










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.21 no.1 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n1a6
HAND SURGERY
Patient satisfaction following wide awake local anaesthetic no tourniquet hand surgery
Michael de Buys*; Mluleki Tsama; Abdirashid A Aden
Department of Orthopaedic Surgery, Helen Joseph Hospital, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Wide awake local anaesthetic no tourniquet (WALANT) hand surgery is a rapidly growing technique for hand surgery whereby a lignocaine/adrenaline/bicarbonate mixture is injected into the hand or fingers where the procedure is to be carried out
METHODS: This was a retrospective study with prospective recall analysing satisfaction of patients who underwent WALANT hand surgery at our academic hospital in the first year of its inception. Data collection included a questionnaire to analyse demographics, comparison to dental procedures, subjective and objective experience of the procedure, overall experience, expectations, pain and surgical outcome
RESULTS: We included 80 procedures in 67 patients; 87% would prefer WALANT in the future, and 87% would recommend WALANT to friends or family. For 79% of patients (who had dental procedures before), the pain was less or the same as a dental procedure, and 70% of patients said the experience was better than expected. Average pain scores were 3.89/10 during local anaesthetic injection, 1.25/10 during the procedure and 5.20/10 postoperatively; with postoperative pain starting at an average of nine hours. Eighty-five per cent of conditions were cured at follow-up and no cases of digital ischaemia or infection were noted
CONCLUSION: Our study suggests WALANT hand surgery is a safe, effective and satisfactory method of performing hand surgery in the South African context
Level of evidence: Level 4
Keywords: WALANT, hand surgery, local anaesthetic, carpal tunnel, de Quervain's, ganglion, patient satisfaction
Introduction
Wide awake local anaesthetic no tourniquet (WALANT) hand surgery, a concept developed in 2007 by Dr Lalonde, is gaining popularity worldwide.1,2 It involves surgery being carried out on a non-sedated patient without the need for a tourniquet with simply a local injection.3,4 A cocktail of 1% lignocaine/adrenaline 1:100 000 and 8.4% sodium bicarbonate in a 10:1 ratio is injected into the area of surgery in a tumescent-type manner. The lignocaine provides anaesthesia and adrenaline causes vasoconstriction and therefore a bloodless field.2,4,5 The sodium bicarbonate buffers the acidic nature of the lignocaine and in doing so optimises the speed of onset.2
Traditionally, anaesthesia for hand surgery would either be general anaesthesia or some form of regional anaesthesia.6 The term 'local anaesthetic' previously implied local anaesthetic given together with some form of sedation, largely to overcome the discomfort of the applied tourniquet.1 The use of the tourniquet traditionally was vital to provide a bloodless field; however, the pain is severe if not combined with general or regional anaesthesia.7 In addition to discomfort, the tourniquet can cause nerve damage with subsequent neurological deficits, muscular damage and is time-limited to a maximum of two hours.7,8 A comparison between WALANT surgery and a local anaesthesia with tourniquet technique showed a difference in comfort, with WALANT being better tolerated.7
Medical school teaches the mantra that local anaesthetic cannot be injected into extremities including fingers, toes, nose and the penis due to a fear of digital ischaemia.5 The idea is based around the belief that these are end artery type systems and the vasospasm from adrenaline is therefore likely to be catastrophic.9 Numerous literature reviews have been conducted looking at this concept and have concluded that there has not been a single literature report of digital ischaemia where adrenaline and lignocaine have been used.9
The benefits of WALANT hand surgery are numerous and include benefits for the patient, the doctor and the hospital.4 WALANT hand surgery requires no general anaesthesia, sedatives or opiates, which ameliorates the possibility of deleterious side effects of these medications and provides a generally safer procedure.4 Davison et al. showed that only 3% of patients undergoing WALANT hand surgery required preoperative blood tests, electrocardiogram and/or chest radiograph versus 48% of patients who were sedated.10 Patients with medical comorbidities are typically not excluded from the procedure and chronic medication, including anticoagulants, does not need to be stopped.11 The procedure does not require intravenous (IV) lines, or intraoperative or postoperative monitoring, and the patient does not need hospitalisation.4,12
The patient can be educated on postoperative management protocols and likely expectations during the procedure.4 Intraoperative visualisation by the patient of the surgical site allows the patient to visualise the repair, which aids understanding of the function allowed during rehabilitation.4 Real-time and dynamic testing of the repair can be done by the surgeon prior to the skin being sutured and is exceptionally helpful for assessing tendon repair tension, glide of tendons in the sheath as well as the rotational component following metacarpal and phalanx fracture repair.1,4
Numerous studies have been done demonstrating the cost-benefit of WALANT hand surgery. A study in Canada and similarly in the United States of America (USA) showed that carpal tunnel release performed in a hospital was four times more expensive than carpal tunnel release done in a clinic.1 In the United Kingdom (UK), a study comparing the cost of adopting WALANT versus normal anaesthetic showed a saving of $3.2 million in 1 000 patients.1 Bismil et al. showed a cost reduction of 50-75% when adopting the WALANT technique for amenable hand surgery cases.13 Rhee et al. demonstrated an 80% and 75% cost saving for carpal tunnel and A1 pulley release when done in their clinic via WALANT versus in their main theatres under general anaesthesia, respectively.12
Teo et al. conducted a study looking at patient satisfaction in the first 100 consecutive patients who underwent WALANT hand surgery at their institution and concluded that 86% of patients would prefer to be awake again and 90% would recommend it to a friend.2 Van Demark et al. looked at patient satisfaction in WALANT hand surgery done in an office procedure room, with results showing 99% of patients would do WALANT in the office again and 99% would recommend it to a friend.1,14 Davison et al. showed that 93% of patients undergoing carpal tunnel release by the WALANT technique would choose it again.10 Rhee et al. conducted a study of 100 patients undergoing a cohort of procedures under WALANT and showed 94% of their followed-up patients would choose WALANT again. Postoperative pain felt following WALANT hand surgery has been shown to be less than that of a dental procedure in 71% of patients.1,12
The South African population can be viewed as being significantly different from those studied in developed European countries, the USA and Canada; this includes cultural and historical factors, values and belief systems. Furthermore, there is significant diversity in the population of patients seen in a South African hospital when looking at parameters including level of highest education, prior contact with the medical sector (surgically or medically) and expectations when seeking medical assistance.
This study was undertaken to assess the satisfaction of patients who underwent WALANT hand surgery at Helen Joseph Hospital, a state hospital, to assess the eligibility of this method in the South African sector.
Methods
We performed a retrospective cross-sectional study with prospective recall of patients who underwent WALANT hand surgery from 1 April 2017 to 31 March 2018, after obtaining hospital permission and ethics clearance.
A questionnaire adapted from the work of Teo et al. was created (with permission) assessing patient demographics, medical history, experience of the surgery and outcome.2 Pain at each part of the procedure was assessed using the Wong-Baker FACES chart (with permission, ©1983 Wong-Baker FACES Foundation). The Wong-Baker FACES chart was selected as the assessment method for pain in an attempt to ensure pain could be evaluated by each patient irrespective of any cultural, language or educational differences.
We included all adult patients (18 years and older) who had WALANT hand surgery performed during the specified time frame, were contactable by their phone number recorded in hospital records and who gave consent to being included in the study.
Descriptive analysis was done looking at patients' demographics and medical history. The future anaesthetic choice of patients (WALANT versus general anaesthesia), comparison of experience versus expectation, likelihood to recommend WALANT to friends/ family and comparison to previous dental procedure(s) were analysed using descriptive parameters.
Level of pain felt was assessed at each part of the WALANT procedure (local anaesthetic injection/surgery/postoperatively). Patients were questioned as to how much pain they would tolerate to have their condition cured and this was defined as 'acceptable level of pain'.
At follow-up, patients were assessed for evidence of sepsis or ischaemia, and an examination was performed to elucidate whether the condition for which surgery was done had been cured.
Results
During the defined study period, 134 procedures were performed in the theatre allocated for WALANT surgery. Six procedures were excluded as they were operations of the foot and one excluded as the patient was less than 18 years of age, leaving 127 procedures eligible for the study. Seventeen patients had two procedures done, leaving 110 different patients eligible to be included in the study.
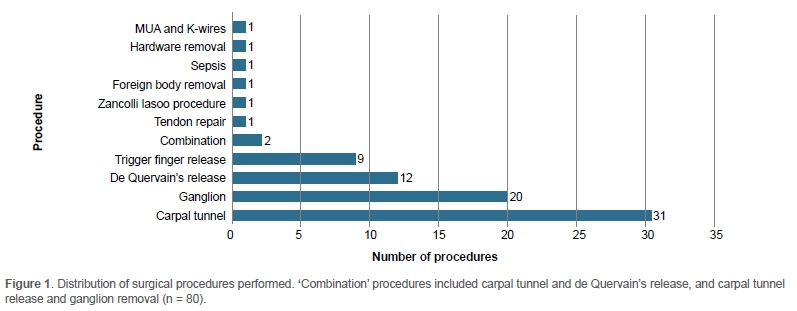
The final number of participants in the study was 67/110 (61%) with a total of 80/127 (63%) different procedures, with Figure 1 showing the procedures included. The patients not included were not contactable via the contact details in hospital records.
Of the 67 patients, 51 patients were female and 16 were male. Patient ages ranged from 18 to 90 years with a mean age of 44 years. The distribution of race, age and levels of education are shown in Figure 2. The percentage of patients whose condition was cured when analysing the four most common procedures is given in Table I.


In this study, 60% of the procedures were done on the patient's right hand and 40% on the left side. In addition, 57% of the procedures were done on the patient's dominant hand.
Overall, 58 (87%) patients would choose WALANT and nine (13%) would prefer to be asleep if they were to have another operation of the hand in the future. Furthermore, 47 (70%) patients said it was better than expected, 18 (27%) said it was the same as they expected and two (3%) said it was worse than expected.
In addition, 70% of patients would definitely recommend WALANT to a friend/family, whereas 16% would probably recommend it, 5% would definitely not recommend it, 8% would probably not recommend it and 2% were unsure if they would (Figure 3).

In total, 58 (88%) patients had had a previous dental procedure, while nine (13%) patients had not. Of the patients who had, 34 (59%) said the WALANT procedure was less painful, 12 (21%) said it was the same and 12 (21%) said it was more painful than the dental procedure.
The average pain measured using the visual analogue scale (VAS) during local anaesthetic (LA) injection was 3.89, during the procedure 1.25, and following the procedure it was 5.20. The average time to maximal amount of pain postoperatively was approximately nine hours. Sixty-five per cent of the patients' procedures had a pain score of 0/10 during the surgery, with 93% of the procedures having a pain score less than or equal to 5/10 during the procedure. Patients were questioned as to what the maximal amount of pain would be to have their condition cured. This was termed 'acceptable level' of pain and on average was 5.60/10.
None of the cases required conversion to regional or general anaesthesia, there was no case of sepsis on follow-up, and not a single case of digital ischaemia was noted.
Discussion
To date, there is no published data looking at the satisfaction, effectiveness and safety of WALANT hand surgery in the South African context.
This study showed that 87% of the patients interviewed would prefer WALANT if they were to have another hand operation in the future. This is similar to the result of 86% seen by Teo et al. and suggests a subjectively high level of satisfaction with the WALANT hand surgery technique.2
Patients were asked the likelihood of their recommending WALANT as the anaesthetic method for hand surgery to their friends or family. This was to analyse the objective assessment of the WALANT hand surgery procedure by the patient and their understanding of it in terms of safety, efficacy, convenience and overall experience. This is in addition to the subjective view noted when asking what anaesthesia the patient would prefer for themselves in the future. We noted that 87% of participants suggested they were likely to recommend WALANT to their family and friends, very close to that of 90% published by Teo et al.2
The preoperative surgical expectations of patients may be governed by multiple factors. These potentially include the preoperative counselling of the patient by the surgical team as well as other patient-specific factors including past surgical experiences, personality traits and understanding of the intricacies of the proposed procedure. This study comprised a heterogenous group of patients as illustrated by the diversity of patients' age, race, sex, level of education and prior medical contact in this study. Furthermore, with the large patient load compared to the number of doctors in the South African setting, insufficient explaining and counselling of patients about procedures may occur, which could potentially negatively affect the patient experience. With these concepts in mind, 70% of patients indicated their experience was better than expected, which is higher than the result seen by Teo et al. (59%).2 Only 3% of patients said it was worse than what they were expecting which is less than half the 7.7% noted by Teo et al.2 This result suggests a positive response to the WALANT hand surgery technique and is a critical statistic that can be included in preoperative counselling sessions with patients as well as for discussions with practitioners reluctant to start implementing the WALANT technique.
The literature states that WALANT hand surgery can be likened to a dental procedure, and this can be used as a method to inform patients on what to expect. In our heterogenous study population, 88% of patients did have a previous dental procedure to which they could relate. Of these patients, 79% said the procedure was the same or less painful than their previous dental procedure, suggesting that this is a reliable predictor of what the patient can expect and an effective statistic to use when counselling the patient.
In keeping with the literature, there was not a single incidence of digital ischaemia noted in the study and none of the cases required phentolamine rescue. This is a critical finding suggesting that WALANT is a safe method of anaesthesia for hand surgery and further adds to the literature base stating such.4,7-9 Further, despite no prophylactic antibiotics being administered and minor field sterility used in this study, there were no instances of infection noted postoperatively, also in keeping with published literature.1
When analysing the amount of pain experienced by the patients in this study, we demonstrated on average the highest pain scores occurred postoperatively (average score 5.20). This is in keeping with Rawal et al. who showed that 37% of hand patients suffered from moderate to severe pain following their procedure.16 This finding that the postoperative pain is more than the local anaesthetic injection contradicts the statement made by Lee and is an important finding.6 The postoperative pain, however, cannot be entirely attributed to the WALANT technique but rather it is related to the surgery itself. This pain was on average maximal at approximately nine hours following the procedure. A further investigation is required to determine the most effective management protocol for postoperative surgical pain. Patient education to begin regular analgesia immediately following the procedure prior to the block wearing off would potentially assist in managing pain. Other mechanical methods, including splints (short term), may be useful adjuncts immediately following surgery and should be kept in mind.
The average pain noted during local anaesthetic injection in this study of 3.89/10 is slightly lower than the value described by Mohd Rashid et al. of 4.66/10.17 When assessing the intraoperative levels of pain, 66% of patients felt no pain during the procedure, which is similar to that of 68% by Teo et al.2 Patients were asked to identify the maximal amount of pain they would say is acceptable for the procedure to have their condition cured; this was noted on average to be 5.60/10. In this study population, 93% felt pain less than or equal to 5/10, compared to 88% by Teo et al., which is less than the average acceptable level of pain.
In this study, WALANT hand surgery showed a high rate of cure (85%) of the condition for which surgical treatment was sought by the patient. We had a diverse group of procedures done but analysing the four most common procedures in our study suggests the cure rates are in keeping with published values. Carpal tunnel release is stated to have a success rate of 75-90%, with our study demonstrating an 80% cure rate.18 Literature suggests a success rate following de Quervain's tenosynovitis release and trigger finger release of 91-100% and 90-100%, respectively; this study population demonstrated success in 100% of the de Quervain's tenosynovitis and 89% of the trigger finger releases, respectively.19,20 Ganglions have been described as having variable recurrence rates with values stated between 1% and 49%.21 In our study a recurrence rate of 24% was observed, which falls within those margins.
No cost analysis was done due to the complexity of such multifactorial calculations; however, a large cost saving can be inferred based on the data presented. Fifty-nine per cent of our patients had known comorbidities and required no work-up whatsoever prior to surgery, and none of the patients required admission pre- or postoperatively, thus further reducing hospital expenses. The number of staff members in theatre was reduced to a surgeon and a scrub nurse compared to the usual complement noted during a general anaesthesia case. In addition, minor field sterility was used, limiting the amount of waste and dirty linen created.
Despite being an innovative and informative study, several limitations exist and need to be addressed. This study relied on a retrospective recall of patients which may affect the results noted depending on the duration of time between surgery and the questionnaire. However, this concept was studied by Teo et al. and the authors found no statistical difference in the results between patients who were classified into the early group (questionnaire completed 3-12 months postoperatively) and the late group (questionnaire completed 13-22 months postoperatively).2 All our patients had the questionnaire completed before the 22 months postoperative time period.
This study noted a skewed enrolment of patients who underwent elective surgery versus those who underwent surgery for emergency injuries. An explanation for this observation is that elective surgery patients had reliable contact details which were used to contact them for their procedure and therefore had a higher likelihood of successful contact when the study was being conducted. Patients who presented following an emergency admission were often noted not to have included a contact number in their file or the contact number was incorrect or suspected to have changed. To be enrolled in this study, patients had to have reliable contact details as they needed to visit the hospital to provide consent and complete the questionnaire, and the combination of these two factors potentially limited the number of enrolled patients.
Further studies looking at the possibility of using WALANT hand surgery in rural areas of the country may prevent the referral of patients to higher level of care facilities. In addition, looking at performing WALANT hand surgery in an adapted out-patient department and potentially operating on the index presentation of the patient would provide critical data and potentially improve the efficiency of the service provided significantly. Finally, patient satisfaction in traumatic/bony procedures needs to be assessed and results compared to soft tissue only procedures to ensure our patients are reliably pleased with our method of anaesthesia; our study strongly favoured soft tissue procedures.
Conclusion
Based on the results obtained from this study, WALANT appears to be a safe, effective and well-tolerated anaesthetic method for hand surgery in the South African context with a high level of patient satisfaction. It has the potential to greatly improve all facets of hand surgery for the patient, the surgeon and the hospital.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
Prior to commencement of the study, hospital permission obtained from the CEO of Helen Joseph Hospital and ethics clearance from the University of the Witwatersrand's Human Research Ethics Committee (Medical), ethics clearance certificate number M180450.
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed written consent was obtained from all patients for being included in the study.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
MdB: study conceptualisation, study design, data capture, data analysis, first draft and subsequent draft preparation, manuscript preparation MT: study design, manuscript revision
AAA: study conceptualisation, study design, data analysis, draft and manuscript revision
ORCID
De Buys M https://orcid.org/0000-0002-8780-433X
Tsama M https://orcid.org/0000-0001-6681-0848
Aden AA https://orcid.org/0000-0001-5589-2972
References
1. Van Demark RE, Becker HA, Anderson MC, Smith VJS. Wide-awake anesthesia in the in-office procedure room: lessons learned. Hand. 2018;13(4):481-85. https://doi.org/10.1177/1558944717715120. [ Links ]
2. Teo I, Lam W, Muthayya P, et al. Patients' perspective of wide-awake hand surgery - 100 consecutive cases. J Hand Surg Eur Vol. 2013;38(9):992-99. https://doi.org/10.1177/1753193412475241. [ Links ]
3. Lalonde D. Wide awake local anaesthesia no tourniquet technique (WALANT). BMC Proc. 2015;9(Suppl 3):A81. [ Links ]
4. Lalonde DH. Conceptual origins, current practice, and views of wide awake hand surgery. J Hand Surg Eur Vol. 2017;42(9):886-95. https://doi.org/10.1177/1753193417728427. [ Links ]
5. Pires Neto PJ, Moreira L de A, Las Casas PP de. Is it safe to use local anesthesia with adrenaline in hand surgery? WALANT technique. Rev Bras Ortop (English Ed [Internet]. 2017;52(4):383-89. https://doi.org/10.1016/j.rboe.2017.05.006. [ Links ]
6. Lee D-C. Wide awake hand surgery. Arch Plast Surg. 2017;44(4):348. https://doi.org/10.5999/aps.2017.44.4.348. [ Links ]
7. Gunasagaran J, Sean ES, Shivdas S, et al. Perceived comfort during minor hand surgeries with wide awake local anaesthesia no tourniquet (WALANT) versus local anaesthesia (LA)/tourniquet. J Orthop Surg [Internet]. 2017;25(3):230949901773949. https://doi.org/10.1177%2F2309499017739499. [ Links ]
8. Ayhan E, Özdemir E, Gumusoglu E, et al. The rise of wide awake hand surgery -Contribution from Turkey. Hand Microsurg. 2018;7(3):1. [ Links ]
9. Thomson CJ, Lalonde DH, Denkler KA, Feicht AJ. A critical look at the evidence for and against elective epinephrine use in the finger. Plast Reconstr Surg. 2007;119(1):260-66. https://doi.org/10.1097/01.prs.0000237039.71227.11. [ Links ]
10. Davison PG, Cobb T, Lalonde DH. The patient's perspective on carpal tunnel surgery related to the type of anesthesia: A prospective cohort study. Hand. 2013;8(1):47-53. https://doi.org/10.1007/s11552-012-9474-5. [ Links ]
11. Sasor SE, Evans TA, Cook JA, et al. Assessing the necessity of stopping antithrombotic agents before wide-awake hand surgery. JAMA Surg. 2018;153(3):284-85. https://doi.org/10.1001/jamasurg.2017.3927. [ Links ]
12. Rhee PC, Fischer MM, Rhee LS, McMillan H, Johnson AE. Cost savings and patient experiences of a clinic-based, wide-awake hand surgery program at a military medical center: a critical analysis of the first 100 procedures. J Hand Surg Am. 2017;42(3):e139-47. https://doi.org/10.1016/jjhsa.2016.11.019. [ Links ]
13. Bismil M, Bismil Q, Harding D, et al. Transition to total one-stop wideawake hand surgery service-audit: a retrospective review. JRSM Short Rep. 2012;3(4):1-9. https://doi.org/10.1258/shorts.2012.012019. [ Links ]
14. Steiner MM, Calandruccio JH. Use of wide-awake local anesthesia no tourniquet in hand and wrist surgery. Orthop Clin North Am. 2018;49(1):63-68. https://doi.org/10.1016/j.ocl.2017.08.008. [ Links ]
15. Haibach-Beach P, Reid G, Collier DH. Motor learning and development. 2nd ed. Human Kinetics; 2018. [ Links ]
16. Rawal N, Hylander J, Nydahl PA, Olofsson I, Gupta A. Survey of postoperative analgesia following ambulatory surgery. Acta Anaesthesiol Scand. 1997;41(8):1017-22. https://doi.org/10.1111/j.1399-6576.1997.tb04829.x. [ Links ]
17. Mohd Rashid MZ, Sapuan J, Abdullah S. A randomized controlled trial of trigger finger release under digital anesthesia with (WALANT) and without adrenaline. J Orthop Surg. 2019;27(1):2309499019833002. https://doi.org/10.1177/2309499019833002. [ Links ]
18. Louie D, Earp B, Blazar P. Long-term outcomes of carpal tunnel release: A critical review of the literature. Hand. 2012;7(3):242-46. https://doi.org/10.1007/s11552-012-9429-x. [ Links ]
19. Scheller A, Schuh R, Hönle W, Schuh A. Long-term results of surgical release of de Quervain's stenosing tenosynovitis. Int Orthop. 2009;33(5):1301-303. https://doi.org/10.1007/s00264-008-0667-z. [ Links ]
20. Ta KT, Eidelman D, Thomson JG. Patient satisfaction and outcomes of surgery for de Quervain's tenosynovitis. J Hand Surg Am. 1999;24(5):1071-77. https://doi.org/10.1053/jhsu.1999.1071. [ Links ]
21. Lidder S. Surgical excision of wrist ganglia; literature review and nine-year retrospective study of recurrence and patient satisfaction. Orthop Rev (Pavia). 2009;1(1):e5. https://doi.org/10.4081/or.2009.e5. [ Links ]
Received: May 2020
Accepted: April 2021
Published: March 2022
* Corresponding author: debuysm@gmail.com
Editor: Dr Duncan McGuire, University of Cape Town, Cape Town, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}