










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.19 no.1 Centurion feb./mar. 2020
EDITORIAL
Surgery of state patients in private hospitals - a free lunch?
Held MI; Workman MIII; Le Roux JIII; Nortje MIV; Dunn RV
IMD, PhD, MMed Orth, FCOrthSA; Department of Orthopaedic Surgery, Groote Schuur Hospital & Red Cross War Memorial Children's Hospital, Orthopaedic Research Unit, University of Cape Town, South Africa
IIFCOrthSA, MMed(Orth)(UCT), MBBCh(Wits), BSc(Physio); Department of Orthopaedic Surgery, Groote Schuur Hospital & Red Cross War Memorial Children's Hospital, Orthopaedic Research Unit, University of Cape Town, South Africa
IIIOrth; MMed; DA(SA); MBChB; Department of Orthopaedic Surgery, Groote Schuur Hospital & Red Cross War Memorial Children's Hospital, Orthopaedic Research Unit, University of Cape Town, South Africa
IVMBChB, DipPEC, FCOrthSA, MMed(Orth)(UCT); Department of Orthopaedic Surgery, Groote Schuur Hospital & Red Cross War Memorial Children's Hospital, Orthopaedic Research Unit, University of Cape Town, South Africa
VMBChB(UCT), MMed, FCS(SA)Orth; Department of Orthopaedic Surgery, Groote Schuur Hospital & Red Cross War Memorial Children's Hospital, Orthopaedic Research Unit, University of Cape Town, South Africa

As the saying goes, 'the best things in life are free' but this is hardly true for orthopaedic surgery. Theatre nursing scrub staff shortages have led to prolonged turn-around times and resistance to starting cases after 15h00 in our state hospitals. This has negatively impacted productivity with surgical volume reduced by at least 25% on our elective lists this year. With the overwhelming demand due to failing services in some provinces and poor socio-economic factors forcing more patients from private to state care, our elective waiting lists continue to grow.1 This is exacerbated by the massive burden of trauma and infection competing for theatre time.2,3 Although this needs investment in resources to increase state capacity in the long term, short- to medium-term alternative solutions need to be explored. With universal health care (UHC) access and National Health Insurance (NHI) funding models being hot topics,4,5 collaboration with the private sector is a no-brainer. And so, besides a short-term BBEEE compliance, private groups are looking to participate as a survival strategy and align themselves for possible future scenarios. There are many offers but is this the free lunch?
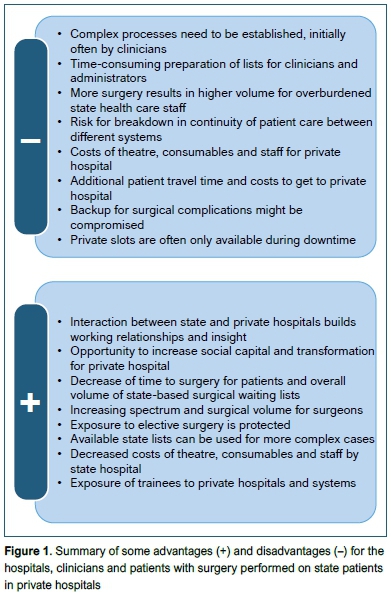
The following editorial is written from a perspective of orthopaedic surgeons which might influence perceptions regarding other stakeholders such as patients, hospital management or auxiliary staff. Our experience of these state-private collaborative initiatives is that of opportunity but also pitfalls (Figure 1). They need to be carefully planned and executed as we describe below.
'We just do the surgery in a different hospital, otherwise everything is the same,' is what we told the first patient on our 'project list'. In reality, complex administrative processes needed to be overcome. Who takes responsibility? Who transports patients? Who provides post-operative pain medication? A formal administrative process is mandatory. It is often not very convenient. Available private lists are usually Friday afternoons or even weekends leading to additional weekend ward rounds - with no interns and registrars for sick certificates and discharge administration. Increased surgical throughput requires increased outpatient clinic capacity with approximately six additional slots needed per case. This needs persuasive discussions with already frustrated clerks, nurses and physiotherapists to accommodate the increased patient load.
Some offers of private surgeons performing the surgery have been made but patient care continuity is a challenge. State surgeons don't want to be reduced to supportive responsibilities without the fun, never mind being left with the complications. Access to clinical notes and imaging across sites, consent and post-operative management communication are problematic and need a clearly established process to ensure safety.
Despite all these challenges, the benefits are massive for the patients and the state health care system. Our year-long waiting list for soft tissue knee procedures quickly shrank to a point where we had to scramble for cases. Patient feedback was positive and for many it was a very comfortable first private hospital experience. By processing straightforward cases of healthier patients on a project list, our state hospital lists were available for more complex cases requiring multidisciplinary peri-operative care and longer post-operative recovery time. Furthermore, the interaction and cross-pollination of state and private health care workers was an incredible experience for both, always amicable and collegial. They felt part of a bigger solution and we enjoyed the golden handrails, automated coffee machines, sparkling clean theatre boots and quick turnaround times. It was a great experience for our trainees and fellows as well, most of whom will work in a private hospital in the future, and (for most) it is worth the extra admin. Admittedly, one of the greatest personal benefits was that we could increase our exposure to a higher volume and spectrum of cases. A monthly full-day list increased our cases by around 50%. Cases were processed more acutely, allowing different treatment approaches and options which directly translated into more surgery and variety in procedures.
In our funding framework, the private hospital covers the theatre time and nursing staff, consumables, possible bed nights and anaesthetic locums. Crutches, braces and implants are provided by the state facility, alongside already employed surgeons. Only day surgery of healthy patients is done. The pre-operative assessment and follow-up are performed at the state facility and patients arrived at the private hospital on the day of surgery.
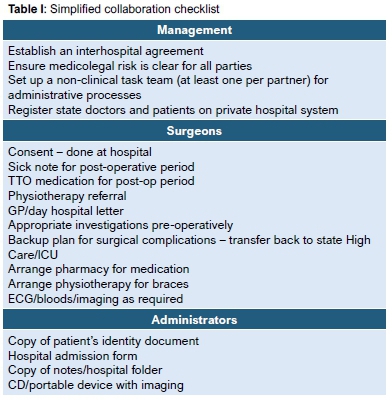
A simplified checklist (Table I) is important to explore when considering such a collaboration.
Regarding equity, there is still a long way to go in the attempt to reduce the great divide between the two sectors. Unfortunately, there is no such thing as a free lunch. All involved require a clear understanding of the costs and benefits to ensure sustainability without the risk of compromise in patient care or overloading individuals involved. We have found it worthwhile - growing a successful relationship between private and public partners with true social value to our patients. Patient outcomes, financial and administrative factors will however dictate viability and longevity.
References
1. Kavalier T, Nortje M, Dunn R. Hip and knee arthroplasty waiting list - how accurate and fair? SAMJ. 2017;107(4):323-26. [ Links ]
2. Beveridge M, Howard A. The burden of orthopaedic disease in developing countries. JBJS. 2004;86(8):1819-22. [ Links ]
3. Dunn R. Musculoskeletal burden of disease: do we have any idea? SA Orthop J. 2012;11(2):20-22. [ Links ]
4. Hofman KJ, McGee S, Chalkidou K, Tantivess S, Culyer AJ. National Health Insurance in South Africa: Relevance of a national priority-setting agency. SAMJ. 2015;105(9):739-40. [ Links ]
5. Mofolo N, Heunis C, Kigozi GN. Towards national health insurance: Alignment of strategic human resources in South Africa. Afr J Prim Health Care Fam Med. 2019;11 (1):7. [ Links ]
 Correspondence:
Correspondence:
Dr M Held
Orthopaedic Research Unit, Division of Orthopaedic Surgery
Groote Schuur Hospital, H49, Old Main Building, 7925 Cape Town, South Africa
Tel: 021 404 5108; Email: michael.held@uct.ac.za
Erratum
The article, 'Antifragile orthopaedic surgeons: a reflection on the training experience' by Dr RG Venter, published in the South African Orthopaedic Journal November 2019 Vol 18 No 4 pp 12-13, had an error on the second page. The sentence starting 'The implication here is that 10 cm of stretching will generate much more strain' should read: 'The implication here is that 10 cm of stretching will generate a lot less strain'. This has been rectified in the online version of the article.

