










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.21 n.1 Centurion 2022
http://dx.doi.org/10.17159/2309-8309/2022/v21n1a2
GENERAL ORTHOPAEDICS
A retrospective file audit of preoperative anaemia in patients referred to an anaesthesiology clinic before elective orthopaedic surgery
Anne-Cecilia van MarieI; Petra-Marie AchoII; Christine O ChepapeII; Reitumetse M MahlabaII; Precious DlaminiII; Samkelisiwe MaguguII; Kamogelo K MahlohlaII; Nicole TeisII; Anna M KachelhofferIII; Gina JoubertIV; Marius J CoetzeeII, *
IDepartment of Haematology and Cell Biology, School of Pathology, Faculty of Health Sciences, University of the Free State and National Health Laboratory Service, Bloemfontein, South Africa
IIDepartment of Haematology and Cell Biology, School of Pathology, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIIDepartment of Anaesthesiology, School of Clinical Medicine, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IVDepartment of Biostatistics, School of Basic Medical Sciences, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: Preoperative anaemia has been shown to be associated with increased postoperative morbidity and mortality, prolonged hospital stay, and increased allogeneic blood transfusions. With elective surgery there is time to manage preoperative anaemia. The aim was to determine the prevalence of preoperative anaemia and evaluate how anaemia was investigated and managed in adult patients who were referred from the Orthopaedic Clinic to the Universitas Academic Hospital Anaesthesiology Clinic between January 2016 and December 2018
METHODS: The retrospective file audit included patient demographics, comorbidities and chronic medication, indication for elective surgery, haemoglobin level at first clinic visit, laboratory investigations done for anaemia, dates of clinic visits and surgery, whether the anaemia was corrected before surgery, and if there were any perioperative red cell transfusions
RESULTS: A total of 178 patients were included. The cut-off value for anaemia was 13 g/dL in both sexes. Forty-four patients (25%, 95% CI 19-32%) had preoperative anaemia with a median haemoglobin of 12.25 g/dL (IQR 11.2; 12.7). Their mean age was 63.3 (SD ± 10.0) years. Fifteen patients (34%) were booked for knee arthroplasty and 24 patients (55%) for hip replacement surgery. No workup was done for the anaemia, and only 15/44 (34%) anaemic patients received any form of treatment. Eighteen anaemic patients (41%) received perioperative red cell transfusions. Eight of the transfused patients (44%) developed postoperative sepsis, while five were still anaemic postoperatively
CONCLUSION: The prevalence of preoperative anaemia before elective orthopaedic surgery (25%) was the same as that reported before patient blood management was introduced internationally. None of the anaemic patients had a diagnostic workup and therefore did not receive therapy targeted at the cause of the anaemia. Perioperative red cell transfusions could have been significantly reduced. The clinic now focuses on managing preoperative anaemia
Level of evidence: Level 3
Keywords: preoperative anaemia, elective orthopaedic procedures, patient blood management, preoperative care, blood transfusion
Introduction
Preoperative anaemia has been shown in systematic reviews to be associated with increased morbidity and mortality in general surgery, cardiovascular surgery and orthopaedic surgery.13 Patient blood management emphasises the diagnosis and treatment of anaemia and prevention of blood loss, rather than the use of allogeneic red cell transfusions.4,5 The South African Surgical Outcomes Study showed that preoperative anaemia was independently associated with in-hospital mortality (odds ratio 1.657) and admission to critical care (odds ratio 1.487).6 The prevalence of preoperative anaemia was 1 727/3 610 (47.8%) in that study. Jadhunandan et al. showed preoperative anaemia was associated with a three-fold higher risk of postoperative mortality in open abdominal surgery.7 Conradie et al. reported that the prevalence of preoperative anaemia was 28% in 375 adult patients presenting for elective non-cardiac, non-obstetric surgery in the Western Cape.8 In that study, 37% of the anaemic patients had iron deficiency, but only 9% of these patients received iron before surgery. There is sufficient evidence that preoperative anaemia is a significant problem in South Africa that requires active management to improve patient outcomes. It is estimated that 17.8 million South Africans are anaemic.9,10
At least two general international guidelines emphasise the need for the identification and prevention of preoperative anaemia.11,12 Palmer et al. and Goodnough et al.provide international guidelines for the management of preoperative anaemia in orthopaedic surgery.5,13 The South African Society of Anaesthesiologists (SASA) published their Perioperative Patient Blood Management Guidelines in 2020.14 Palmer et al. and the SASA guidelines both recommend that the cut-off level for anaemia in both sexes is 13 g/dL.5,14 Women have a smaller blood volume than men, even though they may lose the same amount of blood for a given procedure. Women with a preoperative haemoglobin of 12 g/dL often require perioperative red cell transfusions.5,7,15 The current World Health Organization definitions of anaemia of 12 g/dL in women and 13 g/dL in men are being revisited.16
Preoperative anaemia screening clinics can manage preoperative anaemia in patients before elective surgery.17 The Anaesthesiology Clinic at Universitas Academic Hospital (UAH) evaluates patients before elective surgery, especially orthopaedic surgery. Spahn's systematic review of 2010 reported preoperative anaemia in 25% of patients undergoing elective total hip or knee arthroplasty, and 50% of patients undergoing surgical hip fracture repair.18 That review also showed that preoperative anaemia was associated with a blood transfusion rate of 45 ± 25% and postoperative infections in 44 ± 15%, poorer physical functioning and recovery, and increased length of hospital stay and mortality. Meybohm et al. showed that in 10 017 German patients, the preoperative anaemia rate was 14.8% for elective knee joint arthroplasty, 22.9% for elective hip joint arthroplasty and 45.0% for duo-prosthesis implantation.19 Patients with anaemia had a prolonged hospital stay and increased mortality.
Our primary aim was to assess the prevalence of anaemia in patients referred to the UAH Anaesthesiology Clinic for preoperative assessment and management prior to elective orthopaedic surgery. Secondary objectives were to document i) in how many of these patients the underlying cause for the anaemia was investigated; ii) in how many of these patients the anaemia was corrected prior to surgery; and iii) which of these patients required blood transfusions perioperatively. The information would help to improve the management of preoperative anaemia.
Patients and methods
The retrospective audit included all adult patients who were referred to the UAH Anaesthesiology Clinic from the Orthopaedic Clinic before elective orthopaedic surgery between January 2016 and December 2018. We identified patients from the attendance list of the UAH Anaesthesiology Clinic. A total of 178 adult patients were included. Patients younger than 18 years, and those who required emergency orthopaedic surgery, were excluded. Information was collected from patient notes and hospital, pharmacy and laboratory
information systems. The pseudoanonymised data included basic patient demographics, comorbidities and chronic medications, the indication for elective surgery, haemoglobin level at first clinic visit, laboratory investigations done to determine the cause of anaemia, whether anaemia was corrected before surgery, the dates of the clinic visits and surgery, the postoperative haemoglobin levels, whether any perioperative red cell transfusions were given, as well as any documented postoperative complications. For all 178 patients, information relating to the study objectives was available and therefore no patients were excluded due to missing data. The data was captured on a Microsoft Excel spreadsheet. The cut-off level for anaemia was 13 g/dL in both sexes.14 The design followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies.20 Data was analysed by the Department of Biostatistics at the University of the Free State using SAS Version 9.4 (SAS Institute Inc, Cary NC, USA). Age was summarised by mean and standard deviation. Other numerical variables were summarised by medians and percentiles due to skew distributions. Categorical variables were summarised by frequencies and percentages. Comparison of subgroups regarding categorical variables were done using contingency tables with chi-squared or Fisher's exact tests. Numerical variables were compared using Mann-Whitney tests.
Results
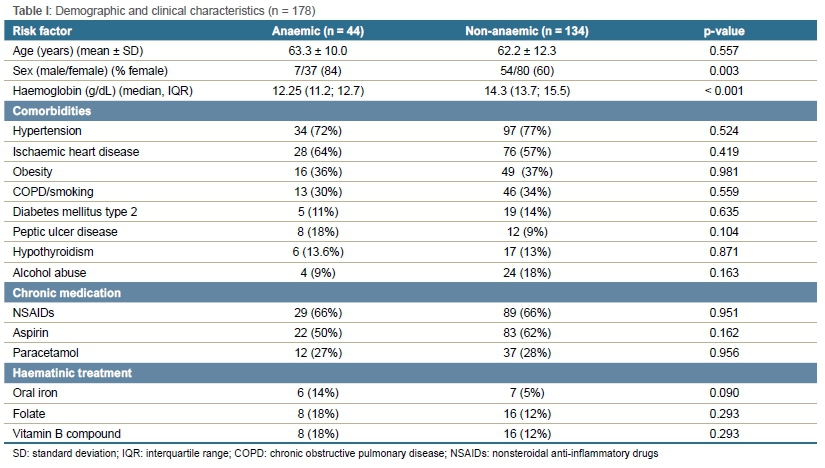
A hundred and seventy-eight patients were included. Forty-four patients (25%, 95% CI 19-32%) were found to be anaemic during their preoperative Anaesthesiology Clinic assessment (Table I). Their mean age was 63.3 years (SD ± 10.0), and 84% were female (compared to 60% of non-anaemic patients, p < 0.001). The median haemoglobin in the anaemic subgroup was 12.25 g/dL (IQR 11.2; 12.7) compared to that of the non-anaemic subgroup which was 14.3 g/dL (p < 0.001). Of the anaemic patients, 29 (66%) regularly used nonsteroidal anti-inflammatory drugs (NSAIDs). Unexpectedly, apart from screening tests for renal function, no laboratory investigations for the anaemia were done. Among the anaemic patients, the most common comorbidities were hypertension (72%), followed by ischaemic heart disease (64%). None of the comorbidities, chronic medication or haematinic treatment differed significantly between the anaemic and non-anaemic subgroups. Of the 44 anaemic patients, three were booked for knee arthroscopy, 15 (34%) for total knee replacement, one for shoulder acromioplasty, one for tibial osteotomy, and the remaining 24 (55%) for hip replacement surgery. The median time between the clinic visit and surgery for the anaemic patients was 76.5 days (range 1-488).
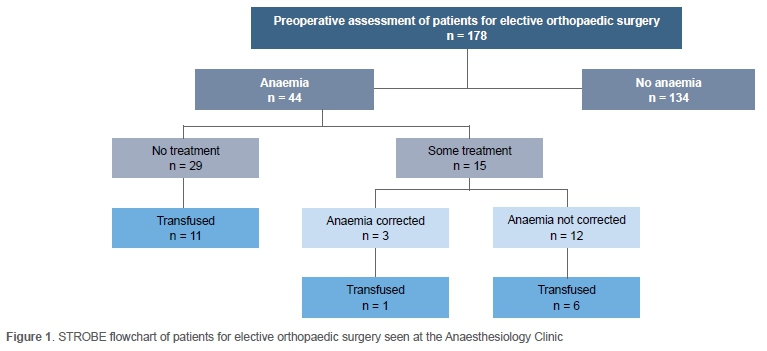
The flow diagram in Figure 1 summarises the patients' clinical course. Only 15/44 (34%) anaemic patients received some treatment for anaemia, which consisted of a varying combination of vitamin B complex, folic acid and oral iron. The anaemia was corrected before surgery in only three of these patients.
Eighteen (41%) of the 44 anaemic patients received perioperative red cell transfusions. One patient received three units, nine patients received two units each and the remaining eight patients received one unit of red cell concentrate each. Seven of the 18 patients who received blood transfusions were on some form of haematinic treatment. The median preoperative haemoglobin level of transfused patients was 11.5 g/dL (range 9.2-12.7). Fourteen of the patients who received blood transfusions were among the 32 anaemic patients who were also regularly using NSAIDs and aspirin. Eight of the 18 patients (44%) who received perioperative blood transfusions developed postoperative sepsis. Ten patients (10/44 = 23%), five of whom had been transfused, were anaemic following surgery. However, this may be an underestimate as a postoperative haemoglobin level was only documented in 13 of the 44 anaemic patients.
Discussion
The prevalence of anaemia in our study was 25%. This is similar to the 20% reported by Saleh et al. in 2007.21 It is also in the range reported in Spahn's meta-analysis of patients undergoing elective orthopaedic surgery before 2010.18 Transfusion rates in arthroplasty surgery are currently decreasing, but the rates depend on the specific hospital setting.22 Recently, Bolz et al. reported that the Michigan Arthroplasty Collaborative Quality Initiative managed to reduce the transfusion rate from 14.82% in 2011 to 1.12% in 2017 by introducing patient blood management education.23
Of concern is that no attempt was made to diagnose the cause of the anaemia in the 44 anaemic patients, even though there was often enough time to investigate and correct the anaemia, with a median time of 76.5 days between the first clinic visit and surgery. The use of NSAIDs by 66% of the anaemic patients might have contributed to their anaemia.
The Society for the Advancement of Patient Blood Management recommends that tests be done to diagnose the common causes of anaemia: iron deficiency anaemia, anaemia of inflammation, anaemia of chronic renal disease, and folate or vitamin B12 deficiency.24 The Australian Blood Authority guidelines simply recommend a full blood count, iron studies including ferritin, C-reactive protein and renal function tests.25 The aetiology of any anaemia needs to be established to guide therapy.
Despite documented anaemia, 29 of 44 patients (66%) received no treatment. The treatment for the other 15 anaemic patients was haphazard and mostly inadequate, as the anaemia was only corrected in time for surgery in three of the anaemic patients (Figure 1). Iron deficiency is the most common nutritional deficiency that contributes to preoperative anaemia.8,21,26 With sufficient time interval (> 6 weeks) before surgery, oral iron supplementation is appropriate. Intravenous iron should be considered if oral iron is poorly tolerated, ineffective (inadequate haemoglobin response), in cases of ongoing blood loss or functional iron deficiency and when the planned surgery is fairly urgent.15,27 Iron deficiency can be rectified within a month by administering intravenous iron.21,22 Where appropriate, an erythropoietin can be combined with intravenous iron to manage anaemia of chronic disease, another common cause of anaemia among surgical patients.28 This combination therapy is also endorsed by the SASA 2020 Perioperative Patient Blood Management Guidelines to reduce postoperative transfusions in patients with non-iron deficiency (e.g. erythropoietin, vitamin D or folate acid deficiency) undergoing elective surgery.14 The routine use of erythropoietin is, however, discouraged due to its potential increased thrombotic risk.27 These measures correct anaemia more safely, and mostly cost far less, than equivalent red cell transfusions.
It is not certain why the one patient whose anaemia had been corrected received a red cell transfusion. In our study population, 44% of the 18 anaemic patients who received blood transfusions developed postoperative sepsis. As we did not collect exhaustive clinical information, we could not exclude other contributing factors to the infections. However, Everhart et al. report that in hip and knee arthroplasty, the odds ratio for surgical site infections increases from 1.97 when one unit of red cells is transfused, to 7.40 when more than three units are transfused.29
The sample of patients was not very large and consisted only of patients referred to the Anaesthesiology Clinic because they needed optimisation of their clinical condition before elective surgery. As a result, the patient cohort consisted mainly of older patients with comorbidities. Regarding the prevalence of preoperative anaemia, this patient cohort is probably not representative of the general population undergoing elective orthopaedic surgery. Most (84%; p < 0.001) of the patients with preoperative anaemia were women. This female preponderance has been noted previously.26 Considering their smaller blood volume, this puts them at greater risk of postoperative complications.14 In retrospect, we did not take into account that Bloemfontein is 1 387 m above sea level, and therefore our cut-off levels should probably have been increased by 0.5 g/dL.30,31
The clinic had mainly focused on comorbidities other than anaemia in the past. Barrett et al. previously demonstrated the need to improve training and knowledge of basic transfusion principles and perioperative anaemia management at our hospital.32 Following this study, the clinic now follows the SASA Perioperative Patient Blood Management Guidelines in order to reduce the rate of transfusions in elective orthopaedic surgery.14,33
This retrospective file audit primarily focused on the prevalence of preoperative anaemia in patients referred to the UAH Anaesthesiology Clinic. Only if patients were found to be anaemic at the first clinic visit was additional information regarding anaemia investigation and management before surgery, as well as perioperative blood transfusions and associated complications, collected. As a result, true comparisons with the non-anaemic cohort, especially with regard to the frequency of perioperative blood transfusions and postoperative complications, cannot be made. Some conclusions should therefore be interpreted with caution.
Because an estimated 17.8 million South Africans are anaemic, there is an urgent need for better management of preoperative anaemia.9,10 In a period when the COVID-19 pandemic has strained our blood supply even further, the era of preoperative red cell transfusions in elective surgery should be something of the past.5,34 The World Health Organization has recently issued a policy brief about the urgent need to implement patient blood management.35
Conclusion
Despite our small cohort, we were able to demonstrate that preoperative anaemia is prevalent, but often missed or neglected, and contributes to unnecessary blood transfusions and postoperative complications. Our study illustrates the urgent need for multidisciplinary teams or clinics that screen patients for anaemia before elective surgery, as well as for the implementation of clear treatment guidelines for preoperative anaemia.17
Acknowledgements
The authors would like to thank the Finance and IT Departments of Universitas Academic Hospital for the provision of data about blood usage. We would also like to thank the nurses at the Universitas Academic Hospital Orthopaedic and Anaesthesiology Clinics. We would like to acknowledge the contribution of our fellow author, Prof. Anna M Kachelhoffer (1935-2021) who worked so hard to collect all the patient files and information, but unfortunately passed away before being able to see this publication.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. Prior to commencement of the study, ethics approval was obtained from the University of the Free State Health Sciences Research Ethics Committee (UFS-HSD2019/0372/3007) as well as from the Free State Department of Health (FS_FS201904-002). All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed written consent was not obtained from patients for being included in the study as the study was retrospective and the research data was pseudoanonymised.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
AvM: suggested the topic, was a study leader who supervised the students and wrote the final draft manuscript
PMA, CC, RM, PD, SM, KM and NT: wrote the protocol, did the data collection and wrote the first draft report
AMK: supervised the collection of data
GJ: helped to plan the study, performed the analysis, and assisted with the write-up of the manuscript
MJC: was a study leader who supervised the students and wrote the final draft manuscript
ORCID
Van Marie A https://orcid.org/0000-0002-6569-4061
Acho P-Mhttps://orcid.org/0000-0003-0982-9926
Chepape CO https://orcid.org/0000-0002-5943-3308
Mahlaba RM https://orcid.org/0000-0001-7986-8774
Dlamini Phttps://orcid.org/0000-0002-0527-9501
Magugu S https://orcid.org/0000-0001-6033-2750
Mahlohla KK https://orcid.org/0000-0001-9966-3178
Teis N https://orcid.org/0000-0002-0240-926X
Kachelhoffer AM https://orcid.org/0000-0003-0418-7493
Joubert G https://orcid.org/0000-0002-3728-6925
Coetzee MJ https://orcid.org/0000-0003-2762-0966
References
1. Fowler AJ, Ahmad T, Phull MK, et al. Meta-analysis of the association between preoperative anaemia and mortality after surgery. Br J Surg. 2015;102(11):1314-24. https://doi.org/10.1002/bjs.9861. [ Links ]
2. Padmanabhan H, Siau K, Curtis J, et al. Preoperative Anemia and outcomes in cardiovascular surgery: systematic review and meta-analysis. Ann Thorac Surg. 2019;108(6):1840-48. https://doi.org/10.10164.athoracsur.2019.04.108. [ Links ]
3. Potter LJ, Doleman B, Moppett IK. A systematic review of pre-operative anaemia and blood transfusion in patients with fractured hips. Anaesthesia. 2015;70(4):483-500. https://doi.org/10.1111/anae.12978. [ Links ]
4. Thomson J, Hofmann A, Barrett CA, et al. Patient blood management: A solution for South Africa. S Afr Med J. 2019;109(7):471-76. https://doi.org/10.7196/SAMJ.2019.v109i7.13859. [ Links ]
5. Palmer AJR, Gagne S, Fergusson DA, et al. Blood management for elective orthopaedic surgery. J Bone Joint Surg Am. 2020;102(17):1552-64. https://doi.org/10.2106/JBJS.19.01417. [ Links ]
6. Marsicano D, Hauser N, Roodt F, et al. Preoperative anaemia and clinical outcomes in the South African Surgical Outcomes Study. S Afr Med J. 2018;108(10):839-46. https://doi.org/10.7196/SAMJ.2018.v108i10.13148. [ Links ]
7. Jadhunandan K, Moodley Y, Gopalan PD. Preoperative anaemia in patients undergoing open intra-abdominal surgery at a South African tertiary hospital. South Afr J Anaesth Analg. 2020;26(1):24-29. https://doi.org/10.36303/sajaa.2020.26.L2250. [ Links ]
8. Conradie WS, Biesman-Simons T, Roodt F, et al. A multicentre prospective observational study of the prevalence of preoperative anaemia and iron deficiency in adult elective surgical patients in hospitals in Western Cape Province, South Africa. S Afr Med J. 2019;110(1):65-68. https://doi.org/10.7196/SAMJ.2019.v110i1.14051. [ Links ]
9. Kassebaum NJ, Jasrasaria R, Naghavi M, et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood. 2014;123(5):615-24. https://doi.org/10.1182/blood-2013-06-508325. [ Links ]
10. Kassebaum NJ, Collaborators GBDA. The global burden of anemia. Hematol Oncol Clin North Am. 2016;30(2):247-308. https://doi.org/10.1016/j.hoc.2015.11.002. [ Links ]
11. Kotze A, Harris A, Baker C, et al. British Committee for Standards in Haematology guidelines on the identification and management of pre-operative anaemia. Br J Haematol. 2015;171(3):322-31. https://doi.org/10.1111/bjh.13623. [ Links ]
12. Mueller MM, Van Remoortel H, Meybohm P, et al. Patient blood management: recommendations from the 2018 Frankfurt Consensus Conference. JAMA. 2019;321(10):983-97. https://doi.org/10.1001/jama.2019.0554. [ Links ]
13. Goodnough LT, Maniatis A, Earnshaw P, et al. Detection, evaluation, and management of preoperative anaemia in the elective orthopaedic surgical patient: NATA guidelines. Br J Anaesth. 2011;106(1):13-22. https://doi.org/10.1093/bja/aeq361. [ Links ]
14. Wise R, Bishop D, Gibbs M, et al. South African Society of Anaesthesiologists Perioperative Patient Blood Management Guidelines 2020. South Afr J Anaesth Analg. 2020;26(6):S1-68. https://doi.org/10.36303/SAJAA.2020.26.6.S1. [ Links ]
15. Muhoz M, Gomez-Ramirez S, Liumbruno GM. Peri-operative anaemia management in major orthopaedic surgery: the need to find a pathway. Blood Transf. 2017;15(4):289-91. https://doi.org/10.2450/2017.0296-16. [ Links ]
16. Pasricha SR, Colman K, Centeno-Tablante E, et al. Revisiting WHO haemoglobin thresholds to define anaemia in clinical medicine and public health. Lancet Haematol. 2018;5(2):e60-62. https://doi.org/10.1016/S2352-3026(18)30004-8. [ Links ]
17. Lin Y. Preoperative anemia-screening clinics. Hematology Am Soc Hematol Educ Program. 2019;2019(1):570-76. https://doi.org/10.1182/hematology.2019000061. [ Links ]
18. Spahn DR. Anemia and patient blood management in hip and knee surgery: a systematic review of the literature. Anesthesiology. 2010;113(2):482-95. https://doi.org/10.1097/ALN.0b013e3181e08e97. [ Links ]
19. Meybohm P, Kohlhof H, Wirtz DC, et al. Preoperative anaemia in primary hip and knee arthroplasty. Z Orthop Unfall. 2020;158(02):194-200. https://doi.org/10.1055/a-0974-4115. [ Links ]
20. Elm EV, Altman DG, Egger M, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806-808. https://doi.org/10.1136/bmj.39335.541782.ad. [ Links ]
21. Saleh E, McClelland DB, Hay A, et al. Prevalence of anaemia before major joint arthroplasty and the potential impact of preoperative investigation and correction on perioperative blood transfusions. Br J Anaesth. 2007;99(6):801-808. https://doi.org/10.1093/bja/aem299. [ Links ]
22. Kimball CC, Nichols CI, Vose JG. Blood transfusion trends in primary and revision total joint arthroplasty: recent declines are not shared equally. J Am Acad Orthop Surg. 2019;27(20):e920-27. https://doi.org/10.5435/JAAOS-D-18-00205. [ Links ]
23. Bolz NJ, Zarling BJ, Markel DC. Long-term sustainability of a quality initiative program on transfusion rates in total joint arthroplasty: a follow-up study. J Arthroplasty. 2020;35(2):340-46. https://doi.org/10.1016/j.arth.2019.08.056. [ Links ]
24. SABM. SABM Administrative and Clinical Standards for Patient Blood Management Programs, 5th ed. Society for the Advancement of Blood Management; 2019. [ Links ]
25. National Blood Authority. Patient Blood Management Guidelines: Module 2 Perioperative. Canberra: National Blood Authority; 2012. [ Links ]
26. Muhoz M, Laso-Morales MJ, Gómez-Ramírez S, et al. Pre-operative haemoglobin levels and iron status in a large multicentre cohort of patients undergoing major elective surgery. Anaesthesia. 2017;72(7):826-34. https://doi.org/10.1111/anae.13840. [ Links ]
27. Munting KE, Klein AA. Optimisation of pre-operative anaemia in patients before elective major surgery - why, who, when and how? Anaesthesia. 2019;74 Suppl 1:49-57. https://doi.org/10.1111/anae.14466. [ Links ]
28. Pagano D, Milojevic M, Meesters MI, et al. 2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. The Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Cardiothoracic Anaesthesiology (EACTA). Eur J Cardiothorac Surg. 2018;53(1):79-111. https://doi.org/10.1093/ejcts/ezx325. [ Links ]
29. Everhart JS, Sojka JH, Mayerson JL, et al. Perioperative allogeneic red blood-cell transfusion associated with surgical site infection after total hip and knee arthroplasty. J Bone Joint Surg Am. 2018;100(4):288-94. https://doi.org/10.2106/JBJS.17.00237. [ Links ]
30. Jarret AH. Boyden Observatory [A Concise History]. Acta Academica 1979(12). Available from: https://www.ufs.ac.za/docs/librariesprovider22/physics-documents/boyden-documents/all-documents/boyden-history-1087-eng.pdf?sfvrsn=42af921_0. Accessed 7 July 2021. [ Links ]
31. World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization; 2011. (WHO/NMH/NHD/MNM/11.1). [ Links ]
32. Barrett C, Mphahlele K, Khunou I, et al. The knowledge of transfusion and related practices among doctors at Universitas Academic Complex, Bloemfontein, South Africa. Transfus Apher Sci. 2020;59(3):102739. https://doi.org/10.1016/j.transci.2020.102739. [ Links ]
33. Newman C, Tran P, McGregor S, Bramley D. Patient blood management strategies in total hip and knee arthroplasty. Curr Orthop Pract. 2018;29(1):31-36. https://doi.org/10.1097/bco.0000000000000577. [ Links ]
34. Wise RD, Gibbs MW, Louw VJ. Lockdown and our national supply of blood products. S Afr Med J. 2020;110(5):12904. https://doi.org/10.7196/SAMJ.2020.v110i5.14749. [ Links ]
35. World Health Organization. The urgent need to implement patient blood management: policy brief. Geneva: World Health Organization; 2021. Available from: https://apps.who.int/iris/handle/10665/346655. Accessed 20 October 2021. [ Links ]
Received: November 2020
Accepted: October 2021
Published: March 2022
* Corresponding author: coetzeemj@ufs.ac.za
Editor: Prof. Michael Held, University of Cape Town, Cape Town, South Africa
Funding: Local departmental resources.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.


{kind=link}
{kind=link}