










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.19 n.2 Centurion May./Jun. 2020
http://dx.doi.org/10.17159/2309-8309/2020/v19n2a5
SPINE
Correlation of Soft tissue Projection in Injured NEcks (CSPINE) - Prevertebral soft tissue measurement in paediatric cervical spine trauma
McCaul JI; Horn AII; McCaul MIII; Dix-Peek SIV
IMBChB(UCT), FCS(SA)Orth(UCT), MMed(UCT); Consultant, Division of Orthopaedic Surgery, Groote Schuur Hospital and Red Cross War Memorial Children's Hospital; University of Cape Town, South Africa
IIMBChB(UP), FCS(SA)Orth(UCT), MMed(UCT); Consultant, Division of Orthopaedic Surgery, Groote Schuur Hospital; University of Cape Town, South Africa
IIIMSc(Clin Epi)(SU); Senior lecturer, Division of Epidemiology and Biostatistics, Department of Global Health, Stellenbosch University, South Africa
IVMBBCh(Wits), FCS(SA)Orth, MMed(UCT); Consultant, Red Cross War Memorial Children's Hospital; University of Cape Town, South Africa
ABSTRACT
BACKGROUND: In paediatric trauma, measured increase in prevertebral soft tissue thickness on a lateral cervical spine (C-spine) X-ray is interpreted as swelling, raising suspicion of C-spine injury. Defining swelling in absolute measurements is cumbersome - children's sizes vary. Published recommendations are largely lacking in evidence. There may be potentially more consistent tools, for example, to measure soft tissue thickness as a ratio of vertebral body width. The aim of this study was to determine whether consistent, measurable prevertebral soft tissue to vertebral body width ratios exist for use as simple diagnostic tools in the assessment of swelling and injury in paediatric C-spine trauma
PATIENTS AND METHODS: C-spine trauma X-rays taken at a South African children's hospital were randomly sampled. Seventy-one un-intubated X-rays from 85 controls were used to identify normal ratios. The authors measured vertebral bodies and soft tissue at each level, created all possible ratios, then chose the two least variable - one for the upper and one for the lower C-spine. Twenty cases aided in determining diagnostic accuracy for C-spine injury.
RESULTS: Mean soft tissue at the second cervical vertebral level (c2) was 38% of the seventh vertebra (C7) (95% confidence interval [CI]: 34-41.9%, standard error [SE]: 2.0%). Mean c6 soft tissue was 65.6% of C7 vertebra (95% CI: 61.9-69.3%, SE: 1.9%). In diagnosing C-spine injury, a receiver operating characteristic (ROC) curve calculation gave an empirical optimal cut-point of 53.9% and 74.4% respectively. Using practical cut-offs of 55% at c2 and 75% at c6 yielded specificities of 93.8% (95% CI: 84.8-98.3%) and 81.8% (95% CI: 70.4-90.2%), with negative predictive values of 90.9% (95% CI: 81.3-96.6%) and 91.5% (95% CI: 81.3-97.2%) respectively
CONCLUSION: Consistent and specific ratios exist in the upper and lower paediatric C-spine. Both ratios have poor sensitivities and positive predictive values and so are poor screening tools; however, a positive result can raise suspicion of C-spine injury in high-risk individuals. This can help to motivate for further investigations such as computer tomography (CT) or magnetic resonance imaging (MRI), which may not be easily accessible in under-resourced settings. However, further research is required to validate the diagnostic value of these ratios
Level of evidence: Level 4
Keywords: prevertebral soft tissue, vertebral body width, cervical spine, paediatric, C-spine trauma, ratio
Introduction
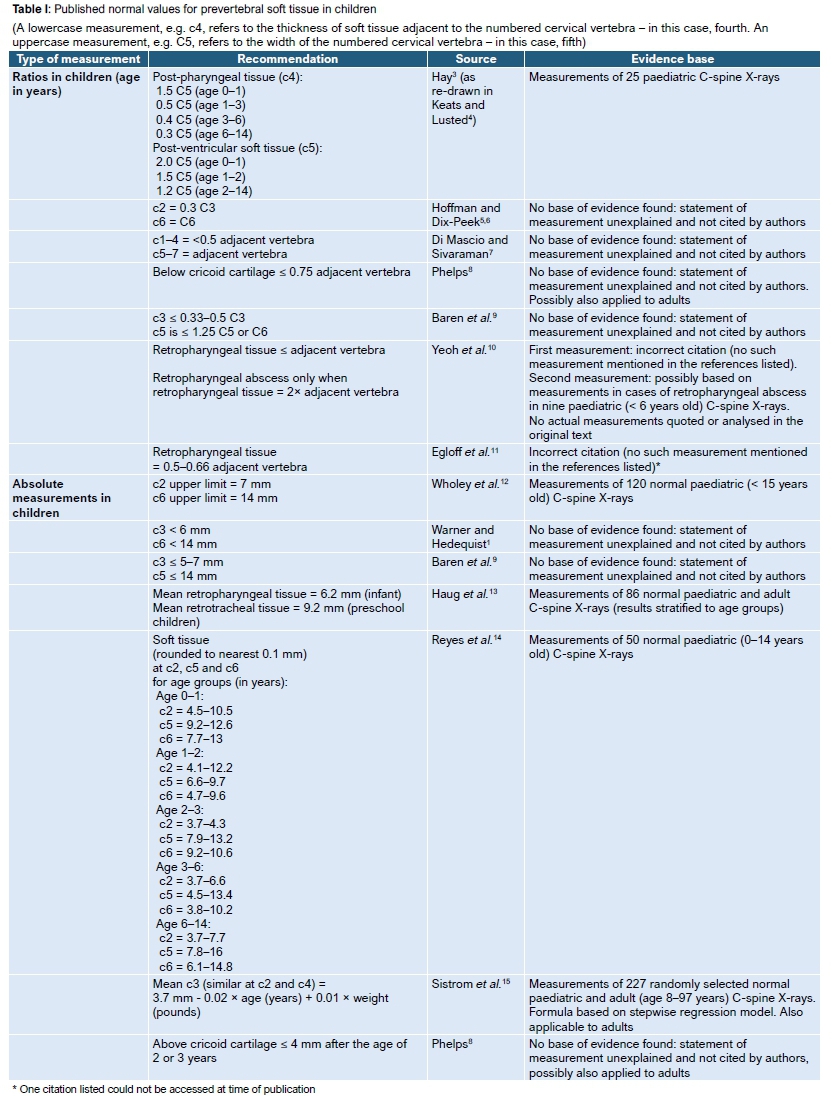
Paediatric cervical spine (C-spine) injury is rare but potentially devastating.1 Although soft tissue swelling on X-ray has been referred to as an aid in identifying injury,1,2 published measurement methods and recommendations on what constitutes swelling vary, as does the diagnostic significance of said swelling.3-16 Measurements in millimetres (mm) may not be applicable across wide age ranges and an alternative is measurement as a ratio of vertebral body width. Some published normal values are based on primary evidence, but many statements regarding measurement norms are uncited, or citations do not correctly support the measurement.3-15Table I provides a summary of published normal values.
The purpose was to determine whether measurement of prevertebral soft tissue as a ratio of vertebral body width on paediatric lateral C-spine trauma X-rays is consistent in uninjured, un-intubated patients and, as a secondary objective, is of diagnostic value in identifying C-spine injury. The hypothesis was that one such measurement would be identified for the upper and one for the lower C-spine; that these would have clinically acceptably narrow variability across age groups and sexes; and that measurements greater than these would correlate with C-spine injury.
Other secondary objectives were to describe the atlanto-dens interval (ADI), basion-dens interval (BD) and effect of intubation on soft tissue thickness.
Materials and methods
Study design and setting
A retrospective pragmatic quantitative cross-sectional study randomly sampled digital lateral C-spine X-rays taken in patients under 13 years of age at Red Cross War Memorial Children's Hospital in Cape Town, South Africa, between December 2012 and February 2016. All X-rays were assigned consecutive numbers, then selected according to a computer-generated random number sequence. X-rays taken for non-traumatic reasons were excluded. Additional X-rays of injured patients from pre-existing records and from the same period were added to the random sample to increase the number of injuries available for analysis to complete the secondary objectives. Patient folders were reviewed. No follow-up was performed.
Dedicated erect or supine lateral C-spine views on conventional, mobile unit and whole-body low dose digital X-rays (LODOX) of patients both with and without C-spine injury were included. Patients assessed as being clinically clear according to the Canadian C-spine,17 National Emergency X-Radiography Utilization Study Group (NEXUS)18 or other pragmatic criteria and that were Anally managed and discharged as having no C-spine injury were classified as controls. Patients with normal C-spine X-ray, computerised tomography (CT) scan or magnetic resonance imaging (MRI) report were also classified as controls. Patients with bony, ligamentous, cervical cord or cervical nerve injury clinically or on imaging were classified as cases. There were 85 controls and 20 cases.
Measurements
Measurements were performed in mm up to one decimal point using the ruler tool of the Phillips iSite® Enterprise radiology system. If an area could not be visualised, those specific measurements only (28 out of 1 365 possible measurements) were treated as missing data.
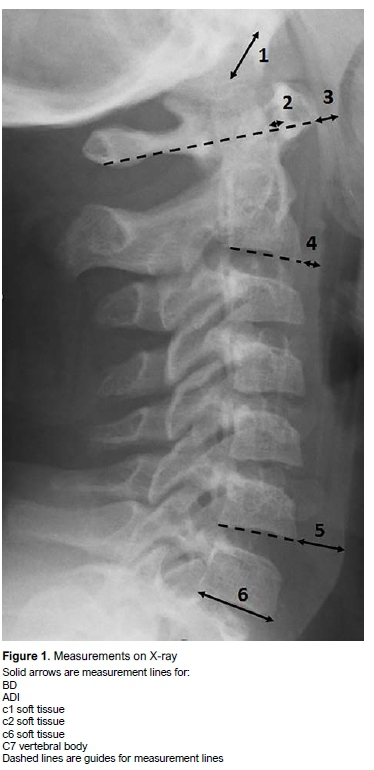
Soft tissue thickness was measured parallel to the adjacent vertebral body's inferior endplate, from the most anterior-inferior aspect of that vertebral body to the most anterior edge of the tissue shadow. As the first cervical vertebra (C1) has no body, measurement started from the most anterior inferior aspect of C1's anterior arch to the anterior edge of the soft tissue, along a line extended from the most inferior projections of C1 anterior and posterior arches. The soft tissue measurements were labelled c1-c7 according to the adjacent vertebra. In intubated cases, if the anterior edge of the soft tissue shadow was obscured by the tube, the measurement was taken up to the most posterior edge of the tube.
Vertebral body width was measured from the most posterior-inferior corner to the most anterior-inferior corner and labelled C2-C7. Atlanto-dens interval (ADI) was measured as drawn from the posterior inferior corner of the anterior arch of C1 to the adjacent anterior border of the odontoid, along the line between the most inferior projections of C1 anterior and posterior arches. Basion-dens distance (BD) was measured from the anterior rim of the foramen magnum to the most prominent superior projection of the dens. See Figure 1 for measurement examples.
The age of the patient was extrapolated from the dates of birth and of the X-ray. Sex was recorded for all patients and, where available, weight in kilograms up to one decimal point. Mechanism of injury was extracted from the clinical information.
Digital radiology reports attached to X-ray, CT and MRI images were examined and any comments on soft tissue and adequacy of images noted. It was recorded whether an injury was identified, excluded or unclear. This was correlated with clinical information regarding examination and management.
Blinding during measurement was not possible as clinical information was digitally linked to images; however, strict measurement protocols as above minimised risk of bias. A single author measured all images.
Statistical methods
A sample size of 60 for the primary objective was calculated by hypothesising clinically acceptably accurate ratios and confidence intervals: a 99% confidence interval (CI) of ±15% around a hypothesised mean of 90% and standard deviation (SD) of 45% was considered sufficient, based on anticipated estimated minimum and maximum values of 20% and 200%. Random sampling was performed until 60 uninjured, un-intubated patients were identified. During this phase 13 intubated patients were also sampled as they were randomly interspersed. Random sampling then continued until another two un-intubated (and one intubated) patients were added. Due to counting error, 11 un-intubated patients were added. Provisional data analysis was performed before and after the sample was enlarged. Repeat data analysis failed to show a clinically significant difference in the consistency of measurements after the increase of the sample size, so it was concluded that further enlarging the sample was unlikely to change final results and so data collection was concluded. Twenty injured patients were captured during random sampling as well as additions from preexisting records.
Data management and analysis was conducted in Stata 14. Simple descriptive statistics were used for demographic data. Age was grouped into categories according to international conventions.19,20 The primary outcome was reported using means and 95% CIs. The appropriate parametric and non-parametric tests were used and a p-value of <0.05 was considered statistically significant. Ratios for every soft tissue thickness to every vertebral body width (42 ratios) were created in un-intubated controls. Two ratios with the lowest standard error (one for upper and one for lower C-spine) were defined as the most consistent. In determining diagnostic accuracy of soft tissue swelling to predict presence of injury, these ratios of cases and controls (in un-intubated patients) were correlated to injury using point-biserial correlation. In addition, receiver operating characteristic (ROC) analysis was used to compare these ratios to aid in identifying the optimal empirical diagnostic cut-point. A sensitivity analysis was conducted by excluding poor quality X-rays. Missing data was excluded.
Results
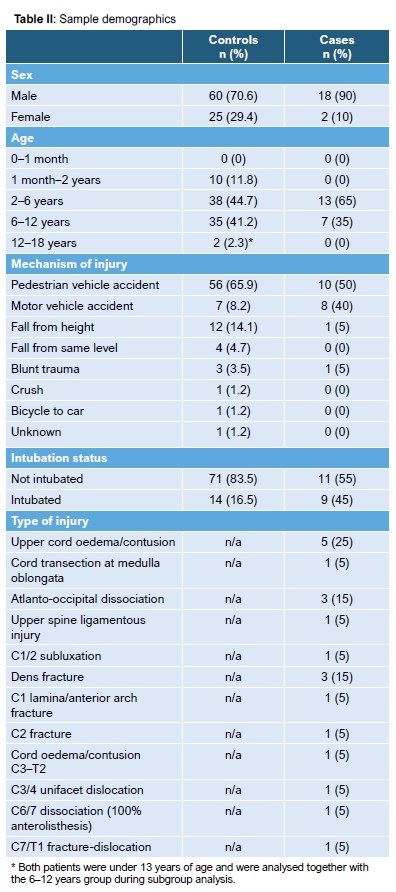
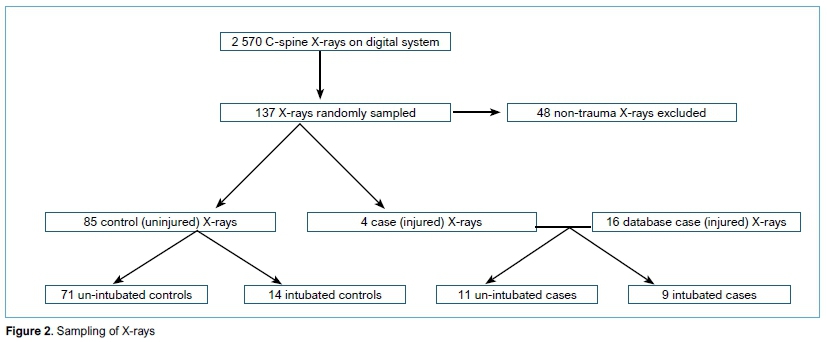
A total of 2 570 C-spine X-rays were digitally accessible, of which 893 were conventional or mobile C-spine X-rays and 1 731 were LODOX, including dedicated lateral C-spine views. During random sampling, 48 X-rays taken for non-traumatic reasons were excluded. Four patients with injury were identified by chance and added to the 16 known cases (Figure 2). Table II provides a summary of demographic data.
The ADI was measurable in 78 controls and the mean was 2.6 mm (SD 1.1). ADI was measurable in all 20 cases and had a mean of 3.6 mm (SD 3.3). BD was measurable in 48 controls and had a mean of 9.4 mm (SD 2.8). BD was measurable in 13 cases with a mean of 11.3 mm (SD 5.8).
Main outcome results
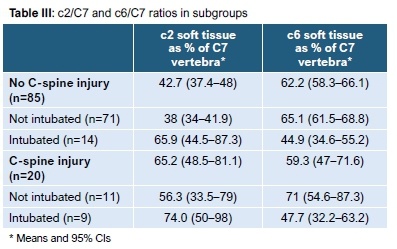
The soft tissue/vertebral body ratio for the upper C-spine with the lowest variance in un-intubated controls was c2/C7, with mean c2 soft tissue being 38% of C7 vertebra (95% CI: 34-41.9%, SE: 2.0%, variance: 2.5%). For the lower C-spine the most consistent ratio was c6/C7 with mean c6 soft tissue being 65.6% of C7 vertebra (95% CI: 61.9-69.3%, SE: 1.9%, variance: 2.3%). As sensitivity analysis, excluding X-rays reporting that the neck was flexed or the patient was crying, resulted in more precision and very slightly lower mean in c2/C7 (2% less) but no clinical or statistical difference. For these reasons, and as the study is pragmatic, it was decided to keep these X-rays in the overall analysis. In the study sample, those poor X-rays were not repeated before further clinical decisions were made. See Table III for a summary of these ratios in different patient groups.
Secondary outcome results: correlation and diagnostic accuracy
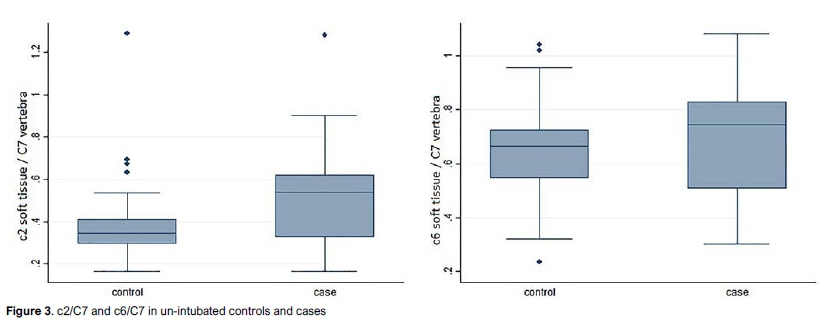
Soft tissue ratios at c2 and c6 in un-intubated controls were compared to un-intubated cases to determine correlation between soft tissue thickness and presence of injury. The point-biserial correlation coefficient for c2/C7 was 0.3060 (p-value: 0.0085) and for c6/C7 was 0.1059 (p-value: 0.3660) (Figure 3).
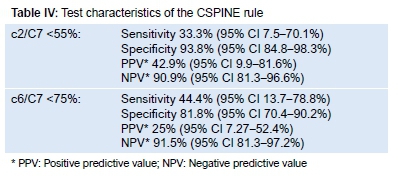
Soft tissue thickness at these levels (as a ratio of C7 vertebra) in un-intubated controls was again compared to un-intubated cases to determine cut-off points with optimal sensitivity and specificity to diagnose C-spine injury. Most importance was placed on specificity. ROC curve calculation gave empirical optimal cut-points of 53.9% for c2/C7 and 74.4% for c6/C7. To create a clinically practical and easy-to-remember 'CSPINE rule' (Correlation of Soft Tissue Projection in Injured Necks), these values were rounded up to a cut-off of 55% at c2 and 75% at c6, which yields specificity of 92.3% (95% CI: 83-97.5%) and 81% (95% CI: 70.4-90.2%) respectively, with negative predictive values of 90.9% (95% CI: 81.3-96.6%) and 91% (95% CI: 81.3-97.2%). See Table IV for a summary of the diagnostic test characteristics and Figure 4 for the ROC curve.

Secondary outcome results: effect of intubation on soft tissue thickness
Soft tissue at each level was, for convenience, expressed as ratios of C7 vertebra and compared between un-intubated and intubated patients (Table V).

Subgroup and confounder analysis
Subgroup analysis was performed for infants (1 month-2 years), young children (2-6 years) and older children (6-13 years). See Table VI for a summary of c2/C7 and c6/C7 in un-intubated control patients in these age groups.

Weight was available for 36 patients. The correlation coefficient for weight compared to soft tissue thickness in un-intubated control patients was -0.2111 (p-value 0.3582) for c2/C7, and -0.3056 (p-value 0.1667) for c6/C7.
Discussion
In our sample of un-intubated, uninjured patients, very consistent soft tissue to vertebral body ratios for both the upper and lower C-spine could be selected. Both were normally distributed and CIs were much narrower than anticipated as acceptable in the sample size calculation hypothesis. At c2, mean soft tissue was 38% of C7 vertebra (95% CI: 34-41.9%) and c6 was 65.6% of C7 vertebra (95% CI: 61.9-69.3%). The serendipitous fact that both ratios with least variability have C7 as denominator makes them extremely convenient. It also indirectly reinforces the need for adequate C-spine X-rays, i.e. where the C7 and first thoracic vertebra interface is visible.
The upper C-spine ratio, c2/C7, was significantly larger in injured compared to uninjured patients regardless of intubation status. When considering only un-intubated patients, this increase was more marked, with a statistically significant correlation coefficient of 30.6% (moderate positive relationship). The lower C-spine ratio, c6/C7, was not significantly different between uninjured and injured patients, even when considering only un-intubated patients. The slight trend towards larger mean soft tissue in injured patients had a statistically non-significant correlation coefficient of 10.6% (weak positive relationship). The fact that upper C-spine swelling correlated more with injury than lower C-spine swelling is likely since most injuries in our sample were in the upper C-spine. This injury pattern is consistent with international literature.21
When testing sensitivity and specificity with the ROC curve, the mean value of c2/C7 at 38% scored poorly with a sensitivity of 66.7% and specificity of 60.9%. Even using the upper limit of the CI, 41.9%, resulted in improving specificity only to 76.6% at the cost of dropping sensitivity to 55.6%. The ROC curve was used to calculate the optimal cut-point for specificity, as C-spine X-rays are not screening tests for the general population - they should be diagnostic tests for patients already screened and suspected of C-spine injury by history and examination. The calculated optimal cut-point of 53.9% provided specificity of 94% without worsening sensitivity further. Rounding up to a more memorable 55% (or even 54%) unfortunately dropped sensitivity down to the next bracket (33.3%). However, CIs for sensitivity are extremely wide due to low prevalence of injury, so the drop is statistically non-significant. The decision was made to suggest the 'CSPINE' rule that c2 soft tissue should be less than 55% of C7 vertebra. The method to develop the CSPINE rule suggesting that c6 soft tissue should be less than 75% of C7 vertebra followed similar patterns. DeBehnke and Havel22 employed comparable methodology in adults and found similar patterns but did not accept any point on the ROC curve as adequate. Patel et al.16also demonstrated similar high specificities and low sensitivities in testing adults using the '7 mm at C2 and 2 cm at C7' rule.
Both ratios have extremely poor sensitivities, and are therefore poor screening tools, but can aid in ruling on injury in patients with high clinical suspicion of injury due to high specificity. The good negative and poor positive predictive values reflect low prevalence of injury.
Intubation in uninjured controls clinically and statistically significantly increased soft tissue thickness in the upper C-spine (c1-3). At c4 there was no difference. Below c4 intubation significantly decreased soft tissue thickness. The lack of difference at c4 is possibly due to the inherent anatomic variability at the level of c4 (location of the glottis), or due to its fulcrum-like mid-position in the trend of upper C-spine tissue increasing and lower C-spine tissue decreasing after intubation. In injured patients, the effect of intubation at c2 and c6 followed the same trend, but without statistical significance. These findings in the upper C-spine are similar to Di Mascio and Sivaraman's7 findings in adults, but the trend of decreased soft tissue thickness below c4 is in contrast to their findings of no difference.
Univariate analysis determined whether weight or age confounded soft tissue thickness. Weight was unavailable in about two-thirds of patients, possibly due to difficulties in placing polytraumatised patients on scales. In our sample, weight and soft tissue thickness had a weak negative correlation but without statistical significance.
Age had no effect on c6/C7, as evidenced by overlap of all three CIs for available age groups. At c2, however, there seemed to be a trend towards decreasing soft tissue thickness as age increased. CIs overlapped between infants and young children, and between young and older children, but were statistically different with no overlap between infants and older children. These, however, come very close to overlapping, with the upper limit in older children being 37.2% and the lower limit in infants being 38.2%. As these values are so close to the all-ages mean it was decided that difference between ages was not clinically significant. The finding of single useful ratios across age groups is in contrast with Hay's3 recommendations which differ between age groups.
Testing diagnostic accuracy and development of the optimal cut-point as a rule in diagnosing C-spine injury were secondary objectives, thus the sample size was not designed for that purpose. The study was powered to measure normal values for soft tissue thickness in uninjured, un-intubated patients. The study sample consisted of a much smaller group of cases than controls. This, however, is more closely representative of clinical practice where C-spine injury has relatively low prevalence, and as this is a cross-sectional study, it was considered a minor limitation. In addition, the specificities have acceptably narrow CIs to be of clinical use. There would need to be 95 cases in order to determine similarly narrow intervals for sensitivity, and there has anecdotally not been that many cases in the history of the hospital since their introduction of digital X-rays. The areas under the curve for the two diagnostic ratios are 0.67 (upper C-spine) and 0.58 (lower C-spine), which shows that prevertebral soft tissue swelling does not have good discriminative value for predicting soft tissue injury, especially in the lower C-spine.
There were only four lower C-spine injuries and they were not specifically sub-analysed. No recommendation can therefore be made regarding the use of these findings in patients with lower C-spine injuries as such. Comments and conclusions about diagnostic accuracy of the CSPINE rule and correlation of soft tissue thickness with presence or absence of injury in this study refer only to the possibility of injury somewhere in the C-spine rather than being directly related to an anatomical area. There is potential for further research in the diagnostic value of these ratios in different types of paediatric C-spine injuries, and validation of the ratios with further research that includes more cases of injury. This further research may help clarify if prevertebral soft tissue swelling should form part of the consideration in assessing for C-spine trauma in children.
The findings are for children between the ages of 1 month and 13 years and may not be generalisable to neonates, adolescents or adults.
Conclusion
This study demonstrates that there are consistent normal values when measuring prevertebral soft tissue thickness as a ratio of vertebral body width in un-injured, un-intubated paediatric patients: soft tissue at c2 and c7 should be 38% and 65.6% of C7 vertebral body, respectively.
However, soft tissue measurement itself does not seem to be very sensitive in predicting injury. A more specific 'CSPINE rule' (soft tissue at c2 and c6 should be less than 55% and 75% of C7 vertebral body, respectively) can be followed. A positive result would raise suspicion of C-spine injury in high-risk individuals and can help to motivate for further investigations such as CT or MRI, which may not be easily accessible in under-resourced settings. However, further research is required to validate the diagnostic value of these ratios.
Acknowledgements
Dr T Mutengwa: research assistant: assistance in folder data collection
Prof. R Dunn: assistance in identifying cases
Dr JP du Plessis: assistance in identifying cases
Mr S Cornelius: information technology assistance
Ms W Smith: library assistance
Ethics statement
Prior to commencement of the study ethical approval was obtained from the following ethical review board: University of Cape Town Health Research Ethics Committee (reference number HREC: 118/2016).
No identifying information for any patient is included in this article. No human subjects were directly involved as it was a review of existing medical records.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
JM contributed to the conception and design of the work; the acquisition, analysis and interpretation of the data for the work; drafting the work; and submitting the final version to be published.
AH contributed to interpretation of the data, review of the manuscript, and study supervision.
MM contributed to study design and data analysis.
SDP contributed to the conception and design, the review of the manuscript, and study supervision.
ORCID
McCaul J https://orcid.org/0000-0003-1011-5912
Horn A https://orcid.org/0000-0002-4159-6520
McCaul M https://orcid.org/0000-0002-2730-6478
Dix-PeekS https://orcid.org/0000-0002-3382-8790
References
1. Warner WC, Hedequist DJ. Cervical spine injuries in children. In: Beaty JH, Kasser JR, eds. Rockwood & Wilkins' Fractures in Children. 6th ed. Lippincott Williams & Wilkins; 2006:775-814. [ Links ]
2. Schöneberg C, Schweiger B, Hussmann B, et al. Diagnosis of cervical spine injuries in children: a systematic review. Eur J Trauma Emerg Surg. 2013;39:653-65. doi:10.1007/s00068-013-0295-1. [ Links ]
3. Hay P. The neck. A roentgenological study of soft tissues. Consideration of the normal and pathological. In: Hoeber PB, ed. Case JT: Annals of Roentgenology. A Series of Monographic Atlases, Vol 9. 2nd ed. New York, NY; 1930. [ Links ]
4. Keats T, Lusted L. Atlas of Roentgeongraphic Measurement. 4th ed. Year Book Medical Publishers Inc.; 1981. [ Links ]
5. Hoffman EB, Dix-Peek S. Cervical spine injuries in children. In: Van As S, Naidoo S, eds. Baby Steps into Paediatric Neuroradiology. Oxford University Press Southern Africa; 2004. [ Links ]
6. Hoffman EB, Dix-Peek S. Cervical spine injuries in children. In: Van As S, Naidoo S, eds. Paediatric Trauma and Child Abuse. Oxford University Press Southern Africa; 2006. [ Links ]
7. Di Mascio L, Sivaraman A. Cervical prevertebral soft tissue swelling in the traumatized patient: what is normality in the intubated patient? Eur J Trauma Emerg Surg. 2009;35(2):165-68. doi:10.1007/s00068-008-8003-2. [ Links ]
8. Phelps PD. Radiology of the pharynx and larynx. In: Kerr AG, Stel PM, eds. Scott-Brown's Otolaryngology Vol 5. 5th ed.; 1987, pp 8-9. [ Links ]
9. Baren JM, Rothrock SG, Brennan J, Brown L. Pediatric Emergency Medicine. Saunders/Elsevier; 2008. http://www.sciencedirect.com/science/book/9781416000877. [ Links ]
10. Yeoh LH, Singh SD, Rogers JH. Retropharyngeal abscesses in a children's hospital. J Laryngol Otol. 1985;99:555-66. doi:10.1017/S0022215100097243. [ Links ]
11. Egloff AM, Kadom N, Vezina G, Bulas D. Pediatric cervical spine trauma imaging: a practical approach. Pediatr Radiol. 2009;39(5):447-56. doi:10.1007/s00247-008-1043-2. [ Links ]
12. Wholey MH, Bruwer AJ, Baker HL. The lateral roentgenogram of the neck. Radiology. 1958;71 (3):350-56. doi:10.1148/71.3.350. [ Links ]
13. Haug RH, Wible RT, Lieberman J. Measurement standards for the prevertebral region in the lateral soft-tissue radiograph of the neck. J Oral Maxillofac Surg. 1991;49(11):1149-51. doi:10.1016/0278-2391(91)90405-B. [ Links ]
14. Reyes MM, Ricalde RR, Tanalgo JB, Baldoz CJ. Prevertebral soft tissue thickness among pediatric patients. Philipp J Otolaryngol Head Neck Surg. 2011;26(2):5-9. http://apamedcentral.org/search.php?where=aview&id=10.0000%2Fpjohns.2011.26.2.5&code=0011PJOHNS&vmode=AR. Accessed January 23, 2016. [ Links ]
15. Sistrom CL, Southall EP, Peddada SD, Shaffer HA. Factors affecting the thickness of the cervical prevertebral soft tissues. Skeletal Radiol. 1993;22(3). doi:10.1007/BF00206147. [ Links ]
16. Patel MS, Grannum S, Tariq A, et al. Are soft tissue measurements on lateral cervical spine X-rays reliable in the assessment of traumatic injuries? Eur J Trauma Emerg Surg. 2013;39(6):613-18. doi:10.1007/s00068-013-0302-6. [ Links ]
17. Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001;286(15):1841-48. http://www.ncbi.nlm.nih.gov/pubmed/11597285. Accessed September 13, 2017. doi:10.1001/jama.286.15.1841. [ Links ]
18. Hoffman JR, Mower WR, Wolfson AB, Todd KH, Zucker MI. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. N Engl J Med. 2000;343(2):94-99. doi:10.1056/NEJM200007133430203. [ Links ]
19. Knoppert D, Reed M, Benavides S, et al. Position paper: Paediatric age categories to be used in differentiating between listing on a model essential medicines list for children. 2007. http://archives.who.int/eml/expcom/children/Items/PositionPaperAgeGroups.pdf. Accessed August 2, 2017. [ Links ]
20. Williams K, Thomson D, Seto I, et al. Standard 6: Age groups for pediatric trials. Pediatrics. 2012;129(Suppl 3). http://pediatrics.aappublications.org/content/129/Supplement_3/S153. Accessed August 2, 2017. doi:10.1542/peds.2012-0055l. [ Links ]
21. Platzer P, Jaindl M, Thalhammer G, et al. Cervical spine injuries in pediatric patients. J Trauma Inj Infect Crit Care. 2007;62(2):389-96. doi:10.1097/01.ta.0000221802.83549.46. [ Links ]
22. DeBehnke DJ, Havel CJ, Laib R. Utility of prevertebral soft tissue measurements in identifying patients with cervical spine fractures. Ann Emerg Med. 1994;24(6):1111124. doi:10.1016/ S0196-0644(94)70242-X. [ Links ]
 Correspondence:
Correspondence:
Dr J McCaul
H49 Old Main Building, Groote Schuur Hospital
Anzio Rd, Observatory, Cape Town, 7925
Tel: +27 83 682 0060
Email: jkmccaul@gmail.com
Received: September 2019
Accepted: January 2019
Published: May 2020
Funding: No funding was received for this study.
Conflict of interest: All authors declare that they have no conflict of interest with respect to this article.


{kind=link}
{kind=link}
{kind=link}