










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.21 no.1 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n1a5
PAEDIATRIC ORTHOPAEDICS
The Fassier technique for correction of proximal femoral deformity in children with osteogenesis imperfecta
Sandile M MwelaseI, *; Pieter H MaréII; David M ThompsonI; Leonard C MaraisIII
IDepartment of Orthopaedic Surgery, Grey's Hospital, School of Clinical Medicine, University of KwaZulu-Natal, South Africa
IIClinical Unit Paediatric Orthopaedics, Department of Orthopaedic Surgery, Grey's Hospital, School of Clinical Medicine, University of KwaZulu-Natal, South Africa
IIIDepartment of Orthopaedic Surgery, School of Clinical Medicine, University of KwaZulu-Natal, South Africa
ABSTRACT
BACKGROUND: Children with osteogenesis imperfecta frequently present with coxa vara. Skeletal fragility, severe deformity and limited fixation options make this a challenging condition to correct surgically. Our study aimed to determine the efficacy of the Fassier technique to correct coxa vara and determine the complication rate
METHODS: We retrospectively reviewed the records of a cohort of eight children (four females, 12 hips) with osteogenesis imperfecta (6/8 Sillence type III, 2/8 type IV) who had surgical treatment with the Fassier technique for proximal femoral deformity between 2014 and 2020
RESULTS: The mean age at operation was 5.8 years (range 2-10). The mean neck-shaft angle (NSA) was corrected from 96.8° preoperatively to 137° postoperatively. At a mean follow-up of 38.6 months, the mean NSA was maintained at 133°, and 83% (10/12) of hips had an NSA that remained greater than 120°. There was a 42% (5/12) complication rate: three Fassier-Duval rods failed to expand after distal epiphyseal fixation was lost during growth; one Rush rod migrated through the lateral proximal femur cortex with recurrent coxa vara; and one Rush rod migrated proximally and required rod revision
CONCLUSION: The Fassier technique effectively corrected coxa vara in children with moderate and progressively deforming osteogenesis imperfecta. The deformity correction was maintained in the short term. The complication rate was high, but mainly related to the failed expansion of the Fassier-Duval rods. Further studies are required to determine the long-term outcome of this technique
Level of evidence: Level 4
Keywords: osteogenesis imperfecta, coxa vara, Fassier-Duval, neck-shaft angle, deformity
Our study aimed to evaluate the Fassier technique of correction of the proximal femoral deformity in OI. Our primary objectives were to determine the magnitude of correction as measured by the NSA, and to determine whether this correction was maintained at the latest follow-up. The secondary objective was to determine the short-term complication rate of this technique.
Patients and methods
Following ethical approval from our institution's research ethics committee, we used non-probability purposive sampling to identify all patients treated with the Fassier technique at our tertiary paediatric orthopaedic unit between 2014 and 2020. All OI patients younger than 18 years who were treated for proximal femoral deformity with or without visible stress fractures with expandable Fassier-Duval rods or Rush rods and K-wire fixation utilising the Fassier technique as the primary procedure were included.
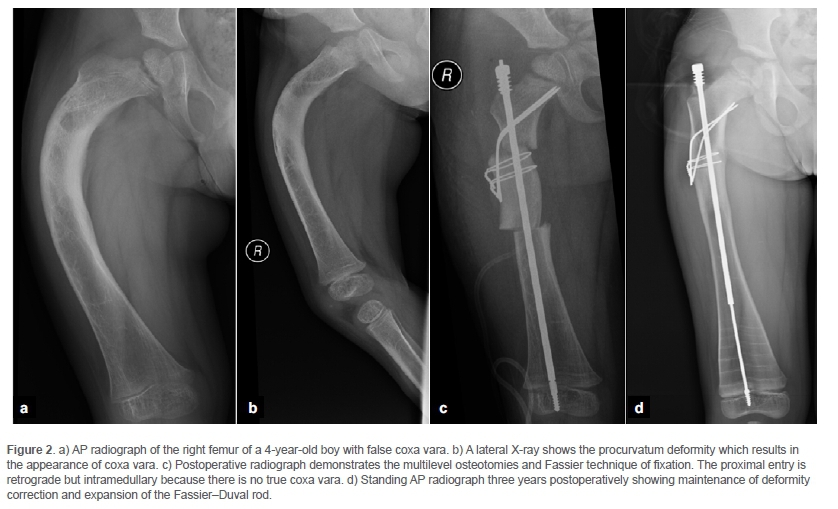
The study cohort included eight children (four females, 12 hips) with a proximal femoral deformity corrected with the Fassier technique after one hip was excluded from analysis as surgery was done to revise a failed valgus osteotomy and plating of the right hip. The plating resulted in severe translation and distortion of the proximal femur anatomy, and we were unable to adequately correct this deformity or achieve stable fixation with the Fassier technique. Bilateral deformity correction (staged in three children) was required in four children. Eight hips were diagnosed as CV with an NSA of less than 110° (Figure 1).1,2 Two hips had a decreased NSA (113° and 114°, respectively) that did not meet the diagnostic criteria of CV. The remaining two hips were diagnosed as 'false coxa vara' with an NSA measured as 124° and 130°, respectively.2 False CV was diagnosed when a severe procurvatum deformity was apparent on the lateral femur X-ray that resulted in the appearance of CV on the AP X-ray (Figure 2).

Fassier et al. previously described the surgical technique.2 Our indication for the procedure was any child with OI and proximal femoral deformity that required correction through a subtrochanteric osteotomy. The lateral approach was used to expose the proximal femur. Two K-wires were inserted along the femoral neck axis from the posterolateral proximal femur to anteromedial in the femoral head, and from the anterolateral proximal femur to posteromedial in the femoral head. We used these wires to control the proximal fragment after a transverse proximal femoral osteotomy was performed just below the level of the lesser trochanter. In severe true CV (Figure 1), the proximal entry was established in a retrograde direction from the lateral cortex. In false CV, the retrograde entry was made from within the intramedullary canal (Figure 2). The proximal tip of the male component of the Fassier-Duval (FD) rod was passed in a retrograde direction through the proximal fragment exiting at the piriformis fossa and through a separate more proximal skin incision. The male component was then advanced, and the threaded distal end seated into the distal femur epiphysis. The female component of the FD rod was then inserted antegrade over the male component and the proximal threaded portion secured in the proximal femur. The K-wires were then cut and bent and secured to the proximal femoral shaft with two cerclage wires. All the children with OI received the intravenous bisphosphonate zoledronic acid (0.05 mg/kg zoledronic acid in 50 ml normal saline over 30 minutes) at six-monthly intervals for metabolic control of the disorder.7
Clinical data was extracted from our paediatric orthopaedic database and combined with the radiological data stored in our picture archiving and communication system (PACS). Data points included age at surgery, sex, body mass index percentile for age and sex (BMI percentile), mobility status, preoperative neck-shaft angle (NSA), immediate postoperative NSA, NSA at latest follow-up, delta NSA (the change between the immediate postoperative NSA measurement and the NSA measured at latest follow-up), and complications.
The magnitude of NSA correction and the extent to which this correction was maintained during follow-up were the primary outcome variables. The incidence of complications was the secondary outcome variable. Possible complications were recurrent deformity, loss of epiphyseal fixation with failed rod expansion (FD rods), transcortical rod migration, periprosthetic fracture, rod breakage, infection, growth arrest and hip avascular necrosis.
Statistical analysis
Statistical analysis was performed using jamovi version 1.2.18.0 open-source software.8 Continuous variables were reported as mean (standard deviation [SD], range) or median (interquartile range [IQR], range), and categorical variables as number and percentages. The Shapiro-Wilk test was used to analyse the distribution of data. Normally distributed data were compared using the unpaired Student's t-test, whereas the Mann-Whitney test was used for non-parametric data. Categorical data were analysed using the chi-squared test unless the expected value in any cell was below 5 when Fisher's exact test was used. Correlation between normally distributed continuous variables was tested with Pearson's correlation coefficient. All tests were two-sided, and the level of significance was set at p < 0.05. Binomial logistic regression was used to determine the odds ratio (ORs) and 95% confidence interval (95% CI) of the primary outcome measure.
Results
The descriptive data are summarised in Table I. The mean age of the patients at operation was 5.8 years (SD 2.4 years, range 2-10). Of the eight children, two had Sillence type IV OI, and six had type III OI. Obesity (BMI > 95th percentile for sex and age) was present in two children (three hips). Intramedullary fixation was achieved with Rush rods (RR) in three, and FD expandable rods in nine hips.
The mean NSA preoperatively was 97° (SD 23°, range 56-130) and mean NSA postoperatively was 137° (SD 5°, range 128-148). The mean follow-up was 39 months (SD 24 months, range 1-72). At the latest follow-up, the mean NSA was 133° (SD 12.4, range 107-153). The mean delta NSA was -6° (SD 8°, range +3 to -21). The NSA remained corrected to > 120° in 83% (10/12) of hips at latest follow-up.
There was no correlation between delta NSA and age at surgery (p = 0.791), BMI percentile (p = 0.722), Sillence type OI (p = 0.653) or ambulatory status (p = 0.193). There was also no correlation between a lower preoperative NSA or longer length of follow-up (p = 0.174) and a higher delta TFA at latest follow-up (p = 0.567).
There was a 42% (5/12) complication rate in our series. There was a 30% (3/9) incidence of loss of distal epiphyseal fixation of the male FD rod with failed rod expansion during growth. In case number 7, lateral transcortical migration of the proximal RR occurred with recurrent CV. The NSA measured 107° at latest follow-up. This child was wheelchair-bound before and after surgery due to severe recurrent kyphoscoliosis and opposite lower limb deformity, and surgical revision was not advised. The final complication occurred when the RR in case number 8 migrated proximally into the gluteal region, causing pain and hip abduction limitation. The RR was exchanged to an FD rod that was inserted percutaneously. This was the only case that underwent revision surgery.
Comparative analysis of data showed that age at surgery (p = 0.342), preoperative NSA (p = 0.765), OI type (p = 0.067), type of rod used (FD vs RR) (p = 0.310) and BMI percentile (p = 0.735) were not associated with a higher complication rate.
Discussion
The role of orthopaedic surgery in OI is primarily to prevent and manage fractures or deformities. Long bone deformity correction and intramedullary stabilisation improve function and decrease the incidence of fractures.9 Our study aimed to evaluate the use of the Fassier technique for the correction of proximal femur deformities in OI.2 The technique resulted in a correction of the NSA to within the normal range in all cases, and this correction was maintained in 83% of cases at a mean three-year follow-up. Complications related to the rods used occurred in five cases, with one patient that required reoperation.
The incidence of CV in OI was reported as 10% by Aarabi et al. with an average NSA of 99 degrees.1 Ambulatory children with CV will limp due to the shortened lever arm of the femoral neck with resultant abductor weakness muscles and a Trendelenburg gait. Finidori described a technique to correct CV using telescopic rods inserted retrograde on the lateral cortex of proximal femur and exiting at the piriformis fossa.10 Wagner described using multiple K-wires to achieve and maintain the deformity correction of CV in young children.11
The specific surgical technique to correct CV in OI that we used combined the techniques of Finidori and Wagner and was first described by Fassier in 2003.4 Fassier et al. published their experience with this technique in 18 hips of children with OI in 2008.2 In South Africa, Robertson and George described a similar surgical technique for CV in OI type III, using K-wires and a Williams rod in Ave hips.5 The advantages of this technique are that the K-wires allow for proximal control during deformity correction, the K-wire cerclage combination provides fixation of the proximal fragment, and intramedullary fixation of the femur is still achieved with the intramedullary rod.
We achieved correction of the NSA from 96.8° preoperatively to 137° postoperatively in 13 hips. This result compares favourably with those of Fassier et al. (18 hips, NSA 84.6° to 119.5°) and Robertson and George (five hips, NSA 60° to 130°), who both used a similar technique.2,5 Compared to these two studies, our cohort had a less severe deformity, but a higher postoperative NSA. We demonstrated maintenance of this correction with a mean NSA of 133° at 39 months (3.25 years) follow-up. In the short term, this compares well with the results reported by Fassier et al. (NSA of 114.4 at 4.3 years).
All patients in this study received intravenous bisphosphonate treatment. While el-Sobky et al., in a comparative study, concluded that surgery plus bisphosphonate treatment improves the ambulatory status of patients with OI, we were not able to confirm an improvement in ambulatory status as we only had data related to wheelchair use.12 Preoperatively, two of the eight patients were wheelchair-bound, and they remained so postoperatively.
None of the patients had intraoperative complications. Implant-related complications were observed in 41% (5/12) of hips. While the complication rate is relatively high, the most common complication is a 30% (3/9) incidence of distal loss of epiphyseal fixation of the male component of the FD rod and subsequent failure of rod expansion. This rate compares favourably to the 45% failure of rod expansion reported by Landrum et al.13 In a recent paper, Holmes et al. found that eccentric epiphysial placement may predispose the rod to fail to expand, and we now pay particular attention to achieving this outcome.14 One RR that migrated proximally required revision, and this was revised to an FD rod. The last complication was a recurrent deformity due to lateral transcortical migration of the proximal RR and loss of fixation in a child with severe OI type III. All patients achieved radiological union, and there were no cases of postoperative infection or avascular necrosis of the hip.
We could not demonstrate an association between the loss of correction of the NSA and age at surgery, BMI, Sillence type OI, ambulatory status, or length of follow-up. Due to our small sample size and relatively short follow-up, our results were prone to a type 2 error. Further studies with larger numbers and longer follow-up are required to determine whether the deformity correction will be lasting, and which factors are associated with loss of correction. Despite the small sample size, there are very few studies that report on the results of treatment of the proximal femoral deformity in OI, and its findings are therefore important. A further limitation of this study is that we were unable to measure the Hilgenreiner's epiphyseal angle (HEA) accurately due to pelvic distortion and variable positioning of the lower limbs during AP pelvis X-rays during follow-up. Despite this shortcoming, we were able to measure the NSA reliably. This was a single-centre study, and external validity needs to be confirmed with further studies. We included cases of 'false CV' and cases with a decreased NSA that was not lower than 110°. We included these because the proximal deformity in OI is varied and often multiplanar, and the advantages of the Fassier technique make it applicable in all these situations.
Despite these shortcomings, we were able to report effective and safe deformity correction with the Fassier technique in this series of children with CV secondary to OI in the short term.
Conclusion
The Fassier technique effectively corrected CV in children with moderate and progressively deforming OI. The deformity correction was maintained in the short term. The complication rate was high, but mainly related to the failed expansion of the FD rods. Further studies are required to determine the long-term outcome of this technique.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. Prior to commencement of the study, ethics approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee BREC/00001850/2020. All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
SMM: data capture, data analysis, first draft preparation, manuscript preparation PHM: study conceptualisation, study design, data capture, data analysis, manuscript revision
DMT: study conceptualisation, data capture, manuscript revision LCM: study design, manuscript revision
ORCID
Mwelase SM https://orcid.org/0000-0001-9952-0986
Maré PH https://orcid.org/0000-0003-1599-7651
Thompson DM https://orcid.org/0000-0003-2607-3999
Marais LC https://orcid.org/0000-0002-1120-8419
References
1. Aarabi M, Rauch F, Hamdy R, Fassier F. High prevalence of coxa vara in patients with severe osteogenesisimperfecta. J Pediatr Orthop. 2006;26(1):24-28. https://doi.org/10.1097/01.bpo.0000189007.55174.7c. [ Links ]
2. Fassier F, Sardar Z, Aarabi M, et al. Results and complications of a surgical technique for correction of coxa vara in children with osteopenic bones. J Pediatr Orthop. 2008;28(8):799-805. https://doi.org/10.1097/bpo.0b013e31818e19b7. [ Links ]
3. Noonan K, Enright W. Bone plating in patients with type III osteogenesis imperfecta: results and complications. Iowa Orthop J. 2006;26:37-40. [ Links ]
4. Fassier F, Glorieux FH. Osteogenesis imperfecta. In: Surgical Techniques in Orthopaedics and Traumatology. Paris: Elsevier SAS; 55-050-D-30,2003, 8. [ Links ]
5. Robertson A, George JA. A surgical technique for coxa vara in osteogenesis imperfecta. SA Orthop J. 2005;4(1):16-19. [ Links ]
6. Georgescu I, Gavriliu S, Nepaliuc I, et al. Burnei's technique of femoral neck variation and valgisation by using the intramedullary rod in osteogenesis imperfecta. J Med Life. 2014;7(4):493-98. [ Links ]
7. Palomo T, Fassier F, Ouellet J, et al. Intravenous bisphosphonate therapy of young children with osteogenesis imperfecta: skeletal findings during follow up throughout the growing years. J Bone Miner Res. 2015;30(12):2150-57. https://doi.org/10.1002/jbmr.2567. [ Links ]
8. The jamovi project (2020). jamovi (Version 1.2)[Computer Software]. Downloaded from: https://www.jamovi.org on 30 August 2020. [ Links ]
9. Esposito P, Plotkin H. Surgical treatment of osteogenesis imperfecta: current concepts. Curr Opin Pediatr. 2008;20(1):52-57. https://doi.org/10.1097/mop.0b013e3282f35f03. [ Links ]
10. Finidori, G. Treatment of osteogenesis imperfecta in children. Ann N Y Acad Sci. 1988;543:167-69. https://doi.org/10.1111/.1749-6632.1988.tb55329.x. [ Links ]
11. Widmann RF, Hresko MT, Kasser JR, Millis MB. Wagner multiple K-wire osteosynthesis to correct coxa vara in the young child: experience with a versatile 'tailor-made' high angle blade plate equivalent. J Pediatr Orthop B. 2001;10(1):43-50. [ Links ]
12. el-Sobky MA, Zaky Hanna AA, Basha NE, et al. Surgery versus surgery plus pamidronate in the management of osteogenesis imperfecta patients: a comparative study. J Pediatr Orthop B. 2006;15(3):222-28. https://doi.org/10.1097/01.bpb.0000192058.98484.5b. [ Links ]
13. Landrum M, Birch C, Richards BS. Challenges encountered using Fassier-Duval rods in osteogenesis imperfecta. Curr Orthop Pract. 2019;30(4):318-22. [ Links ]
14. Holmes K, Gralla J, Brazell C, et al. Fassier-Duval rod failure: is it related to positioning in the distal epiphysis? J Pediatr Orthop. 2020;40(8):448-52. https://doi.org/10.1097/bpo.0000000000001513. [ Links ]
Received: January 2021
Accepted: February 2021
Published: March 2022
* Corresponding author: sandilemwelase@gmail.com
Editor: Dr Greg Firth, University of the Witwatersrand, Johannesburg, South Africa
Funding: No funding was secured for this research.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}
{kind=link}