










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.20 n.2 Centurion 2021
http://dx.doi.org/10.17159/2309-8309/2021/v20n2a5
PAEDIATRIC ORTHOPAEDICS
Polio-like deformity: a diagnostic dilemma
Khaled A Ben SalemI; Pieter H MaréI, *; Matthew GoodierII; Leonard C MaraisIII; David M ThompsonI
IDepartment of Orthopaedic Surgery, Grey's Hospital, School of Clinical Medicine, University of KwaZulu-Natal, South Africa
IIDepartment of Radiology, Grey's Hospital, School of Clinical Medicine, University of KwaZulu-Natal, South Africa
IIIDepartment of Orthopaedic Surgery, School of Clinical Medicine, University of KwaZulu-Natal, South Africa
ABSTRACT
BACKGROUND: Significant advances have been made in the global effort to eradicate polio. Vaccine-associated poliovirus, or other enteroviruses, may still affect the anterior horn cell and cause acute flaccid paralysis. Following the acute disease, residual paralysis results in lower motor neuron weakness, altered growth and deformity. Our study aims to describe the clinical manifestations of a group of children that mimic that of classic paralytic poliomyelitis
METHODS: We identified six children from our paediatric orthopaedic database that presented with polio-like deformities. Their clinical and imaging records were reviewed and described, together with the clinical manifestations of paralytic poliomyelitis
RESULTS: Limb hypoplasia, pathological gait patterns and foot deformities were consistent features. The median leg length discrepancy was 2.5 cm (range 2-4 cm). The gait patterns observed included a Trendelenburg gait in 33% (n=2), a short limb gait in 50% (n=3), and one case with a combination of Trendelenburg, short limb and steppage gait. Tensor fascia lata contracture was present in 50% (n=3) of our patients. Foot deformities ranged from calcaneo-cavo-valgus to equino-cavo-varus deformities
CONCLUSION: Despite significant advances made in the global fight to eradicate polio, we still see children with clinical manifestations reminiscent of the disease. Orthopaedic surgeons should remain familiar with the assessment and diagnosis of the sequelae of paralytic poliomyelitis
Level of evidence: Level 5
Keywords: poliomyelitis, vaccine-associated paralytic poliomyelitis, polio-like deformity, acute flaccid paralysis
Introduction
The last case of wild-strain poliomyelitis in South Africa was reported in 1989.1 Despite this, we still see patients with clinical deformities resulting from paralysis reminiscent of that caused by the poliovirus (so-called polio-like deformity). Most orthopaedic surgeons familiar with the assessment and management of polio are nearing the end of their careers.2 Current orthopaedic reference textbooks have removed sections on polio. As availability bias may limit our ability to consider and diagnose uncommon conditions, it is essential that orthopaedic surgeons remain familiar with the clinical manifestations of paralytic polio.3
The most common viral motor neuronopathy in children presenting as acute flaccid paralysis (AFP) results from enterovirus infections. These viruses include coxsackievirus, enterovirus 68 and 71, echovirus and polio.4 Previously the focus was mainly on poliovirus. Significant strides have been made in the fight to eradicate polio globally. However, this goal has not been achieved yet and polio may still be imported from endemic areas. South Africa lost its 'polio-free' status in 2017 due to insufficiencies in its vaccination programme and surveillance systems.5 This was reinstated by the WHO's African Regional Certification Committee (ARCC) in September 2019. Limitations in surveillance may result in some cases of AFP being missed. Vaccine-associated paralytic polio (VAPP) and circulating vaccine-derived poliovirus (cVDPV) remain a risk with the use of the oral attenuated polio vaccine (OPV). There has recently been a resurgence of interest in virus strains other than polio that have caused outbreaks of a febrile paralytic illness initially described as 'polio-like illness'.6 This syndrome was eventually named acute flaccid myelitis (AFM) to differentiate it from disease caused by the poliovirus. Residual lower motor neurological deficit was noted in 84% of cases at median nine-month follow-up.6
While several causes of polio-like paralysis remain, the entity itself and its clinical characteristics in particular, remains poorly characterised. We could find no previous reports on the orthopaedic manifestations of paralytic enterovirus infection. This study aims to describe a cohort of patients presenting with polio-like deformities.
Methods
We retrospectively reviewed data from cases who presented to our tertiary level paediatric orthopaedic unit over the seven years from January 2011 to December 2018. The unit serves a population of approximately 4.3 million people, of which 1.6 million are children between the ages of 0 and 14 years.7
Following ethical approval, cases were identified from our paediatric orthopaedic database. All patients, below the age of 18 years, presenting with polio-like deformity were included. 'Poliolike deformity' was defined as the combination of asymmetric lower motor neuron (LMN) paralysis, deformity and altered growth consistent with that seen with poliomyelitis. Spine MRI investigation was routinely performed to identify features suggestive of previous neuroinvasive viral infection. Patients with deformity and neurological deficit due to other causes were excluded. The differential diagnosis for this presentation includes other causes of lower motor neuropathy, such as hereditary motor sensory neuropathies, congenital spinal abnormalities (spinal dysraphism), previous traumatic or toxic neuritis as well as neuroinvasive viral infection.
The records were reviewed for vaccination history, any previous significant febrile illness (with or without signs of meningism) and history of AFP. Clinical records were reviewed for the pertinent findings during neurological evaluation, as well as documentation of joint contractures, deformities and leg-length discrepancy (LLD). X-ray and MRI records were reviewed from our institution's PACS and included in our analysis. Motor function was assessed by testing and grading power according to the Medical Research Council (MRC) grading.8 Decreased or absent tone and reflexes were findings consistent with an LMN lesion.
The indication for MRI was any child who presented with unexplained LMN weakness and deformity or altered growth in keeping with the typical findings of poliomyelitis.
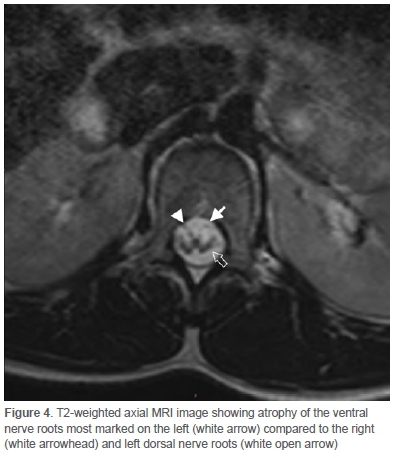
All MRI scans were performed using a 1.5 Tesla Phillips Intera MRI machine. Standard spine sequences included STIR, T2 and T1 sagittal acquisitions and T2 and T1 axial acquisitions. Intravenous gadolinium was not routinely used. Five of the MRI scans were evaluated by a specialist radiologist with seven years' experience and a postgraduate diploma in neuroradiology. Axial images were evaluated for the presence of ventral nerve root atrophy which was considered to be present if the ventral (motor) nerve roots of the cauda equina were markedly smaller in calibre than the dorsal (sensory) roots at the same level. One of the scans (patient 4) did not have MRI images available for review, and the MRI report from the patient records was used.
Results
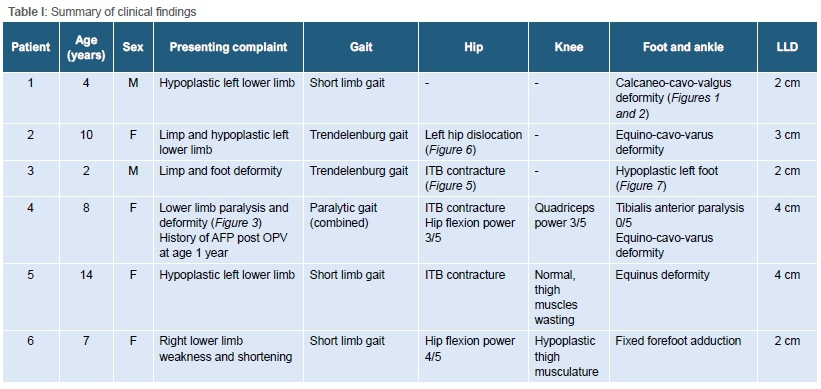
We identified six patients that met the clinical criteria for polio-like deformity. MRI findings consistent with previous neuroinvasive viral infection were present in 67% (n=4). Their mean age was 8 years (range of 2-14). Their presenting complaints and clinical findings are summarised in Table I.
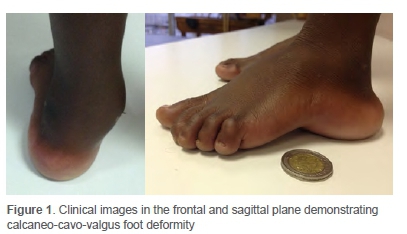
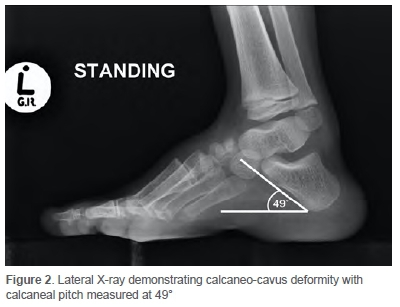
All patients had some degree of limb hypoplasia with LLD of median 2.5 cm (range 2-4). Limp was another consistent feature with 33% (n=2) presenting with Trendelenburg gait, a short limb gait was present in 50% (n=3), and one child presented with a combination of Trendelenburg, short limb and steppage gait. Tensor fascia lata (TFL) contracture is a classic feature of polio and was present in 50% (n=3) of our patients. Foot deformities were present in all cases. These ranged from mere hypoplasia to calcaneo-cavo-valgus (Figures 1 and 2) at one end, and equino-cavo-varus deformity at the other end of the spectrum.
VAPP was confirmed in one patient who presented to the paediatric service with AFP after OPV administration during infancy. She presented at our orthopaedic unit at the age of 8 years with an LMN paresis affecting the left lower limb and classic deformities of polio in the hip, knee and foot and ankle (Figure 3). No clear history of AFP could be elicited in any of the other cases.

Two of the MRI scans were normal. Three of the patients had a clear subjective reduction in the calibre of the ventral nerve roots of the cauda equina (Figure 4). In one patient, this finding was present bilaterally, and in two patients, this finding was unilateral. One patient had long segment signal abnormality involving the entire spinal cord.
Discussion
Polio is caused by three related enteroviruses (types 1, 2 and 3). Fewer than 1% of polio infections in children result in AFP.9 A recovery phase follows AFP during which the muscle recovers rapidly in the first six months and slower over the subsequent months until up to two years. No recovery occurs after this in the residual paralysis phase. Residual paralysis following enterovirus infection may be mild. Asymmetric weakness and incomplete recovery of paralysis result in muscle imbalance. In the growing child, active muscles shorten, and paralysed muscles overlengthen. Over time this results in altered bone growth and joint contractures. A greater disparity in strength will result in earlier deformity. A mild discrepancy, however, over a long period, will also result in deformity, altered growth and joint development. These deformities often manifest years after the initial paralysis and are recognised as the typical manifestations of paralytic polio.10
Our study describes a cohort of patients with the typical clinical features of paralytic polio.
The typical joint contractures and deformities seen in polio occur during growth as a result of the muscle imbalance in the residual paralysis phase after neuroinvasive viral infection. A shortened limb is due to interference with growth.11 The pattern of paralysis is classically asymmetric. All our patients had asymmetric growth disturbance and presented with varying degrees of limb hypoplasia and shortening. Sharrard published detailed and extensive analyses of the pattern of cell destruction in the spinal cord, as well as muscle recovery in poliomyelitis.12,13 Muscles most frequently completely paralysed have their anterior horn cells located in a narrow zone in the spinal cord (e.g. tibialis anterior).14 Muscles that have their anterior horn cells in a wider region may still be frequently affected (e.g. the quadriceps femoris), but will seldom be completely paralysed.10 This pattern was seen in the child with confirmed VAPP who had complete paralysis of tibialis anterior, (0/5 power) but paresis of the quadriceps (3/5 power). Sensory loss is infrequent. Subsequent motor dysfunction and deformity will depend on the pattern of paralysis.15
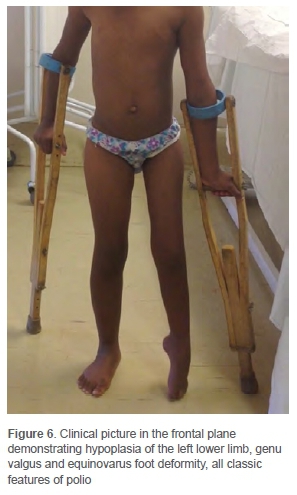
A Trendelenburg gait is a common feature due to abductor paralysis. Gluteus maximus paralysis may result in an extensor lurch during the stance phase of gait. Three children in our series had a Trendelenburg gait due to abductor weakness. We did not see any children with gluteus maximus paralysis. Hip contractures are typically into an abducted, externally rotated and flexed position.2 Abduction contracture is in part the result of TFL contracture. Ober's test identifies TFL contracture (Figure 5). Less frequently, hip instability and dislocation may occur due to paralysed gluteal muscles and strong hip adductors and flexors. This is associated with coxa valga, persistent anteversion and acetabular dysplasia.10 ITB contracture was found in three children in our series. One child presented with a paralytic dislocation (Figure 6).

Quadriceps weakness makes a 'hand on thigh' gait necessary to lock the knee during stance.2 Genu recurvatum deformity may develop if a child bears weight on a flail limb by locking the leg into hyperextension during every stance phase.10 Fixed flexion deformity of the knee occurs more frequently due to quadriceps weakness and strong knee flexors.10 Contracture is often severe. TFL contracture also results in external tibial torsion. Quadriceps weakness was found in one child, while in two children thigh hypoplasia was present without weakness. None of the children in our series had knee flexion or recurvatum deformities.
Tibialis anterior is one of the most frequently completely paralysed muscles.10 This results in a foot drop and fixed equinus deformity. Depending on the pattern of paralysis, a range of deformities may occur. These include equinus, calcaneus, hindfoot varus or valgus, pes cavus or pes planus, or any combination of these.2 Foot deformities were present in all children in our series. These ranged from calcaneo-cavo-valgus deformity in one child (Figures 1 and 2) to equino-cavo-varus deformities in two children. One child each had forefoot adduction, pure equinus and hypoplasia (Figure 7).

MRI findings consistent with previous poliomyelitis were present in 69% (n=4). This is consistent with a report by Teoh et al., which found 75% (n=3) abnormal spine MRIs in cases of AFP due to neuroinvasive viral infection.16 Only one of our cases had a clear history of AFP. This was confirmed as VAPP. It is possible that the other cases may have been the result of undiagnosed enterovirus infection, causing lower motor neuronopathy. Once the child presents with the late sequelae of paralytic enterovirus infection, no serological test or imaging investigation can confirm the diagnosis definitively. Spine MRI investigation may strengthen the clinical suspicion. During the acute phase of the disease, MRI features could include diffuse signal abnormality in the cord (as was present in patient 4). In the chronic phase the only changes may be that of ventral root atrophy (these features were observed in patients 1-3).
Significant progress has been made since 1988 by the Global Polio Eradication Initiative (GEPI) and the World Health Organization. Since 2000, 13 million cases of polio have been prevented by the oral polio vaccine (OPV), and the disease has been reduced by more than 99%.17 Only wild poliovirus (WPV) type 1 remains endemic in Pakistan and Afghanistan. The last case of WPV type 2 was recorded in 1999, and WPV type 3 in 2012.18 South Africa has a well-established vaccination programme which has been massively successful in eradicating wild polio infection. In rare instances the attenuated Sabin poliovirus administered as the OPV may undergo genetic drift during replication, developing neurovirulent properties. This may cause AFP identical to that caused by WPV. The rate has been reported between 3.8 and 4.7 cases per million live births.19 These viruses may be transmitted as circulating vaccine-derived poliovirus (cVDPV). The small risk of VAPP and cVDPV is offset by the immense public health benefit of OPV. Ironically, the management of a cVDPV outbreak is ensuring efficient vaccination in the area to stop the spread of the mutated neurovirulent viral strain. While there are advantages to OPV, it is being phased out as wild polio is eradicated to prevent the occurrence of VAPP and cVDPV. This started in April 2016 as a global coordinated effort to change from trivalent OPV (containing types 1, 2 and 3) to bivalent OPV (type 1 and 3).17
Several limitations of our study warrant consideration. Due to the rarity of the syndrome we were able to identify only a small number of cases. We were unable to confirm a history of AFP in all but one child. This may be explained by a situation where the meningitic nature of a febrile illness was not appreciated. A mild neurological deficit, especially in young children, can easily be missed. As the subsequent clinical course is that of progressive recovery, healthcare opinion may not have been sought. This is supported by the 2016 report that South African national AFP surveillance was below the heightened WHO target for 2015/16 of 4/100 000 with several districts reporting 0 or 1/100 000 cases.18 Electrophysiological testing would have been useful but was not available for paediatric patients at our hospital during the study period. Despite these shortcomings, the classic clinical findings of paralytic polio, supported by MRI findings in most cases, prompted us to compile this report. We could not And any previous published reports of this clinical entity. Clinicians should remain familiar with sequelae of paralytic polio because, to quote the philosopher George Santayana, 'those who cannot remember the past are condemned to repeat it'.20
Conclusion
While major strides have been made towards worldwide polio eradication, non-polio enteroviruses, VAPP and cVDPV may still cause a polio-like deformity. AFP surveillance should be strengthened to ensure all cases are identified early and deformities prevented or treated early. If the child presents years later, thorough clinical evaluation should exclude other causes of lower motor neuronopathy. Typical features include asymmetric limb hypoplasia combined with LMN weakness and TFL contracture. MRI may be useful to identify features of previous neuroinvasive viral infection.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010. All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Ethical approval was granted by the University of KwaZulu-Natal Biomedical Research Ethics committee (BE380/18).
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
KABS: Data capture, first draft preparation, manuscript revision
PHM: Manuscript revision and review
MG: Manuscript preparation and review
LCM: Manuscript revision and review
DMT: Study design, data capture, manuscript review
ORCID
Ben Salem KA https://orcid.org/0000-0003-2778-3140
Maré PH https://orcid.org/0000-0003-1599-7651
Goodier M https://orcid.org/0000-0002-6091-1768
Marais LC https://orcid.org/0000-0002-1120-8419
Thompson DM https://orcid.org/0000-0003-2607-3999
References
1. Khuzwayo LS, Kuonza LR, Ngcobo NJ. Evaluating the acute flaccid paralysis surveillance system in South Africa, 2005-2009: an analysis of secondary data. Pan Afr Med J. 2013;14:86. [ Links ]
2. Joseph B, Watts H. Polio revisited: reviving knowledge and skills to meet the challenge of resurgence. J Child Orthop. 2015;9:325-38. [ Links ]
3. Morgenstern J. Cognitive errors in medicine: The common errors. FirstlOEM blog, September 15, 2015. Available at: https://first10em/cognitive-errors/. [ Links ]
4. Teoh H, Carey K, Sampaio H, et al. Inherited paediatric motor neuron disorders: beyond spinal muscular atrophy. Neural Plast. 2017:6509493. https://doi.org/10.1155/2017/6509493. [ Links ]
5. No authors listed. South Africa certified polio-free. https://www.nicd.ac.za/south-africa-certified-polio-free/. [Accessed 19 June 2020]. [ Links ]
6. Messacar K, Schreiner TL, Van Haren K, et al. Acute flaccid myelitis: a clinical review of US cases 2012-2015. Ann Neurol. 2016;80(3):326-338. https://doi.org/10.1002/ana.24730. [ Links ]
7. No authors listed. 2018 KwaZulu-Natal citizen satisfaction survey: analytical report. http://www.statssa.gov.za/publications/Report-03-00-07/Report-03-00-072018.pdf. [Accessed 19 June 2020]. [ Links ]
8. Medical Research Council. Aids to the investigation of the peripheral nervous system. Memorandum No. 45. London, Her Majesty's Stationery Office; 1976. [ Links ]
9. Centers for Disease Control and Prevention. Chapter 18: Poliomyelitis. In: Hamborsky J, Kroger A, Wolfe S, editors. Epidemiology and Prevention of Vaccine-Preventable Diseases. 13th ed. Washington D.C. Public Health Foundation; 2015. [ Links ]
10. Sharrard WJW. Affectations of the lower motor neurone. In: Sharrard WJW. Paediatric Orthopaedics and Fractures. 2nd edition. Blackwell Scientific Publications; 1979. p. 889-942. [ Links ]
11. Faraj AA. Poliomyelitis: Orthopaedic management. Curr Orthop. 2006;20:41-46. [ Links ]
12. Sharrard WJW. Correlation between changes in the spinal cord and muscle paralysis in poliomyelitis - a preliminary report. Proc R Soc Med. 1953;46(5):346-49. [ Links ]
13. Sharrard WJW. Muscle recovery in poliomyelitis. J Bone Joint Surg (Br). 1955;37-B:63-79. [ Links ]
14. Sharrard WJW. The distribution of the permanent paralysis in the lower limb in poliomyelitis. J Bone Joint Surg (Br). 1955;37-B:540-58. [ Links ]
15. Sharrard WJW. Paralytic deformity in the lower limb. J Bone Joint Surg (Br). 1967;49-B:731-47. [ Links ]
16. Teoh H, Mohammad SS, Britton PN, et al. Clinical characteristics and functional motor outcomes of Enterovirus 71 neurological disease in children. JAMA Neurol. 2016;73(3):300-307. [ Links ]
17. World Health Organization. Poliomyelitis. https://www.who.int/news-room/q-a-detail/poliomyelitis. [Accessed 19 June 2020]. [ Links ]
18. Howard W, Moonsamy S, Manamela J, et al. Acute flaccid paralysis surveillance for polio, South Africa and other African countries. NICD Communicable Diseases Surveillance Bulletin. 2017;15(1):3-8. [ Links ]
19. Platt LR, Estivariz CF, Sutter RW. Vaccine-associated paralytic poliomyelitis: a review of the epidemiology and estimation of the global burden. J Infect Dis. 2014;210(S1):S380-389. [ Links ]
20. Santayana G. Reason in Common Sense. 1905. p. 284. [ Links ]
Received: July 2020
Accepted: October 2020
Published: May 2021
* Corresponding author: phmare@gmail.com
Editor: Prof. Jacques du Toit, Stellenbosch University, South Africa
Funding: No funding was secured for this research.
Conflict of interest: The authors have no conflict of interest to declare.


{kind=link}