinical orthopaedic research conducted in low- and middle-income countries. SICOT J. 2017;3:6. https://doi.org/10.1051/sicotj/2016042. [ Links ]
27. Ministry of Health and Child Welfare. Zimbabwe Electronic Health Records. February 2016. Available from: https://apps.mohcc.gov.zw/mrs-docs/. Accessed 28 March 2022. [ Links ]
28. Rukuni R, Gregson C, Kahari C, Kowo F, McHugh G, Munyati S, Mujuru H, Ward K, Filteau S, Rehman AM, Ferrand R. The IMpact of Vertical HIV infection on child and Adolescent SKeletal development in Harare, Zimbabwe (IMVASK Study): a protocol for a prospective cohort study. BMJ Open. 2020;10(2):e031792. https://doi.org/10.1136/bmjopen-2019-031792. [ Links ]
29. Rees CA, Lukolyo H, Keating EM, Dearden KA, Luboga SA, Schutze GE, Kazembe PN. Authorship in paediatric research conducted in low-and middle-income countries: parity or parasitism? Trop Med Int Health. 2017;22(11):1362-70. https://doi.org/10.1111/tmi.12966. [ Links ]
30. Kelaher M, Ng L, Knight K, Rahadi A. Equity in global health research in the new millennium: trends in first-authorship for randomized controlled trials among low- and middle-income country researchers 1990-2013. Int J Epidemiol. 2017;45(6):2174-83. https://doi.org/10.1093/ije/dyw313. [ Links ]
31. Tscharntke T, Hochberg ME, Rand TA, Resh VH, Krauss J. Author sequence and credit for contributions in multiauthored publications. PLoS Biol. 2007;5(1):e18. https://doi.org/10.1371/journal.pbio.0050018. [ Links ]
32. Trading Economics. 7 December 2020. Zimbabwe GDP per capita. Available from: https://tradingeconomics.com/zimbabwe/gdp-per-capita. [ Links ]
Received: May 2021
Accepted: October 2021
Published: May 2022
* Corresponding author: cosmas.sibindi@yale.edu
Editor: Dr Marilize Burger, Stellenbosch University, Cape Town, South Africa
Funding: This study was funded in part by the Yale School of Medicine Medical Student Research Fellowship.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.

