










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.21 no.2 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n2a1
TRAUMA AND GENERAL ORTHOPAEDICS
The impact of the COVID-19 lockdown restrictions on orthopaedic trauma admissions in a central academic hospital in Johannesburg
Matthew FosterI,; Jason du PlessisII; Marike Jansen van VuurenI; Maxwell JingoI; Jurek RT PietrzakII
IDivision of Orthopaedic Surgery, University of the Witwatersrand, Johannesburg, South Africa
IICharlotte Maxeke Johannesburg Academic Hospital, Division of Orthopaedic Surgery, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: The novel coronavirus (SARS-CoV-2), commonly known as Covid-19, has caused a global economic and healthcare crisis. Many countries tried to curb the spread of the virus by implementing various lockdown restrictions to reduce transmission. The Republic of South Africa (RSA) implemented an alcohol ban as one of the lockdown restrictions. The objectives were to describe the effect of the lockdown alert levels and alcohol availability on orthopaedic trauma admissions, compared to the preceding two years.
METHODS: A retrospective review of clinical records was conducted. Data included orthopaedic trauma admissions for the five-month period in a facility in Johannesburg from 27 March to 31 August in the years 2018, 2019 and 2020. Lockdown alert levels were categorised according to the Department of Health which included the ban, reintroduction and re-banning of alcohol consumption. Data collected for 2018, 2019 and 2020 included demographics of sex and age, as well as fracture location, open or closed injuries, polytrauma patients and gunshot injuries.
RESULTS: Overall, 672, 621 and 465 patients were admitted in 2018, 2019 and 2020, respectively. There was a decrease of 25% of orthopaedic trauma admissions during the five-month lockdown period in 2020 compared to 2019 (p-value = 0.020) and 30% from 2020 compared to 2018 (p-value = 0.010). In 2020, admissions increased by 112% (n = 82) from alert level 4, when alcohol was banned, to alert level 3 (3a), when alcohol was reintroduced. Admissions decreased by 33% (n = 51) from alert level 3 (3a) to alert level 3 (3b), when alcohol was re-banned. Motor vehicle accidents (MVAs) were the commonest cause of admissions in alert level 3 (3a), accounting for 41% (n = 56). Covid-19 tests were positive in 10% (n = 34) of the 346 tests performed on orthopaedic trauma admissions
CONCLUSION: Our study showed the decrease in orthopaedic trauma admissions due to the Covid-19 lockdown regulations. Furthermore, our study demonstrated the impact of alcohol availability on orthopaedic trauma admissions in a central academic hospital in Johannesburg.
Level of evidence: Level 4.
Keywords: Covid-19, orthopaedic trauma, alcohol
Introduction
The novel coronavirus (SARS-CoV-2), commonly known as Covid-19, was declared a pandemic in March 2020 by the World Health Organization (WHO) and has caused a global health crisis.1 The virus has spread rapidly worldwide spanning 223 countries to date with more than 172 million cases diagnosed and more than 3 711 672 deaths.1 At the time of writing, in the Republic of South Africa (SA), 1 675 013 cases have been diagnosed with 56 711 deaths recorded.2
On 15 March 2020, in response to the escalating number of infections, President Cyril Ramaphosa declared a national state of disaster in SA.3 The SA government made the decision to implement a nationwide lockdown in order to 'flatten the curve' and prepare an under-resourced healthcare system for the inevitable outbreak.2 The lockdown consisted of five alert levels, decreasing in stringency on restrictions of freedom of movement and accessibility to alcohol, with alert level 5 implemented on the 27 March 2020; at the time of writing, we are still under lockdown. A number of unique restrictions were enforced in SA that differed from the rest of the world. One such restriction was the prohibition of selling and distributing alcohol.3-5 Trauma-related injuries claimed 4.9 million lives in 2016, of which 29% were as a result of road traffic accidents.6,7 The leading cause of death between the ages of 5 and 45 years in low- to middle-income countries was injury, which is consistent with SA statistics, as trauma-related orthopaedic injuries currently remain the largest burden on orthopaedic departments across government hospitals.8 Alcohol is a significant contributing factor to trauma-related injuries. The WHO predicts three million deaths worldwide are attributed to alcohol, representing 5.3% of all deaths and is a causal factor in over 200 conditions including injury.9 The devastating socioeconomic and healthcare sector impact caused by the burden of alcohol in SA is well documented, with 62 300 adults dying from alcohol-attributed deaths in 2015.10,11 The tangible financial cost of harmful alcohol use in SA is estimated at R37.9 billion or 1.6% of the GDP.12
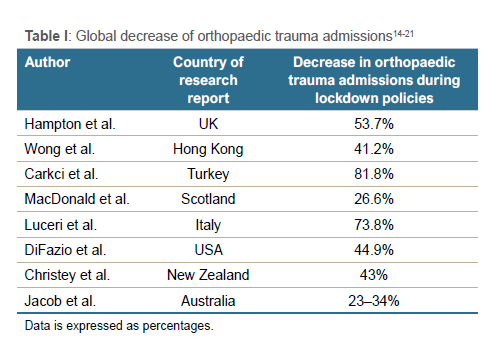
Worldwide, the impact of lockdown levels on orthopaedic trauma admissions has been widely documented (Table I). Waseem et al. reviewed over 665 studies noting a decrease in trauma admission rates ranging from 20.3% up to 84.6%.13 Many studies from Europe, Asia, Australasia and the United States of America have all shown varying degrees of a decrease in orthopaedic trauma admissions (Table I).14-21
The aim of this study is to determine the impact of lockdown restrictions and subsequent alcohol prohibition imposed in response to the Covid-19 pandemic on orthopaedic trauma admissions at a central academic hospital in Johannesburg, compared to the preceding two years.
Methods
Our study was a retrospective review of patients admitted to a central academic hospital in Johannesburg with a trauma orthopaedic injury for the five-month period from 27 March to 31 August in the years 2018, 2019 and 2020, respectively. All research data were collected with approval from both the hospital board and a local research ethics committee.
Our study defined acute orthopaedic trauma injuries as: fractures or dislocations of the upper and lower limbs, traumatic joint injuries, soft tissue injuries to the lower limbs, pelvis injuries and polytrauma patients. These were included in the study population. The legal age for alcohol consumption in South Africa is 18 years; therefore, only patients above 18 years were included in this study. All patients with chronic orthopaedic injuries, musculoskeletal infection, hand fractures distal to the carpus, upper limb tendon injuries, spinal fractures as well as paediatric patients, were excluded as they were attended to by different specialist units.
Admission data were collected from a variety of sources including: trauma admission data sheets collected by the orthopaedic department daily, orthopaedic trauma admission books, clinical audits compiled by the orthopaedic departments six-monthly, as well as morbidity and mortality meeting statistics. All data were collected by the principal investigator (MF), and the results were collated using Microsoft Excel (Microsoft, Seattle, Washington).
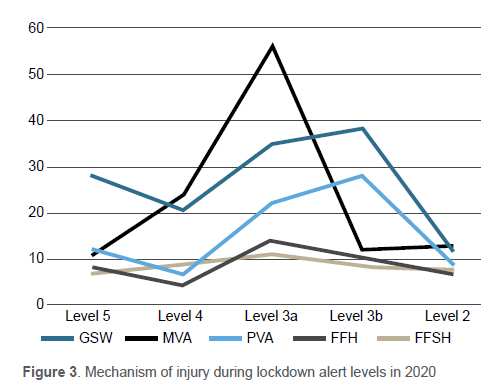
Patients' data were categorised into a variety of groups: demographics, fracture location and morphology, polytrauma, open or closed injuries and mechanism of injury. Demographic data included the patients' sex and age groups, which were divided into those patients younger than 30 years, 31-50 years, 51-70 years and older than 70 years. Fracture location was divided into upper limb, lower limb, pelvis and acetabulum, and polytrauma patients. Upper limb injuries are defined from the clavicle down to carpal bones; lower limb injuries are defined as femoral head to phalanges of the foot; pelvis is defined as injuries to the ischium, ileum and pubis. Hand injuries distal to the carpus and tendon injuries to the upper limb were excluded as they are managed by plastic surgery in our facility. Upper limb and lower limb injuries were further categorised into the location of injury. Pelvis injuries included injuries to the pelvic ring and acetabular fractures. Polytrauma was categorised into more than two long bone fractures, a long bone with a pelvis injury and a long bone with other injury. Open or closed injuries were defined as to whether the associated fracture had an associated breach of skin resulting in an open fracture or a traumatic joint injury. Gunshot wounds (GSWs) were recorded in 2018, 2019, 2020, but other mechanisms of injury (MOI) were only recorded for 2020. These included a fall from standing height (FFSH), fall from height (FFH) (recorded as a fall greater than one step), motor vehicle/motor bike accident (MVA/MBA), pedestrian vehicle accidents (PVA) and not otherwise specified. Covid-19 results were recorded in 2020 and this is defined if the patient tested positive for Covid-19 on a polymerase chain reaction (PCR) nasal swab.
The time periods were categorised according to the months and lockdown alert levels in 2020, as published in the Government Gazette by the Department of Health, and corresponding time periods in 2018 and 2019.3-5 Lockdown levels included alert level 5 which commenced on 27 March 2020 and lasted until 30 April 2020. Restrictions included, but were not limited to, a complete ban of alcohol sales, a curfew, work from home except for essential workers with forced closure of all takeaway outlets and restaurants (Table II). Alert level 4 commenced on 1 May 2020 until 31 May 2020 with a slight ease of restrictions, including allowing for takeaway outlets to operate but maintaining the alcohol prohibition. Lockdown alert level 3 (3a) commenced on 1 June 2020 until 12 July during which time alcohol sales were permitted but subject to specific restrictions. Revised alert level 3 (3b) was from 13 July to 17 August 2020, which did not allow alcohol sales or distribution (Table II).
Data analysis
Categorical variables were described using counts and percentages. Two categorical variables were compared using chi-square test or Fisher's exact test when appropriate. Logistic regression was used to determine associations between binary outcomes (e.g., hospitalisations in 2019 vs 2020 and hospitalisations in alert level 3 (3a) vs 3 (3b) and age, sex, MOI and site. Incidence rates were calculated as the number of events divided by the number of days in the given period. Incidence rates were compared using an exact Poisson test.
Results
Overall, 672 patients were admitted in 2018, 621 admitted in 2019 and 465 in 2020, during the five-month time period from 27 March to 31 August. There was a significant decrease of admissions by 25% between 2019 and 2020 (p-value = 0.020) and 30% between 2018 and 2020 (p-value = 0.010 ) (Figure 1). In alert level 5 lockdown, 81 patients were admitted in 2020 compared to 116 in 2019 and 145 in 2018 for the same time periods. In alert level 4 lockdown, admissions decreased by 42% from 126 in 2019 to 73 patients in 2020 (p-value < 0.001).

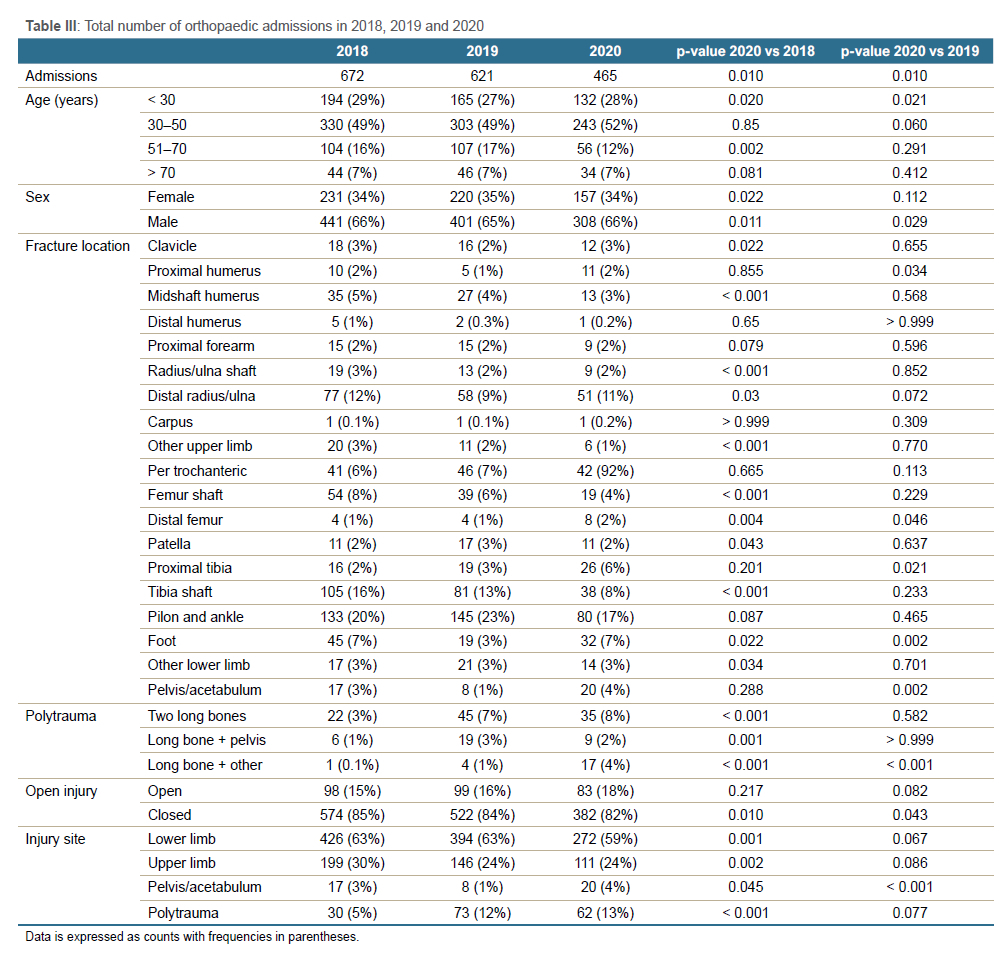
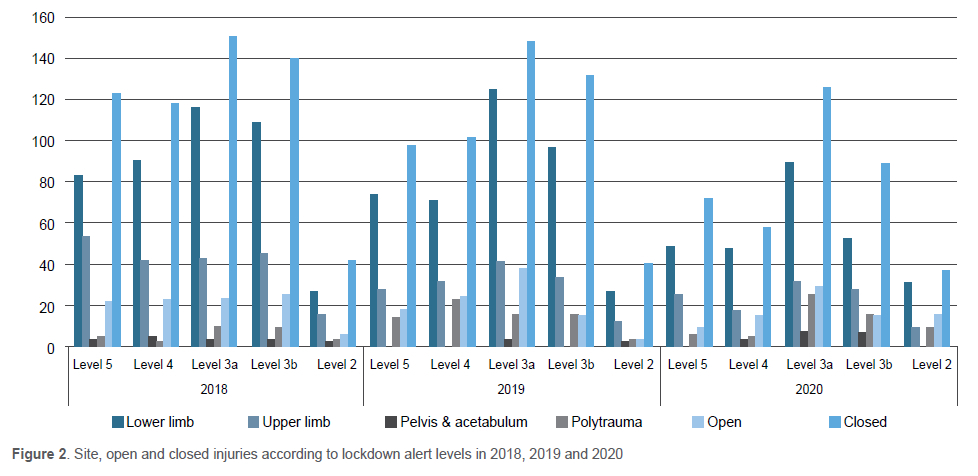
Demographics, fracture morphology and site of all admissions in 2018, 2019 and 2020 are illustrated in Table III. Open fractures accounted for 16% and closed fractures accounted for 84% of the admissions in 2018, whereas in 2020, the proportion of open fractures increased to 18% (p-value = 0.157) and closed fractures decreased to 82%, respectively (p-value = 0.010) (Figure 2).
Admissions increased by 112% (n = 82) in alert level 3 (3a) from alert level 4, followed by a decrease of admissions by 33% (n = 51) in alert level 3 (3b), from level 3 (3a) (p-value = 0.050). The incidence rate (IR) of admissions during alert level 3 (3a) vs 3 (3b) is 1.27 (95% CI: 0.99, 1.65). During alert level 3 (3a), patients < 30 years accounted for 34% of admissions compared to 20% in level 3 (3b). Patients admitted in the 30-50 years age group were 2.16 times more likely than patients < 30 years to be admitted in alert level 3 (3b) compared to alert level 3 (3a) (p-value = 0.020).
From initiation of mandatory testing of all orthopaedic admissions from 19 May 2020, 346 Covid-19 tests were performed on orthopaedic trauma admissions, of which 10% were positive (n = 34) (p-value = 0.001). Of the 34 positive patients, 71% (n = 24) of patients were male (p-value = 0.001). No patients that were Covid-19 positive sustained GSWs and 3% (n = 1) of Covid-19 positive patients sustained an open fracture (p-value < 0.001).
During alert level 5, FFSH were the commonest MOI accounting for 42% (n = 28) of admissions. MVAs were the commonest cause of admissions in alert level 3 (3a), accounting for 41% (n = 56) whereas in alert level 3 (3b), MVAs decreased to 12% (n = 12) (p-value = 0.001) (Figure 3). In alert level 3 (3b), FFSH was again the MOI which attributed to the most admissions at 39% (n = 38). GSWs remained constant through all alert levels of lockdown ranging from 11% (n = 7) of admissions in alert level 5, up to 16% (n = 8) in alert level 2.
Discussion
Our study showed that there was a decrease of 31% and 25% in orthopaedic trauma admissions from the initiation of lockdown compared to the same time periods in 2018 and 2019, respectively. Global reports have shown similar trends; however, many of these were conducted over a short time period, whereas this study has a longer time period to compare data. Hampton et al. showed a decrease of 53.7% of orthopaedic trauma admissions in a United Kingdom (UK) hospital from a two-week pre-lockdown time period to a two-week lockdown time period, and compared these rates to 2019.14 Christey et al. noted a decrease of 43% of admissions in a New Zealand facility and DiFazio et al. showed a 44.9% decrease in a USA facility, for a two-week period pre- and post-lockdown, but without the 2019 comparison.15,20 If we compare the combination of alert levels 4 and 5, referred to as the hard lockdown, to the same time period in 2019, the decrease in admissions was 36% which was more consistent with international data.
SA has a higher burden of trauma relating to interpersonal violence compared to developed nations, where the majority of injuries in developed nations are caused by MVAs or falls, and much less violence.22 A reasonable assumption can be made about the decrease in trauma admissions during lockdown. This was due to policies enforced by government such as: non-essential service employees working from home, a curfew, school closures and a ban on alcohol and cigarettes. This would result in fewer MVAs/PVAs and sporting injuries, and less interpersonal violence and crime. All of the above would be further decreased without the exaggerated harmful effects of intoxication, as alcohol has been proven in SA to have a severe negative impact on society.10 In SA, Moustakis et al. looked at all surgical admissions in the North West in alert level 5, noting a 53% reduction in trauma-related conditions.23 Navsaria et al. noted similar results with a decrease of 53% of all surgical trauma admissions during the hard lockdown in Cape Town.24 Waters et al. specifically looked at the reduction of orthopaedic services from 01 January to 30 April 2020 at Groote Schuur hospital to compare pre-lockdown and lockdown admission rates, noting a decrease of orthopaedic admissions by 40% in April. Our data was consistent with our colleagues in Cape Town, comparing a tertiary hospital in Cape Town to one in Johannesburg; however, our study further looked at the availability and prohibition of alcohol, and the effects thereof.25
Our study showed a significant increase in admissions of 112% from when alcohol was banned in alert level 4, to when it was available in alert level 3 (3a) (Figure 4). The change in admissions between alert levels 4, 3 (3a) and 3 (3b) suggests the influence alcohol has on orthopaedic trauma. Reuter et al. stated that 62 300 South Africans die of alcohol-attributable causes annually and noted a sharp reduction in unnatural related deaths from pre-lockdown of 800-1 000 per week to a rate of 400 per week during lockdown.26 Furthermore, there was a 45% decrease in orthopaedic admissions from two weeks pre-lockdown to the first two weeks of lockdown from the hospital in George where Reuter et al. conducted their research.26 The decrease in admissions due to MVAs from 41% in alert level 3 (3a) to 13% in alert level 3 (3b) identified the significant impact alcohol availability had on MVAs. The association between alcohol and MVAs is consistent with global trends as Papalimperi et al. identified 40.7% of all MVAs over a seven-year period were alcohol related.27 Shneider et al. looked at the burden of disease attributed to alcohol in SA, noting that interpersonal violence and road traffic accidents contributed significantly to disability adjusted life years, clearly illustrating the harmful effects of alcohol on South African society.28

When comparing 2018, 2019 and 2020, males have consistently accounted for almost two-thirds of admissions. Our study showed no difference in this trend during lockdown, which is in keeping with global literature, as males are more prone to trauma-related injuries due to increased risk-taking behaviour and higher levels of interpersonal violence.9,29 When alcohol was allowed in alert level 3 (3a), the age group younger than 30 years accounted for 34% of admissions compared to 16% in alert level 4, when alcohol was banned. This illustrated the impact alcohol has on those younger than 30 years, which was consistent with Caamaño-Isorna et al.'s results, which showed the increase in alcohol-associated injuries in college students in Spain.30
Mandatory Covid-19 testing of all admissions was not present during the early lockdown alert levels so the incidence of 10% was during our peak time period. Pillai et al. concluded that the number of Covid-19 positive patients increased with the easing of lockdown regulations to level 3 in Gauteng, which is consistent with our data.31 In the Covid-19 positive population, demographics, fracture pattern and mechanism of injury were similar to that of Covid-19 negative patients.
Globally, the socioeconomic impact of orthopaedic trauma and alcohol is immense. In the USA, an estimated $53.1 billion is spent annually to treat musculoskeletal injuries, with over a million hospital discharges recorded for fractures.32 Probst et al. identified the socioeconomic effect of alcohol on the South African population, noting that 60% of deaths due to alcohol occur in patients within the low socioeconomic status group.10 Martin et al. calculated that the cost of treating an orthopaedic trauma patient secondary to a GSW in SA was $2 940 (R24 945 at the time), three hours of theatre time with an average stay of 9.75 days.33 The combination of financing healthcare costs, acute and chronic disability of patients, hospital stay and rehabilitation, as well as the time off work, places severe strain on our economy. Alcohol is a major contributing factor, as demonstrated by this report, and the effects of which can be minimised. The WHO has led a global initiative to assist governments in decreasing alcohol-associated harm.34
Covid-19 and the effects of the lockdown policies have demonstrated significant associations between alcohol and orthopaedic trauma admissions. The data collected during this period can be utilised to guide government policies in limiting the harmful effects of alcohol on our society.
Data collection at our institution was not uniform and multiple sources were recorded to obtain data to get a global perspective. Additional limitations included government lockdown bias as a curfew was imposed. This may contribute to diminished orthopaedic trauma admissions in conjunction with no alcohol availability. Moultrie et al. concluded that the complete prohibition of alcohol had a significant reduction in unnatural deaths regardless of the length of the curfew.35 Lastly, with the anticipated reintroduction of alcohol restrictions, people may have stockpiled alcohol, making it available to them during the time of repeat restrictions.
Conclusion
Covid-19 and the lockdown policies enforced by governments worldwide has had a significant effect on decreasing orthopaedic trauma admissions, with SA consistent with global trends. Alcohol availability clearly has a major impact on orthopaedic trauma admissions which, through correct legislation, can be minimised. Our study will hopefully allow government and policy makers to rethink the current legislature around alcohol availability and consider enforcing further regulations limiting alcohol access and the consequence thereof on our healthcare system.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
All research data were collected with approval from both the hospital board and University of the Witwatersrand Human research ethics committee (HREC) (Clearance number: M200877).
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
MF: study conceptualisation, data capture, data analysis, manuscript preparation,
revision and approval of final manuscript
JdP: manuscript revision and approval of final manuscript
MJvV: data collection and approval of final manuscript
MJ: manuscript revision and approval of final manuscript
JRTP: study conceptualisation, manuscript revision and approval of final manuscript
ORCID
Foster Μ https://orcid.org/0000-0001-7709-9529
Du Plessis J https://orcid.org/0000-0002-4617-9742
Jingo M https://orcid.org/0000-0003-2715-5742
Pietrzak JRT http://orcid.org/0000-0001-5694-0016
References
1. WHO. Emergency diseases: Novel Coronavirus 2019 [Internet]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Aaccessed 10 August 2021. [ Links ]
2. Department Of Health. SA Coronavirus [Internet]. Available from: https://sacoronavirus.co.za/. Accessed 10 August 2021. [ Links ]
3. Department of Health. Government Gazette Staatskoerant. Government Gazette Vol. 657 18 March 2020. [ Links ]
4. Department of Health. Government Gazette Staatskoerant. Government Gazette Vol. 608 28 May 2020. [ Links ]
5. Department of Health. Government Gazette Staatskoerant. Government Gazette Vol. 662 17 August 2020. [ Links ]
6. WHO. Global Health Estimates 2016: Deaths by cause, age, sex, by country and by region, 2000-2016. Geneva, World Health Organization; 2018. [ Links ]
7. Allard D, Burch VC. The cost of treating serious abdominal firearm-related injuries in South Africa. S Afr Med J. 2005;95(8):591-94. https://doi.org/10.7196/SAMJ.1783. [ Links ]
8. Lutge EE, Muirhead D. The epidemiology and cost of trauma to the orthopaedic department at a secondary-level hospital. S Afr J Surg. 2005;43(3):74-77. https://doi.org/10.7196/sajs.171. [ Links ]
9. WHO. Global status report on alcohol and health 2018. [ Links ]
10. Probst C, Parry CDH, Wittchen HU, Rehm J. The socioeconomic profile of alcohol-attributable mortality in South Africa: A modelling study. BMC Med. 2018;16(1):97. https://doi.org/10.1186/s12916-018-1080-0. [ Links ]
11. WHO. South Africa: Alcohol consumption, levels and patterns. Elite youth sport policy and management: a comparative analysis. 2016;167-82. https://doi.org/10.4324/9781315713700. [ Links ]
12. Matzopoulos RG, Truen S, Bowman B, Corrigall J. The cost of harmful alcohol use in South Africa. S Afr Med J. 2014;104(2):127-32. https://doi.org/10.7196/SAMJ.7644. [ Links ]
13. Waseem S, Nayar SK, Hull P, et al. The global burden of trauma during the COVID-19 pandemic: A scoping review. J Clin Orthop Trauma. 2021;12(1):200-207. https://doi.org/10.1016/j.jcot.2020.11.005. [ Links ]
14. Hampton M, Clark M, Baxter I, et al. The effects of a UK lockdown on orthopaedic trauma admissions and surgical cases. Bone Jt Open. 2020;1(5):137-43. https://doi.org/10.1302/2633-1462.15.bjo-2020-0028.r1. [ Links ]
15. Christey G, Amey J, Campbell A, Smith A. Variation in volumes and characteristics of trauma patients admitted to a level one trauma centre during national level 4 lockdown for COVID-19 in New Zealand. N Z Med J. 2020;133(1513):81-88. [ Links ]
16. Carkci E, Polat B, Polat A, et al. The effect of the coronavirus 2019 (COVID-19) pandemic on the number and characteristics of orthopedic trauma patients in a tertiary care hospital in Istanbul. Cureus. 2021;2019(1):1-6. https://doi.org/10.7759/cureus.12569. [ Links ]
17. MacDonald DRW, Neilly DW, Davies PSE, et al. Effects of the COVID-19 lockdown on orthopaedic trauma: a multicentre study across Scotland. Bone Jt Open. 2020;1(9):541-48. https://doi.org/10.1302/2633-1462.19.bjo-2020-0114.r1. [ Links ]
18. Wong JSH, Cheung KMC. Impact of COVID-19 on orthopaedic and trauma service: an epidemiological study. J Bone Joint Surg Am. 2020;102(14):e80. https://doi.org/10.2106/JBJS.20.00775. [ Links ]
19. Jacob S, Mwagiru D, Thakur I, et al. Impact of societal restrictions and lockdown on trauma admissions during the COVID-19 pandemic: a single-centre cross-sectional observational study. ANZ J Surg. 2020;90(11):2227-31. https://doi.org/10.1111/ans.16307. [ Links ]
20. DiFazio LT, Curran T, Bilaniuk JW, et al. The impact of the COVID-19 pandemic on hospital admissions for trauma and acute care surgery. Am Surg. 2020;86(8):901-903. https://doi.org/10.1177/0003134820939904. [ Links ]
21. Luceri F, Morelli I, Accetta R, et al. Italy and COVID-19: The changing patient flow in an orthopedic trauma center emergency department. J Orthop Surg. 2020;15(1):1-4. https://doi.org/10.1186/s13018-020-01816-1. [ Links ]
22. Naghavi M, Wang H, Lozano R, et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117-71. https://doi.org/10.1016/S0140-6736(14)61682-2. [ Links ]
23. Moustakis J, Piperidis AA, Ogunrombi AB. The effect of COVID-19 on essential surgical admissions in South Africa: A retrospective observational analysis of admissions before and during lockdown at a tertiary healthcare complex. S Afr Med J. 2020;110(9):910-15. https://doi.org/10.7196/SAMJ.2020.v110i9.15025. [ Links ]
24. Navsaria PH, Nicol AJ, Parry CDH, et al. The effect of lockdown on intentional and nonintentional injury during the COVID-19 pandemic in Cape Town, South Africa: A preliminary report. S Afr Med J. 2020;13183. https://doi.org/10.7196/SAMJ.2021v111i2.15318. [ Links ]
25. Waters R, Dey R, Laubscher M, et al. Drastic reduction of orthopaedic services at an urban tertiary hospital in South Africa during COVID-19: Lessons for the future response to the pandemic. S Afr Med J. 2021;111(3):240-44. [ Links ]
26. Reuter H, Jenkins LS, De Jong M, et al. Prohibiting alcohol sales during the coronavirus disease 2019 pandemic has positive effects on health services in South Africa. Afr J Prim Health Care Fam Med. 2020;12(1):1-4. https://doi.org/10.4102/phcfm.v12i1.2528. [ Links ]
27. Papalimperi A, Athanaselis S, Mina A, et al. Incidence of fatalities of road traffic accidents associated with alcohol consumption and the use of psychoactive drugs: A 7-year survey (2011-2017). Exp Ther Med. 2019;18(3):2299-306. https://doi.org/10.3892/etm.2019.7787. [ Links ]
28. Schneider M, Bradshaw D, Norman R, et al. Estimating the burden of disease attributable to alcohol use in South Africa in 2000. S Afr Med J. 2007;97(8):674-81. https://doi.org/10.7196/SAMJ.661. [ Links ]
29. Gomez D, Haas B, De Mestral C, et al. Gender-associated differences in access to trauma center care: A population-based analysis. Surgery. 2012;152(2):179-85. https://doi.org/10.1016/j.surg.2012.04.006. [ Links ]
30. Caamaño-Isorna F, Moure-Rodríguez L, Doallo S, et al. Heavy episodic drinking and alcohol-related injuries: An open cohort study among college students. Accid Anal Prev. 2017;100:23-29. https://doi.org/10.1016/j.aap.2016.12.012. [ Links ]
31. Pillai J, Motloba P, Motaung KSC, et al. The effect of lockdown regulations on SARS-CoV-2 infectivity in Gauteng Province, South Africa. S Afr Med J. 2020;110(11):1119-23. https://doi.org/10.7196/SAMJ.2020.v110i11.14828. [ Links ]
32. Bone and Joint Initiative USA. By the numbers. Musculoskeletal Conditions. Diseases, disorders and injuries relating to bones, joints and muscles. Available from: www.boneandjointburden.org. Accessed 8 June 2021. [ Links ]
33. Martin C, Thiart G, McCollum G, et al. The burden of gunshot injuries on orthopaedic healthcare resourcesin south Africa. S Afr Med J. 2017;107(7):626-30. https://doi.org/10.7196/SAMJ.2017.v107i7.12257. [ Links ]
34. WHO. SAFER- a world free from preventable disease. Available from: https://www.who.int/initiatives/SAFER. [ Links ]
35. Moultrie TA, Dorrington RE, Laubscher R, et al. Unnatural deaths, alcohol bans, and curfews: Evidence from a quasi-natural experiment during COVID-19. S Afr Med J. 2021;111(9):834-37. https://doi.org/10.7196/SAMJ.2021.v111i9.15813. [ Links ]
Received: August 2021
Accepted: November 2021
Published: May 2022
* Corresponding author:matthew@drfoster.co.za
Editor: Prof. Nando Ferreira, Stellenbosch University, Cape Town, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}
{kind=link}
{kind=link}