










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.18 no.4 Centurion Out./Dez. 2019
http://dx.doi.org/10.17159/2309-8309/2019/v18n4a7
CURRENT CONCEPTS REVIEW
Current concepts in the management of open tibia fractures
Manjra MAI; Basson TII; Du Preez GIII; Du Toit JIV; Ferreira NV
IMBBCh, FC Orth (SA), MMed(Orth); Tygerberg Arthroplasty Fellow, Division of Orthopaedic Surgery, Department of Surgical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, 7505, South Africa
IIMBChB, FC Orth (sa); Registrar, Division of Orthopaedic Surgery, Department of Surgical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, 7505, South Africa
IIIMBChB, FC Orth (sa); Consultant and Head of Trauma Unit, Division of Orthopaedic Surgery, Department of Surgical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, 7505, South Africa
IVMBChB, FC Orth (sa), MScClinEpi; Consultant and Head of Department, Division of Orthopaedic Surgery, Department of Surgical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, 7505, South Africa
VBSc, MBChB, FC Orth (SA), MMed (Orth), PhD; Consultant and Head of Tumour, Sepsis and Limb Reconstruction Unit, Division of Orthopaedic Surgery, Department of Surgical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, 7505, South Africa
ABSTRACT
Open tibia fractures are associated with an increased risk of infection, delayed union, non-union and wound complications. Management is aimed at mitigating the risk of infection while optimising the biological and biomechanical environment to encourage soft tissue and bone healing. With ongoing clinical trials and research, our knowledge around best clinical practice continues to evolve. Multiple consensus documents and protocols have been formulated, yet some controversy exists around the ideal management for high risk grade III injuries. Early antibiotic therapy has become a cornerstone in the management of these injuries. However, some controversy remains around the type and duration of antibiotic therapy. Emergent debridement and lavage is a critical factor in treatment success. Intramedullary nailing is a viable fixation option for most open tibia fractures while circular external fixation has gained prominence in the management of high energy grade III injuries, especially in the presence of bone and soft tissue loss. The timing of the various treatment interventions continues to provoke debate and controversy. Considering the available literature, the local context needs to be considered. Inadequate access to theatre, shortage of staff, resources and expertise are frequently encountered. We aim to elucidate current literature with regard to the management of open tibia fractures guided in part by various consensus documents and protocols.
Level of evidence: Level 5
Keywords: open fracture, tibia, debridement, antibiotics, external fixation, internal fixation
Introduction
Tibia fractures are among the most common long bone fractures, occurring at a rate of between 8.1 to 37.0 per 100 000 patients.13 The superficial location of the tibia leaves it particularly susceptible to open fractures and potential loss of soft tissue and bone.4,5 Compared to closed injuries, open fractures have a significantly higher risk of infection, non-union, and wound healing complications, and often require multiple surgeries for definitive care.6
A multidisciplinary approach that includes orthopaedic, trauma and plastic surgeons is frequently required in the management of open fractures. The literature does not provide strong conclusions regarding the best treatment for open tibia fractures; evidence to support best treatment practices for the less prevalent and more devastating 'severe' open fractures is even less conclusive.7 The primary objectives in the management of open tibia fractures include early antibiotic therapy, emergent debridement of all devitalised soft tissue and bone, early soft tissue cover and skeletal stabilisation.2,5 Failure to adhere to these principles may result in significant morbidity, cost and even loss of the injured limb.
The aim of this paper is primarily to review current concepts in the management of open tibia fractures, and secondarily to assess these treatment strategies considering our South African context.
Classification
The most widely used systems in open tibia fractures include the Gustilo-Anderson, Ganga Hospital and the AO (Arbeitsgemeinschaft für Osteosynthesefragen) Orthopaedic Trauma Association Open Fracture Classification (OTA-OFC) systems.8-10
Ramon Gustilo and John Anderson, in 1976, first classified open long bone fractures into grade I to III injuries.11 Subdivision of type III injuries (A-C) was necessitated after they identified the high rate of complications associated with this group.12 This classification system is practical, aids in prognostication and treatment, and is widely implemented in clinical practice and research. However, since the initial description, many modifications have taken place, leading to a loss of uniformity and poor interobserver reliability.10'13,14
Primary assessment
Effective management of open tibia fractures begins in the emergency department. Trauma patients are assessed and managed according to the Advanced Trauma Life Support (ATLS) guidelines, after which attention can be focused on the injured limb during the secondary survey.
Systemic antibiotic therapy
Intravenous antibiotic therapy has been shown to be the single biggest predictor of infection in open tibia fractures.15,16 A Cochrane review by Gosselin reviewing 913 patients confirmed the efficiency of prophylactic antibiotics vs placebo in open fractures, citing a pooled relative risk reduction of 59% for acute infection in patients with open fractures treated with prophylactic antibiotics.17 It was concluded that for every 13 patients treated with prophylactic antibiotics, one acute infection would be circumvented.17 In addition to systemic antibiotics, tetanus prophylaxis should be administered according to local guidelines.
Prophylactic antibiotic therapy should be considered an adjunct to, and not a substitute for, a systematic open fracture management protocol that includes early debridement and irrigation, fracture stabilisation, and wound coverage.18 Nonetheless, prophylactic antibiotics are essential because, in their absence, infection can be expected to occur in 20% of open fractures.19
Sufficient data has concluded that an intravenous antibiotic such as a first- or second-generation cephalosporin (in most cases cefazolin) should be used for antimicrobial prophylaxis.20,21 In patients with beta-lactam allergy, clindamycin is the best alternative.21 The addition of Gram-negative cover (gentamycin) for grade III fractures, and penicillin for fecal or possible clostridial contamination, has been propagated throughout the literature, but is controversial.6,20,22 Gustilo and Mendoza initially suggested the addition of an aminoglycoside, after reporting that up to 77% of infections were a result of Gram-negative bacteria.12 However, Gustilo did not subsequently investigate whether the addition of an aminoglycoside decreased the risk of infection in type III fractures.6 The effectiveness of this strategy was reported in a retrospective study by Patzakis et al., who showed a decreased risk of infection compared with cephalosporin alone; however, several flaws were noted in the study with regard to duration of antibiotic therapy and inconsistencies in the timing of wound closure.6,19
Sufficiently powered trials with large sample sizes are still needed to provide unequivocal guidance on the optimal antibiotic regimen for type III open fractures.23 Considering the available evidence, a combined regimen consisting of an aminoglycoside in conjunction with a first-generation cephalosporin appears to be adopted by most authors and guidelines.23
The Eastern Association for the Surgery of Trauma (EAST) guidelines recommend this combination of a first-generation cephalosporin plus an aminoglycoside, with the addition of penicillin to prevent clostridium infection in farmyard injuries.6,24 Carver et al. in a 2017 review further suggested that a third-generation cephalosporin (ceftriaxone) or piperacillin/tazobactam as a good alternative to the above combination, although further research is still required.21
The AO and BOA/BAPRAS standards for trauma (BOAST4) guidelines are currently the most implemented guidelines on which management is based. The current AO guidelines for antibiotic prophylaxis in open fractures are as follows:9
• Type I and II: 24 hours, first- or second-generation cephalosporin
• Type III: five days amoxicillin/clavulanic acid or ampicillin sulbactam or five days third-generation cephalosporin
• In the case of fecal contamination (farmyard injury or open pelvic fracture) use piperacillin/tazobactam or a carbapenem or third-generation cephalosporin plus metronidazole
The current BOAST4 guidelines are as follows:25,26
1. Co-amoxiclav 1.2 g eight-hourly or a cephalosporin such as cefuroxime 1.5 g eight-hourly IV as soon after the injury as possible and continued until debridement
2. Co-amoxiclav/cephalosporin and gentamicin 1.5 mg/kg at the time of debridement and co-amoxiclav/cephalosporin continued until definitive soft tissue closure, or for a maximum of 72 hours, whichever is sooner
3. Gentamicin 1.4 mg/kg and either vancomycin 1 g or teicoplanin 800 mg on induction of anaesthesia at the time of skeletal stabilisation and definitive soft tissue closure. These should not be continued post-operatively. The vancomycin infusion should be started at least 90 minutes prior to surgery.
For patients with penicillin allergy, clindamycin can be given in place of co-amoxiclav/cephalosporin.
Since the landmark paper by Patzakis and Wilkins et al., studies have consistently shown an association between delay of intravenous antibiotic administration and an increased risk of infection.1,16,27 In their case-control study of more than 1 100 open fractures, administration of antibiotics more than three hours after injury was associated with a 1.63 times greater odds of infection in comparison with treatment within the first three hours after injury.16 The risk of infection increases significantly beyond this period due to changes in circulation and multiplication of bacteria.27 However, limitations of this study include antibiotic timing that was not examined against the grade of injury, the evolved and advanced nature of our modern trauma systems, and only 36% patients receiving antibiotics within three hours.
A more recent retrospective study by Lack et al. examining the relationship between antibiotic timing and deep infection in grade III open tibia fracture put forward a stronger case for antibiotic timing.28 They found that wound coverage beyond Ave days and antibiotics beyond 66 minutes independently predicted infection. Immediate antibiotics and early coverage limited the infection rate relative to delay in either factor or delay in both factors. Age, smoking, diabetes, injury severity score, grade IIIA versus IIIB/C injury, and time to surgical debridement were not associated with infection.
Routine antibiotic therapy beyond the initial post-operative period is not beneficial in any open fracture.15 A prospective randomised controlled trial by Dellinger et al. examining the relationship between timing and duration of antibiotic therapy with infection, concluded that on presentation to the emergency department, one-day antibiotic administration is equally efficacious as five-day administration in preventing infections.29 Antibiotics should be discontinued 24 hours after wound closure in grade I and II fractures, and continued for 72 hours following grade III fractures - but not more than 24 hours after tissue coverage of the open wound.15,20
With increasing use of antibiotics in the general population, we are faced with a new concern that was probably not present in clinical trials from prior decades, namely antibiotic resistance.18 Among four level I trials studying antibiotic prophylaxis in open fractures, all highlighted a prevalence of Staphylococcus aureus as the number one cause of surgical site infection, and one reported the rate of methicillin-resistant S aureus (MRSA) as being nearly one-third of the total staphylococcal infections.27,30-32 Vancomycin may be appropriate for first-line treatment if the patient has a significant, documented beta-lactam allergy, has a history of MRSA colonisation, or is hospitalised in an area with recent MRSA outbreaks.22 Clinicians should also be cognisant of the associated risk for selection of resistant organisms such as MRSA that are associated with cephalosporins, particularly in patients who may require prolonged hospitalisation.33 Fluoroquinolones offer no advantages compared with a combination of cephalosporin and gentamicin and may actually have a detrimental effect on fracture healing and increase the infection rate in type III fractures.24
Wound cultures
Wound cultures obtained at debridement immediately post injury must not be used to direct choice of agent for antimicrobial prophylaxis, as the infecting pathogens do not typically correlate to pathogens initially cultured after injury.15,20 Most infections from open fracture wounds result from nosocomial organisms.32,34 In contrast, while pre-debridement cultures are not recommended, post-debridement cultures may be useful.6 Positive cultures at time of closure do not predict the infecting organism but correlate with the development of infection.32 This has led to some units adopting the practice of performing post-debridement cultures in delayed cases (>24 hours).6
Local antibiotic therapy
Local antibiotic-laden polymethylmethacrylate beads (APB) have been shown to produce high antibiotic concentrations at the wound site in open tibia fractures while minimising systemic exposure, thus decreasing the risk of systemic adverse effects.35 In addition to providing a high dose of local antibiotics to the area of highest risk, which may not be well perfused or reached by systemic antibiotics, they serve to eliminate potential dead space.36 Local antibiotic therapy cannot replace the use of intravenous therapy but may be a useful adjunct in severe injuries where the tissues are not amenable to immediate closure.35
Osterman et al. in the largest series of 1 085 patients on APB efficacy in open tibia fractures, demonstrated a significant decrease in the rates of acute and chronic osteomyelitis with the use of tobramycin-impregnated cement beads in conjunction with systemic antibiotics in the management of grade III fractures (infection rate, 6.5% versus 20.6%, respectively; p=0.001); but the same benefit was not demonstrated in lower grade injuries.37 However, the decision to use APB was not randomised and was rather a matter of surgeon preference or bead availability. Secondly, soft tissue management differed between the groups, with patients receiving APB having their wounds closed earlier than the control group.
Keating et al. and Moehring et al. did not find a statistical difference comparing systemic versus local antibiotic therapy; however, there are limitations in both studies.38,39 A recent meta-analysis by Craig et al. of 21 studies demonstrated a significantly lower deep-infection risk with use of local antibiotic administration as an adjunct to systemic antibiotics across all types of open tibia fractures treated with intramedullary nailing.40 The effect was most pronounced for type III injuries, in keeping with Osterman's findings, which demonstrated a pooled infection risk of 2.4% (95% CI: 0.0% to 9.4%) with an adjunct local antibiotic as compared with 14.4% (95% CI: 10.5% to 18.5%) with systemic prophylaxis alone (odds ratio, 0.17; p value not reported).23,40
The skin should ideally be closed over the beads which can be removed on the second or third day post-surgery without a second operation, if threaded through the incision on insertion.36 Wahlig and Dingeldein showed that the highest concentration of elution from the gentamicin beads takes place in the first several days after implantation, with detectable levels still present at day 80.41 These elution characteristics are ideal for short-term use in open fractures.36 The use of negative pressure wound therapy (NPWT) in conjunction with antibiotic beads has been reported, but there is a concern that negative pressure reduces antibiotic concentration at the wound site.42,43
Bioabsorbable mediums which have recently been investigated include calcium sulfate, polycaprolactone (PCL), collagen sponges and gels.36 These mediums have the advantage of not requiring removal; however, they present a significant problem if the development of infection necessitates their removal.36 Since bioabsorbable beads require cellular activity to degrade the implants, when there is a recurrence of infection the absorption process stops, and the beads simply float in the purulence.36
Learning points
• Administer intravenous antibiotic therapy as soon as possible according to local guidelines.
• Be aware of local antibiotic resistance patterns.
• Local antibiotic beads are a useful and effective adjunct to intravenous therapy.
• Wound cultures are not useful in acute injuries.
Surgical principles
Debridement
The quality of the initial debridement represents a key point in the treatment of open fractures and infection prevention.44 The technique of debridement of open fractures is guided in part from the BOA/BAPRAS working party on the management of open tibia fractures.18,45 This step-by-step protocol for removal of all dead tissue at the initial debridement is followed nationwide across the United Kingdom. Systematic debridement occurs in the following sequence:
1. Initial cleaning of the limb with a soapy solution
2. Preparation of the limb with a chlorhexidine alcohol solution, avoiding direct contact of the chlorhexidine with the open wound
3. Wound extension, ideally following potential fasciotomy incisions
4. Systematic assessment of the tissues, from superficial to deep, and from the periphery to the centre of the wound
Radical excision of necrotic tissue, as proposed by Godina, should be performed so that all nonviable tissue, including bone, is removed.46,47 Muscle viability is assessed using the four Cs:
Colour, Consistency, Contractility and Capacity to bleed. It is important to note that an inflated tourniquet might interfere with this assessment. A tourniquet should be applied but only inflated when required. Loose bone fragments are assessed via the tug test and all segments with no bleeding edges, or loose fragments without attachment to soft tissue, should be removed.18 This is then followed by wound lavage. At this juncture an accurate assessment of the grade of injury can be made.
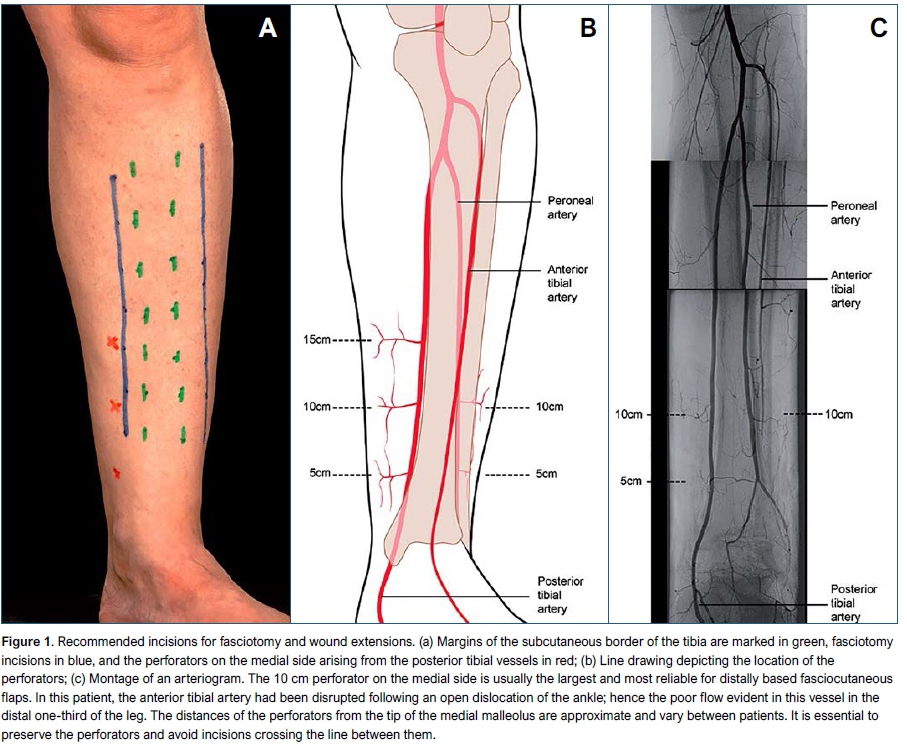
BOA/BAPRAS guidelines recommend longitudinal wound extensions for debridement along fasciotomy incisions to preserve the longitudinal running neurovascular structures and perforating arteries medially and laterally that form the basis of local flap reconstructive options in the leg (Figure 1).25,45Conversely, Salih et al. recently published a case series of 31 patients with open tibia fractures which were treated with acute bony debridement and shortening with a transverse wound extension that enabled tension-free soft tissue coverage, and either primary closure or split skin grafting.48 Fracture stabilisation was usually obtained with a monolateral external fixator and converted to a circular Ilizarov frame that then allowed correction of leg length discrepancy or deformity. The reasoning given for choosing a transverse incision was a wound that could be closed more easily (than the rhomboid wounds created by longitudinal incisions) with the avoidance of soft tissue flaps and associated complications. All but one patient achieved bony union with the initial circular fixator, and all wounds were closed either primarily or with a split thickness graft. The decision to perform a transverse incision was done on a case-by-case basis in conjunction with the plastic surgical team. Factors that were considered to guide the decision included: a transverse wound, a wound not amenable to local flap coverage, a high-energy injury with bone loss that would result in shortening, and a patient who would be unsuitable for a free flap. Hence this option should not be the standard of care, but rather an option for carefully selected patients.
Also contrary to the BOA/BAPRAS guidelines is the technique described by Marecek et al. When extension of the traumatic wound may compromise the soft-tissue envelope and necessitate a rotational or free tissue transfer, they suggest that debridement may instead be performed through a 'defined surgical approach', distant to the traumatic wound.49 In this technique an anterolateral or posteromedial surgical approach is used to visualise the zone of injury and perform debridement. They compared 47 patients who had direct extension of the traumatic wound with 21 patients who were debrided using an anterolateral approach. The decision on what approach to use was at the discretion of the consultant surgeon, and the groups had similar proportions of Gustilo-Anderson grades. The average number of surgeries, including index procedure, per patient was 1.96 in the direct extension group and 1.29 in the defined approach group (p=0.026). Flap coverage was needed in nine patients in the direct extension group and no patients in the defined approach group (p=0.048). However, the authors noted the absence of grade IIIB injuries in the defined surgical approach group. It was unclear if any patients successfully avoided a flap based on the choice of approach for debridement.
Timing of debridement
The timing of debridement has been the subject of many studies. It was initially advocated that the surgical debridement should not be delayed for more than six hours. This 'six-hour rule' is believed to originate from a rodent study in the pre-antibiotic era.50 In 1989 Patzakis et al. found that the time to antibiotic prophylaxis was more important than time to surgical debridement.16 This has been corroborated by many authors, with the most recent stating that, due to the risk associated with after-hours surgery, the debridement of open fractures can be safely postponed to an urgent elective theatre slate without increasing the risk of infection.255051
When the primary debridement was done by an experienced surgical team, the outcomes were also found to be better.51-53 Steeby et al. confirmed this when they compared the outcome of open tibia fractures managed during daylight hours in a dedicated orthopaedic operating room (DOTOR) versus being managed on an urgent basis in an on-call operating theatre (OCOR). Although they found similar infection rates, the DOTOR group had fewer unplanned surgeries and an uncomplicated fracture union.54 The BOAST4 guidelines state that:45
• Surgery to achieve debridement, fixation and cover of open fractures of the long bone, hindfoot or midfoot should be performed concurrently by consultants in orthopaedic and plastic surgery (a combined orthoplastic approach).
• Perform debridement:
▫ immediately for highly contaminated open fractures
▫ within 12 hours of injury for high-energy open fractures (likely Gustilo-Anderson classification type IIIA or type IIIB) that are not highly contaminated
▫ within 24 hours of injury for all other open fractures.
Lavage
Wound irrigation as an adjuvant to surgical debridement is essential to minimise infection.7,8,23,55 The ideal composition and irrigation pressure have been long been the subject of controversy.23,55-63 High pressure may be more effective in removing particulate matter and bacteria, but at the expense of bone damage.58-62 Low pressure may avoid bone damage and resultant delays in bone healing but is thought to be less effective at removal of foreign bodies and bacteria.64
The Fluid Lavage in Open Wounds (FLOW) trial, a multicentre randomised trial examining the effect of normal saline vs castor soap and high (15-35 psi or higher) vs low pressure (5-10 psi) lavage vs very low pressure (1 or 2 psi) in open fractures, has shed light on previously held notions on the delivery and composition of the ideal lavage solution.64 It is important to note that the study included open fractures of all extremities defined as arm, wrist, leg, ankle, foot, clavicle or scapula, with the exclusion of the pelvic ring, axial skeleton and hand.64 The primary endpoint was reoperation after 12 months from the index surgery for promotion of bone healing and wound infection.64 The reasons cited for the decision to use soap as opposed to other enhanced irrigation solutions (containing antiseptics or antibiotic agents) include: less cost, toxicity and risk of antibiotic resistance.7'8'23'55-58'6566 No significant differences were found in the rates of secondary end points (non-operatively managed infection, wound-healing problem or bone-healing problem) between the two irrigation solutions or among the three irrigation pressures. However, castor soap did demonstrate a significantly higher incidence of reoperation.64 Subgroup analysis of open tibia fractures suggested that very low pressure was superior to low or high pressure.64 Given our context of budget constraints and sometimes scarce resources in peripheral government centres, low pressure saline is an acceptable and cost-effective solution.
Wound closure
Primary wound coverage has been considered critical to achieving favourable outcomes.53,67 Wounds that can be closed primarily should be closed.18 However, some studies have suggested that delayed wound closure with the use of NPWT also results in favourable outcomes.68,69 Delayed wound closure is believed by some authors to reduce the risk of deep infection.70,71 Russel et al. reported that early wound closure may result in pathogenic organisms remaining encased in the wound, hence increasing the risk of infection, and suggested there is no place for primary wound closure in open tibia fractures.72 This is supported by data from military injuries, where authors suggest that the wound should initially be left open, serial debridements performed as needed, and the wound closed after it is deemed clean.73 This notion has been challenged by more recent literature which suggests that pathogenic organisms were secondarily acquired via nosocomial routes.74,75 This is supported by studies which showed a poor correlation between organisms cultured at initial debridement and resultant infecting pathogens.15,20 Furthermore, advances in the field of wound care, antibiotic therapy as well as internal fixation have vastly improved infection rates, challenging earlier studies examining the early in vitro response of bacteria to metals.67,73,76
It is generally accepted that grade I and II open fracture wounds can be safely closed after initial debridement, provided the patient received adequate antibiotic prophylaxis. There is no concern about ongoing tissue necrosis or contamination, and that a tension-free closure of the soft tissues can be achieved.6,23 However, controversy exists regarding the optimal closure or coverage of grade III open fracture wounds.
Rajesakeran et al. published a prospective series of 173 patients with grade IIIA and IIIB open tibia fractures treated with primary closure. They reported 'excellent' results in 87% of patients assessed by bony union, wound healing with no marginal necrosis and absence of infection at Ave years.77 Strict criteria for closure required included: no skin loss, debridement within 12 hours of injury, stable skeletal fixation during primary surgery, skin apposition without tension, and no sewage or organic contamination.23,77
For wounds requiring flap coverage, location of the injury, size of the defect, and zone of injury must collectively be assessed to determine if rotational or free-flap coverage is optimal.23 Generally, wounds in the proximal two-thirds of the tibia can be adequately managed with rotational gastrocnemius and/or soleus flaps, while fractures of the distal third require free muscle or fasciocutaneous flaps.78
Learning points
• Debridement should be done on an emergent basis.
• While it is preferable for debridement to be done by an experienced team, this is not always possible in public hospitals where these cases need to be done as theatre becomes available.
• Low pressure saline is acceptable and cost effective as a lavage solution.
• Primary wound closure should be performed where this can be done safely.
The role of NPWT/VAC
Negative pressure wound therapy (NPWT) or vacuum-assisted closure (VAC) should be seen as an adjunctive modality in the management of the soft tissue component of open tibia fractures. It involves the application of subatmospheric pressure to a wound via a sealed sponge or foam dressing, removing fluid and exudate, and encouraging blood flow to the wound site.6,18,79 This environment decreases tissue bacterial levels, increases tissue perfusion and rapidly promotes granulation tissue formation, thus improving wound healing.79-81 In cases of immediate closure, these conditions promote wound healing, and in cases of delayed closure, the promotion of granulation tissue formation prepares the wound bed for subsequent coverage and may reduce the need for soft tissue transfer and muscle flaps.67,82 They have been shown to effectively reduce bacterial counts in wounds until definitive soft tissue coverage.81,83
The utility of NPWT in orthopaedic surgery has seen an increase in recent years, particularly in the management of infection and open fractures.18,84 After open fractures specifically, NPWT is commonly used as a temporary dressing between operative interventions. In a prospective, randomised study, Stannard et al. examined infection rates in 62 patients with open fractures who received soft tissue management with either NPWT or standard gauze dressings between the initial debridement and definitive soft tissue closure.80 They found a significantly decreased infection rate (28% vs 5.4%; p=0.02) in favour of the NPWT. More recently, Blum et al. reported similar results: 20% infection in the standard dressing group and 8% in the NPWT group.85 As expected, the open fracture grade correlated with the infection rate.
Caution should however be raised against the use of NPWT as a definitive soft tissue management strategy. A 2011 international expert panel attempted to provide consensus statements regarding the use of NPWT in traumatic wounds and reconstructive surgery.86 A 98% agreement was obtained for a recommendation on the use of NPWT for soft tissue trauma. In this regard the panel recommended that 'NPWT may be used when primary closure is not possible after or in between debridements as a bridge to definitive closure'.86
Skeletal stabilisation
Stabilisation of open fractures restores length, alignment and rotation, protecting the soft tissues around the zone of injury from further damage, and decreases dead space.87 These factors have been shown to decrease the rate of infection in multiple studies.88-90 Early fixation allows improved access to soft tissues surrounding the injury and facilitates the patient's early return to normal function.8
The choice of fixation depends on the fracture location (intra-articular, metaphyseal, diaphyseal), the extent of the soft tissue injury, and the degree of contamination and physiologic status of the patient.46
Intramedullary nails dominate the most commonly used fixation method following open tibia shaft fractures and are associated with low overall infection rates, high union rates, and high levels of patient satisfaction.4 Intramedullary nails remain the fixation method of choice for Gustilo-Anderson I to IIIA open injuries, but utilisation of these devices in Gustilo-Anderson IIIB injuries are coming under increased scrutiny and is the topic of multiple ongoing trials.7,70,91-94
Temporary external fixation plays an important role in the acute management of severely contaminated open tibia fractures.23 This is usually in the form of monolateral external fixation providing stability to the fracture, while allowing resuscitation of the soft tissues, and in the case of the multiply injured polytrauma patient, stabilisation of the patient's physiological state before more extensive reconstructive surgery
Bhandari et al. conducted a systemic review of tibial and femoral fractures converted to intramedullary nailing following external fixation. They found a significant relative risk reduction for infection if conversion was done in less than 14 days, and that lack of pin-site infections was the most important factor in prevention of infections.95 Other key factors in this scenario cited by Yokoyama et al. include: flap coverage by well-vascularised tissue within one week after trauma; short duration of external fixation; debridement of the screw hole at the pin site; early unreamed intramedullary nailing; and slightly prolonged interval between removal of the external fixator and intramedullary nailing until complete healing of the pin site.96
Circular external fixation has demonstrated its effectiveness in the management of complex open tibia fractures in both civilian and war injuries.97-100 They utilise indirect reduction techniques with fine wires and/or half pins and small incisions, which ensure minimal soft-tissue damage and soft-tissue footprint.4 Treatment with circular external fixation, which does not place any hardware at the fracture site, may reduce infections and hospital readmissions.101
Circular external fixators consist of two distinct systems: the original Ilizarov technique and hexapod systems. Limited literature regarding the use of hexapod external fixation in open tibia fractures shows promising results, suggesting that the hexapod design can play a significant role in managing complex tibia fractures.102,103
Dickson et al. recently reported on the surgical and functional outcome of 22 patients with grade III open tibia fractures treated with circular external fixation at a minimum one-year follow-up.4 Clinical scores were either good or excellent in over half of the patients in all knee and ankle scores, with good functional outcome in most cases. All fractures united without further surgery, and no refractures. The deep infection rate was low at 4.5%, adding to the growing body of evidence for managing these complex injuries with a circular frame.
Nieuwoudt et al. reported excellent short-term results with low infection and non-union rates on 94 consecutive grade III open tibia fractures treated with circular external fixation followed up for a period of 12 months.100 The majority of patients were treated in traditional Ilizarov fixators. Hexapod external fixators were used in 12 patients. Deep infection developed in four out of 94 (4.25%) cases. Two patients united in the presence of sepsis and two developed infected non-unions. There was no statistically significant difference between infection rates in grade IIIA and IIIB injuries (p=0.617). Two of the four deep infections occurred in HIV-positive individuals. There was no statistically significant association between HIV status and the development of deep infection (p=0.601). No superficial infection cases were reported. Non-union occurred in three out of 94 (3.2%) patients, all with grade IIIB injuries.
Circular external fixation is especially useful in the setting of significant segmental bone loss, where the defect can be managed with Ilizarov bone transport.53 The Ilizarov bone transport technique, known as distraction osteogenesis for restoration of limb length, is well described in the literature.48,104-107 Advocates of this technique use it to treat large bone defects by creating an osteotomy at a site away from the fracture and transporting the existing bone into the defect.91 New bone forms at the osteotomy site, thus maintaining the length of the limb and avoiding bone grafting procedures.91
Hutson et al. reviewed 19 grade IIIB injuries treated with a protocol of multiple aggressive debridements followed by soft tissue reconstruction with rotational or free flaps, utilising monolateral half-pin external fixation.98 Bone loss was managed with a temporary antibiotic spacer, followed by definitive fixation and bone transport with Ilizarov circular external fixation. Flap coverage was achieved on an average of 34 (range 12-77) days, and the Ilizarov fixator was applied at an average of 23 (range 2-43) weeks post injury. There were no cases of non-union, infection or failed treatment with internal fixation. Similarly, Hohmann et al. reported good outcomes using a staged 'Road to Union' protocol in their management of complex and acute complex tibial fractures.108
A modification of this technique, which is well described by multiple authors, is the intentional shortening and/or deformation of the limb to achieve bony apposition as well soft tissue closure, decreasing or negating the need for soft tissue flaps.48,104,105,109,110 The length and/or deformity is then gradually corrected utilising either conventional Ilizarov external fixation or hexapod external fixation. In most cases shortening is achieved after bony debridement of devitalised bone; however, the decision can be made to excise healthy bone to achieve soft tissue apposition and negate the need for a soft tissue flap, as described in the case series by Nho et al.104
Internal fixation vs external fixation
Intramedullary nailing (IMN) and external fixation currently represent the most widely used methods of fixation after open fractures, with the use of plate fixation declining since the 1970s.111 Giovannini et al. performed a meta-analysis of five randomised controlled trials comparing intramedullary nailing with external fixation in the management of open tibia fractures.111 The authors concluded that IMN was more effective due to the lower rate of infection; however, the results of this analysis should be treated with caution as only five studies that included less than 250 patients were reviewed, monolateral and circular fixators were grouped together, and the description of fracture subtypes and complications was not uniform.
Bhandari et al. conducted a systemic review and meta-analysis on the treatment of open tibia fractures comparing various methods of skeletal fixation: plate fixation, external fixators, unreamed tibial nails and reamed tibial nails.70 They concluded that their study provided 'compelling evidence' that unreamed nails reduced the incidence of reoperations, superficial infections and malunions, when compared with external fixators. However, no mention was made of whether monolateral or circular external fixation was used, limiting the applicability of this evidence. It is well reported in the literature that monolateral external fixation results in a significantly higher rate of delayed union in open tibia fractures.92
Foote et al. conducted a network meta-analysis using evidence from randomised trials, on the risk of unplanned reoperation of open fractures of the tibial diaphysis treated with various stabilisation devices.7 The secondary study endpoints included malunion, deep infection and superficial infection. They found that unreamed nail fixation was associated with a lower risk of reoperation compared with external fixation, and this was independent of the Gustilo classification of the fracture. No conclusions could be drawn with regard to secondary endpoints. They noted that limitations of the 14 studies included a high risk of bias and poor precision in the conduct of the studies.
Inan et al. conducted a prospective study comparing unreamed tibial nailing (UTN) with Ilizarov external fixation in patients with grade IIIA tibial fractures.92 Their results showed that the Ilizarov technique had a notable incidence of pin-site infection, joint contracture and shortening related to delayed union. The UTN technique had the disadvantage of post-traumatic osteomyelitis and delayed union requiring additional surgery. The rate of union of Ilizarov circular external fixation was similar to that of unreamed tibial nails. No further conclusion could be drawn with regard to which modality was superior. It is important to note that the type of tibial nail used in the study was not standardised, and that all the nails used were solid nails.
The LEAP study group has been fundamental in expanding our understanding of the surgical and functional outcomes of open and closed tibia fractures. They reported a significantly higher rate of non-union and infection with external fixation compared to unreamed tibial nails, leading to unreamed tibial nails becoming the 'gold standard' for open tibia fractures.93 However, the LEAP study (similar to other studies mentioned previously) only included monolateral external fixators, which have very different biomechanical properties, and therefore different outcomes to circular frames.4 An important systematic review of the literature conducted by Dickson et al. revealed that circular frames have higher union rates, and lower deep infection and reoperation rates, compared to other treatment modalities in open tibia fractures.4
At the recent International Consensus Meeting for Musculoskeletal Infections. a consensus statement regarding the optimal fixation method for open tibia fractures in terms of infection was released and stated that: 'There is little to no difference in terms of infection rates for Gustilo-Anderson type I-II treated with either circular external fixator, unreamed intramedullary nail or reamed intramedullary nail. For Gustilo-Anderson IIIA-B fractures, circular external fixation appears to provide the lowest infection rates when compared to all other fixation methods'.94 This statement achieved the strongest consensus and was unanimously accepted by all attending delegates.94
To date no randomised control trial has been undertaken to compare circular external fixation with internal fixation in the management of these injuries. The Modern Ring External Fixators Versus Internal Fixation (FIXIT) Study, is a prospective multicentre randomised control trial which will compare one-year outcomes after treatment of severe open tibia shaft fractures with modern external ring fixation versus internal fixation among men and women of ages 18-64 years.91 The primary outcome is rehospitalisation for major limb complications. Secondary outcomes include infection, fracture healing, limb function, and patient-reported outcomes including physical function and pain. One-year treatment costs and patient satisfaction will be compared between the two groups, and the percentage of Gustilo IIIB fractures that can be salvaged without soft tissue flap among patients receiving external fixation will be estimated. The results of this study will shed further light on the preferred management of open tibia fractures.
Timing of soft tissue management and definitive fixation
Although many authors tend to study these two treatment modalities in isolation, they are intricately entwined and should be seen as a single treatment entity. In the lower grade injuries, both these steps can and should be completed at the initial debridement. With higher-grade injuries, these modalities cannot be completed at initial debridement and temporary fixation with soft tissue dressings is utilised. These include monolateral external fixation and NPWT.
The current BOAST4 guidelines stipulate soft tissue closure within 72 hours and definitive fixation only when it can be followed immediately by soft tissue closure.45 This was based on the evidence report of the National Institute of Health and Care Excellence (NICE).26 The literature used in this report to determine the timing of soft tissue cover and fracture stabilisation is, by their own admission, of very low quality. The main driver for their recommendation of early reconstruction was the theoretical reduction in hospital-acquired infections and tissue necrosis induced by prolonged wound exposure.69
The earliest proponent of this early (<3 days) definitive soft tissue closure was Godina in his landmark study.47 He achieved an infection rate of 1.5% in a group of 134 patients where soft tissue reconstruction was achieved in less than 72 hours. Other supporters of soft tissue reconstruction within 72 hours include Hertel et al., Gopal et al. and Naique et al. with their 'fix and flap' protocol.51,53,69
Other authors supported a more conservative approach where definitive soft tissue management can be delayed up to seven days after injury without adverse effects. Cierny et al. compared infection rates in type III injuries that had wound closure before or after seven days.112 They reported rates of 4% and 50% respectively. Similar findings were also made by Caudle and Fischer et al.113,114Reporting on patients from the LEAP study, Webb et al. and Pollak et al. found no difference in infection rate patients with wound coverage less than three, four to seven or greater than seven days; however, there was a 32% incidence in flap complications in wounds covered after seven days.93,115 This finding was complemented by a study by D'Alleyrand et al. who reported that the complication rate increased by 11% per day, and the infection risk by 16% per day after seven days, even after controlling for known risk factors for complications (such as injury severity), in patients treated with flap coverage for grade IIIB open tibia fractures.101
In their study, Mathews et al. made the same observation and directly commented on the BOAST4 guideline of completing the definitive management within 72 hours post injury.116 They found much improved rates of deep infection where definitive soft tissue and skeletal management was completed at the same surgical setting rather than both being completed within the 72-hour guideline (4.2% vs 34.6%).
Learning points
• Grade I, II and IIIA injuries can be safely treated with reamed or unreamed intramedullary nailing.
• Grade III (B and C) injuries should rather be treated with circular external fixation to mitigate the risk of infection.
• Circular external fixators can be used to aid in soft tissue cover/ healing to avoid the use of soft tissue flaps.
• Temporary external fixation when used should be limited to less than 14 days.
• Aim to obtain soft tissue cover within seven days.
South African context: issues to consider
Results and recommendations from international studies need to be adapted to our local context. Orthopaedic units within public hospitals manage a large trauma burden. This, in conjunction with a constrained resource pool, does not always lend itself to the ideal management pathway for open tibia fractures.
Despite literature indicating that emergency theatre debridement is not needed, limited resources often prevent patients from receiving their first debridement within 24 hours of their injury. Because of this, patients must utilise theatre when it becomes available. This means that open fracture debridement sometimes happens after hours, by an inexperienced surgeon. Due to an even greater shortage of plastic surgeons in South Africa, orthoplastics units dedicated to the management of musculoskeletal injuries, do not exist.
South Africa has one of the highest prevalence of HIV infection in the world. HIV infection causes a decline in the CD4 (T helper cell) count, resulting in impaired immunity, hence one would expect to see a higher rate of infection in HIV-positive patients.117 Harrison et al. conducted three studies relevant to this topic: a prospective study of open tibia fractures comparing HIV-positive and -negative patients; a prospective study of internal fracture fixation including cases in open fractures comparing wound infection for HIV-positive and -negative patients; and a prospective study of pin-tract sepsis comparing HIV-positive and -negative patients.117,118 They found that rates of infection were higher in HIV-positive patients; internal fixation of open tibias was associated with a higher risk of infection; HIV was associated with delayed union; and that HIV-positive patients had a higher rate of pin-tract sepsis with the use of external fixation.118 However, there are a number of factors limiting the validity of their findings: the presence of confounding factors such as smoking, nutrition, small patient number in all the studies and, probably most importantly, CD4 count.
These studies were undertaken long before the advent of antiretroviral therapy, and it is plausible that an HIV-infected patient with a normal CD4 may be treated as immune competent.118 Recent evidence indicates there is no association between HIV status and surgical outcome unless the CD4 count is below 350 cells/ml.119-122 It is therefore suggested that HIV status should not influence the management of open tibia fractures.120
Patient demographics, and specifically home circumstances, are important factors to consider especially when deciding the optimal form of skeletal fixation. Patients with poor socioeconomic circumstances may not be able to cope with labour-intensive circular fixators or may not be able to return timeously for follow-up. A peculiar circumstance is patients not being able to access public transport either logistically from not being able to fit into a crowded taxi, or not being allowed onto a taxi due to misunderstanding and the stigma associated with the fixator. This can be overcome by prolonged inpatient stays; however, this contributes to overcrowded public hospital wards and rising inpatient expenses.
In the private sector, surgeons working in remote areas may not have immediate access to the same devices and implants as central areas, or may not deal with a sufficient volume of cases to be familiar with them. The availability of plastic surgical cover in these areas, as in the public sector, is also variable. Devices available to surgeons in the private sector may also be governed in part by funders/medical aids.
Conclusion
Open tibia fractures remain challenging injuries to treat. Early intravenous antibiotic therapy continues to be one of the most important modifiable risk factors for infection. Local antibiotic beads are an effective adjunct, particularly in grade III injuries. The importance of a thorough and meticulous debridement cannot be overstated. While the traditional method of longitudinal extension of the traumatic wound along fasciotomy lines remains standard practice, the use of a transverse incision or a defined surgical approach can be equally effective in select cases. Costly high-pressure lavage modalities have no benefit over low-cost irrigation with saline and should be avoided, especially in the context of a cost-conscious public health system. Soft tissue closure should not be unnecessarily delayed if the soft tissues are amenable. Definitive soft tissue coverage should aim to be completed within seven days of injury. Negative pressure wound dressings are a valuable adjunct in soft tissue management prior to definitive wound coverage. While IMN is effective in grade I and II injuries, strong consideration should be given to the use of circular external fixation in high energy grade III injuries, especially in the setting of bone and soft tissue loss.
While awareness of the best clinical practice and protocols is essential, adaptation to the local context is equally important. Large trauma loads, coupled with constrained resources and personnel, often make internationally accepted time frames for treatment unrealistic. Public hospitals are forced to utilise theatre time at whatever time it becomes available. Fixation devices need to be adapted to these possibly delayed treatment time frames as well as to patient demographics, and cultural and socioeconomic circumstances.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore, 2010.
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Ethical approval for this study was not obtained - review article.
Declarations
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
ORCID
Μ Manjra http://orcid.org/0000-0002-4411-5921
Τ Basson http://orcid.org/0000-0003-1686-9862
G du Preez http://orcid.org/0000-0003-2760-7307
J du Toit http://orcid.oro/0000-0002-0958-5450
Ν Ferreira http://orcid.org/0000-0002-0567-3373
References
1. Court-Brown CM, McBirnie J. The epidemiology of tibial fractures. J Bone Joint Surg Br. 1995;77(3):417-21. [ Links ]
2. Wani N, Baba A, Kangoo K, Mir M. Role of early Ilizarov ring fixator in the definitive management of type II, IIIA and IIIB open tibial shaft fractures. Int Orthop. 2011;35(6):915-23. [ Links ]
3. Larsen P, Elsoe R, Hansen SH, Graven-Nielsen T, Laessoe U, Rasmussen S. Incidence and epidemiology of tibial shaft fractures. Injury. 2015;46(4):746-50. [ Links ]
4. Dickson DR, Moulder E, Hadland Y, Giannoudis PV, Sharma HK. Grade 3 open tibial shaft fractures treated with a circular frame, functional outcome and systematic review of literature. Injury. 2015;46(4):751-58. [ Links ]
5. Hutchinson AJ, Frampton AE, Bhattacharya R. Operative fixation for complex tibial fractures. Ann R Coll Surg Engl. 2012;94(1):34-38. [ Links ]
6. Ryan SP, Pugliano V. Controversies in initial management of open fractures. Scand J Surg. 2014;103(2):132-37. [ Links ]
7. Foote CJ, Guyatt GH, Vignesh KN, Mundi R, Chaudhry H, Heels-Ansdell D, et al. Which surgical treatment for open tibial shaft fractures results in the fewest reoperations? A network meta-analysis. Clin Orthop Relat Res. 2015;473(7):2179-92. [ Links ]
8. Gustilo RB, Merkow RL, Templeman D. The management of open fractures. J Bone Joint Surg Am. 1990;72(2):299-304. [ Links ]
9. Ruedi TP, Buckley RE, Moran CG. AO principles of fracture management. 2nd expanded ed. [edited by] Thomas P Rüedi, Richard E Buckley, Christopher G Moran. ed. Davos Platz, [Switzerland]: AO Pub.; 2007. [ Links ]
10. Rajasekaran S, Naresh Babu J, Dheenadhayalan J, Shetty AP, Sundararajan SR, Kumar M, et al. A score for predicting salvage and outcome in Gustilo type-IIIA and type-IIIB open tibial fractures. J Bone Joint Surg Br. 2006;88(10):1351-60. [ Links ]
11. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453-58. [ Links ]
12. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24(8):742-46. [ Links ]
13. Brumback RJ, Jones AL. Interobserver agreement in the classification of open fractures of the tibia. The results of a survey of two hundred and forty-five orthopaedic surgeons. J Bone Joint Surg Am. 1994;76(8):1162-66. [ Links ]
14. Horn BD, Rettig ME. Interobserver reliability in the Gustilo and Anderson classification of open fractures. J Orthop Trauma. 1993;7(4):357-60. [ Links ]
15. Anderson A, Miller AD, Brandon Bookstaver P. Antimicrobial prophylaxis in open lower extremity fractures. Open Access Emerg Med. 2011;3:7-11. [ Links ]
16. Patzakis MJ, Wilkins J. Factors influencing infection rate in open fracture wounds. Clin Orthop Relat Res. 1989;243:36-40. [ Links ]
17. Gosselin RA, Roberts I, Gillespie WJ. Antibiotics for preventing infection in open limb fractures. Cochrane Database Syst Rev. 2004;1:CD003764. [ Links ]
18. Mauffrey C, Bailey JR, Bowles RJ, Price C, Hasson D, Hak DJ, et al. Acute management of open fractures: proposal of a new multidisciplinary algorithm. Orthopedics. 2012;35(10):877-81. [ Links ]
19. Patzakis MJ, Wilkins J, Moore TM. Use of antibiotics in open tibial fractures. Clin Orthop Relat Res. 1983;178:31-35. [ Links ]
20. Hauser CJ, Adams CA, Jr., Eachempati SR, Council of the Surgical Infection S. Surgical Infection Society guideline: prophylactic antibiotic use in open fractures: an evidence-based guideline. Surg Infect (Larchmt). 2006;7(4):379-405. [ Links ]
21. Carver DC, Kuehn SB, Weinlein JC. Role of systemic and local antibiotics in the treatment of open fractures. Orthop Clin North Am. 2017;48(2):137-53. [ Links ]
22. Fletcher N, Sofianos D, Berkes MB, Obremskey WT. Prevention of perioperative infection. J Bone Joint Surg Am. 2007;89(7):1605-18. [ Links ]
23. Mundi R, Chaudhry H, Niroopan G, Petrisor B, Bhandari M. Open tibial fractures: updated guidelines for management. JBJS Rev. 2015;3(2). [ Links ]
24. Hoff WS, Bonadies JA, Cachecho R, Dorlac WC. East Practice Management Guidelines Work Group: update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma. 2011;70(3):751-54. [ Links ]
25. Nanchahal J. Standards for the management of open fractures of the lower limb. London: Royal Society of Medicine Press Ltd.; 2009. [ Links ]
26. Skinner D BK, Fitzsimmons C, Handley B, Hughes S, Jarman H, et al. National Clinical Guideline Centre. Final. Fractures (complex): assessment and management. 2016. [ Links ]
27. Patzakis MJ, Harvey JP, Jr., Ivler D. The role of antibiotics in the management of open fractures. J Bone Joint Surg Am. 1974;56(3):532-41. [ Links ]
28. Lack WD, Karunakar MA, Angerame MR, Seymour RB, Sims S, Kellam JF, et al. Type III open tibia fractures: immediate antibiotic prophylaxis minimizes infection. J Orthop Trauma. 2015;29(1):1-6. [ Links ]
29. Dellinger EP, Caplan ES, Weaver LD, Wertz MJ, Droppert BM, Hoyt N, et al. Duration of preventive antibiotic administration for open extremity fractures. Arch Surg. 1988;123(3):333-39. [ Links ]
30. Bergman BR. Antibiotic prophylaxis in open and closed fractures: a controlled clinical trial. Acta Orthop Scand. 1982;53(1):57-62. [ Links ]
31. Braun R, Enzler MA, Rittmann WW. A double-blind clinical trial of prophylactic cloxacillin in open fractures. J Orthop Trauma. 1987;1(1):12-17. [ Links ]
32. Carsenti-Etesse H, Doyon F, Desplaces N, Gagey O, Tancrede C, Pradier C, et al. Epidemiology of bacterial infection during management of open leg fractures. Eur J Clin Microbiol Infect Dis. 1999;18(5):315-23. [ Links ]
33. Dancer SJ. The problem with cephalosporins. J Antimicrob Chemother. 2001;48(4):463-78. [ Links ]
34. Lee J. Efficacy of cultures in the management of open fractures. Clin Orthop Relat Res. 1997;339:71-75. [ Links ]
35. Melvin JS, Dombroski DG, Torbert JT, Kovach SJ, Esterhai JL, Mehta S. Open tibial shaft fractures: I. Evaluation and initial wound management. J Am Acad Orthop Surg. 2010;18(1):10-19. [ Links ]
36. Seligson D, Berling S. Antibiotic-laden PMMA bead chains for the prevention of infection in compound fractures: current state of the art. Eur J Orthop Surg Traumatol. 2015;25(6):969-74. [ Links ]
37. Ostermann PA, Seligson D, Henry SL. Local antibiotic therapy for severe open fractures. A review of 1085 consecutive cases. J Bone Joint Surg Br. 1995;77(1):93-97. [ Links ]
38. Moehring HD, Gravel C, Chapman MW, Olson SA. Comparison of antibiotic beads and intravenous antibiotics in open fractures. Clin Orthop Relat Res. 2000;372:254-61. [ Links ]
39. Keating JF, Blachut PA, O'Brien PJ, Meek RN, Broekhuyse H. Reamed nailing of open tibial fractures: does the antibiotic bead pouch reduce the deep infection rate? J Orthop Trauma. 1996;10(5):298-303. [ Links ]
40. Craig J, Fuchs T, Jenks M, Fleetwood K, Franz D, Iff J, et al. Systematic review and meta-analysis of the additional benefit of local prophylactic antibiotic therapy for infection rates in open tibia fractures treated with intramedullary nailing. Int Orthop. 2014;38(5):1025-30. [ Links ]
41. Wahlig H, Dingeldein E, Bergmann R, Reuss K. The release of gentamicin from polymethylmethacrylate beads. An experimental and pharmacokinetic study. J Bone Joint Surg Br. 1978;60-B(2):270-75. [ Links ]
42. Large TM, Douglas G, Erickson G, Grayson JK. Effect of negative pressure wound therapy on the elution of antibiotics from polymethylmethacrylate beads in a porcine simulated open femur fracture model. J Orthop Trauma. 2012;26(9):506-11. [ Links ]
43. Stinner DJ, Hsu JR, Wenke JC. Negative pressure wound therapy reduces the effectiveness of traditional local antibiotic depot in a large complex musculoskeletal wound animal model. J Orthop Trauma. 2012;26(9):512-18. [ Links ]
44. Neubauer T, Bayer GS, Wagner M. Open fractures and infection. Acta Chir Orthop Traumatol Cech. 2006;73(5):301-12. [ Links ]
45. British Orthopaedic Association & British Association of Plastic, Reconstructive Aesthetic Surgeons; Audit Standards for Trauma Open Fractures (BOAST4) 2017 [Available from: https://www.boa.ac.uk/resources/boast-4-pdf.html. [ Links ]
46. Zalavras CG, Marcus RE, Levin LS, Patzakis MJ. Management of open fractures and subsequent complications. J Bone Joint Surg Am. 2007;89(4):884-95. [ Links ]
47. Godina M. Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg. 1986;78(3):285-92. [ Links ]
48. Salih S, Mills E, McGregor-Riley J, Dennison M, Royston S. Transverse debridement and acute shortening followed by distraction histogenesis in the treatment of open tibial fractures with bone and soft tissue loss. Strategies Trauma Limb Reconstr. 2018;13(3):129-35. [ Links ]
49. Marecek GS, Nicholson LT, Auran RT, Lee J. Use of a defined surgical approach for the debridement of open tibia fractures. J Orthop Trauma. 2018;32(1):e1-e4. [ Links ]
50. Schenker ML, Ahn J, Donegan D, Mehta S, Baldwin KD. The cost of after-hours operative debridement of open tibia fractures. J Orthop Trauma. 2014;28(11):626-31. [ Links ]
51. Naique SB, Pearse M, Nanchahal J. Management of severe open tibial fractures: the need for combined orthopaedic and plastic surgical treatment in specialist centres. J Bone Joint Surg Br. 2006;88(3):351-57. [ Links ]
52. Rajasekaran S. Early versus delayed closure of open fractures. Injury. 2007;38(8):890-95. [ Links ]
53. Gopal S, Majumder S, Batchelor AG, Knight SL, De Boer P, Smith RM. Fix and flap: the radical orthopaedic and plastic treatment of severe open fractures of the tibia. J Bone Joint Surg Br. 2000;82(7):959-66. [ Links ]
54. Steeby SF, Harvin WH, Worley JR, Della Rocca GJ, Volgas DA, Stannard JP, et al. Use of the dedicated orthopaedic trauma room for open tibia and femur fractures: does it make a difference? J Orthop Trauma. 2018;32(8):377-80. [ Links ]
55. Anglen JO. Wound irrigation in musculoskeletal injury. J Am Acad Orthop Surg. 2001;9(4):219-26. [ Links ]
56. Barnes S, Spencer M, Graham D, Johnson HB. Surgical wound irrigation: a call for evidence-based standardization of practice. Am J Infect Control. 2014;42(5):525-29. [ Links ]
57. Crowley DJ, Kanakaris NK, Giannoudis PV. Irrigation of the wounds in open fractures. J Bone Joint Surg Br. 2007;89(5):580-85. [ Links ]
58. Bhandari M, Adili A, Schemitsch EH. The efficacy of low-pressure lavage with different irrigating solutions to remove adherent bacteria from bone. J Bone Joint Surg Am. 2001;83(3):412-19. [ Links ]
59. Bhandari M, Schemitsch EH, Adili A, Lachowski RJ, Shaughnessy SG. High and low pressure pulsatile lavage of contaminated tibial fractures: an in vitro study of bacterial adherence and bone damage. J Orthop Trauma. 1999; 13(8):526-33. [ Links ]
60. Gross A, Bhaskar SN, Cutright DE, Beasley JD, 3rd, Perez B. The effect of pulsating water jet lavage on experimental contaminated wounds. J Oral Surg. 1971;29(3):187-90. [ Links ]
61. Bhhaskar SN, Cutright DE, Runsuck EE, Gross A. Pulsating water jet devices in debridement of combat wounds. Mil Med. 1971;136(3):264-66. [ Links ]
62. Polzin B, Ellis T, Dirschl DR. Effects of varying pulsatile lavage pressure on cancellous bone structure and fracture healing. J Orthop Trauma. 2006;20(4):261-66. [ Links ]
63. Petrisor B, Jeray K, Schemitsch E, Hanson B, Sprague S, Sanders D, et al. Fluid lavage in patients with open fracture wounds (FLOW): an international survey of 984 surgeons. BMC Musculoskelet Disord. 2008;9:7. [ Links ]
64. Investigators F, Bhandari M, Jeray KJ, Petrisor BA, Devereaux PJ, Heels-Ansdell D, et al. A trial of wound irrigation in the initial management of open fracture wounds. N Engl J Med. 2015;373(27):2629-41. [ Links ]
65. Anglen JO. Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds. A prospective, randomized study. J Bone Joint Surg Am. 2005;87(7):1415-22. [ Links ]
66. Anglen JO, Apostoles S, Christensen G, Gainor B. The efficacy of various irrigation solutions in removing slime-producing Staphylococcus. J Orthop Trauma. 1994;8(5):390-96. [ Links ]
67. Wei SJ, Cai XH, Wang HS, Qi BW, Yu AX. A comparison of primary and delayed wound closure in severe open tibial fractures initially treated with internal fixation and vacuum-assisted wound coverage: a case-controlled study. Int J Surg. 2014;12(7):688-94. [ Links ]
68. Hou Z, Irgit K, Strohecker KA, Matzko ME, Wingert NC, DeSantis JG, et al. Delayed flap reconstruction with vacuum-assisted closure management of the open IIIB tibial fracture. J Trauma. 2011;71(6):1705-708. [ Links ]
69. Hertel R, Lambert SM, Muller S, Ballmer FT, Ganz R. On the timing of soft-tissue reconstruction for open fractures of the lower leg. Arch Orthop Trauma Surg. 1999;119(1-2):7-12. [ Links ]
70. Bhandari M, Guyatt GH, Swiontkowski MF, Schemitsch EH. Treatment of open fractures of the shaft of the tibia. J Bone Joint Surg Br. 2001;83(1):62-68. [ Links ]
71. French B, Tornetta P, 3rd. High-energy tibial shaft fractures. Orthop Clin North Am. 2002;33(1):211-30, ix. [ Links ]
72. Russell GG, Henderson R, Arnett G. Primary or delayed closure for open tibial fractures. J Bone Joint Surg Br. 1990;72(1):125-28. [ Links ]
73. Hohmann E, Tetsworth K, Radziejowski MJ, Wiesniewski TF. Comparison of delayed and primary wound closure in the treatment of open tibial fractures. Arch Orthop Trauma Surg. 2007;127(2):131-36. [ Links ]
74. Harley BJ, Beaupre LA, Jones CA, Dulai SK, Weber DW. The effect of time to definitive treatment on the rate of nonunion and infection in open fractures. J Orthop Trauma. 2002;16(7):484-90. [ Links ]
75. Faisham WI, Nordin S, Aidura M. Bacteriological study and its role in the management of open tibial fracture. Med J Malaysia. 2001;56(2):201-206. [ Links ]
76. Levin LS. Early versus delayed closure of open fractures. Injury. 2007;38(8):896-99. [ Links ]
77. Rajasekaran S, Dheenadhayalan J, Babu JN, Sundararajan SR, Venkatramani H, Sabapathy SR. Immediate primary skin closure in type-III A and B open fractures: results after a minimum of five years. J Bone Joint Surg Br. 2009;91(2):217-24. [ Links ]
78. Melvin JS, Dombroski DG, Torbert JT, Kovach SJ, Esterhai JL, Mehta S. Open tibial shaft fractures: II. Definitive management and limb salvage. J Am Acad Orthop Surg. 2010;18(2):108-17. [ Links ]
79. Prasarn ML, Zych G, Ostermann PA. Wound management for severe open fractures: use of antibiotic bead pouches and vacuum-assisted closure. Am J Orthop (Belle Mead NJ). 2009;38(11):559-63. [ Links ]
80. Stannard JP, Volgas DA, Stewart R, McGwin G, Jr., Alonso JE. Negative pressure wound therapy after severe open fractures: a prospective randomized study. J Orthop Trauma. 2009;23(8):552-57. [ Links ]
81. Tan Y, Wang X, Li H, Zheng Q, Li J, Feng G, et al. The clinical efficacy of the vacuum-assisted closure therapy in the management of adult osteomyelitis. Arch Orthop Trauma Surg. 2011;131(2):255-59. [ Links ]
82. Prokuski L. Negative pressure dressings for open fracture wounds. Iowa Orthop J. 2002;22:20-24. [ Links ]
83. Dedmond BT, Kortesis B, Punger K, Simpson J, Argenta J, Kulp B, et al. The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibial shaft fractures. J Orthop Trauma. 2007;21(1):11-17. [ Links ]
84. Bollero D, Carnino R, Risso D, Gangemi EN, Stella M. Acute complex traumas of the lower limbs: a modern reconstructive approach with negative pressure therapy. Wound Repair Regen. 2007;15(4):589-94. [ Links ]
85. Blum ML, Esser M, Richardson M, Paul E, Rosenfeldt FL. Negative pressure wound therapy reduces deep infection rate in open tibial fractures. J Orthop Trauma. 2012;26(9):499-505. [ Links ]
86. Krug E, Berg L, Lee C, Hudson D, Birke-Sorensen H, Depoorter M, et al. Evidence-based recommendations for the use of negative pressure wound therapy in traumatic wounds and reconstructive surgery: Steps towards an international consensus. Injury. 2011;42(S1):S1-S12. DOI: 10.1016/S0020-1383(11)00041-6. [ Links ]
87. Cross WW, 3rd, Swiontkowski MF. Treatment principles in the management of open fractures. Indian J Orthop. 2008;42(4):377-86. [ Links ]
88. Merritt K. Factors increasing the risk of infection in patients with open fractures. J Trauma. 1988;28(6):823-27. [ Links ]
89. Merritt K, Dowd JD. Role of internal fixation in infection of open fractures: studies with Staphylococcus aureus and Proteus mirabilis. J Orthop Res. 1987;5(1):23-28. [ Links ]
90. Worlock P, Slack R, Harvey L, Mawhinney R. The prevention of infection in open fractures: an experimental study of the effect of fracture stability. Injury. 1994;25(1):31-38. [ Links ]
91. O'Toole RV, Gary JL, Reider L, Bosse MJ, Gordon WT, Hutson J, et al. A prospective randomized trial to assess fixation strategies for severe open tibia fractures: modern ring external fixators versus internal fixation (FIXIT Study). J Orthop Trauma. 2017;31 Suppl 1:S10-S7. [ Links ]
92. Inan M, Halici M, Ayan I, Tuncel M, Karaoglu S. Treatment of type IIIA open fractures of tibial shaft with Ilizarov external fixator versus unreamed tibial nailing. Arch Orthop Trauma Surg. 2007;127(8):617-23. [ Links ]
93. Webb LX, Bosse MJ, Castillo RC, MacKenzie EJ, Group LS. Analysis of surgeon-controlled variables in the treatment of limb-threatening type-III open tibial diaphyseal fractures. J Bone Joint Surg Am. 2007;89(5):923-28. [ Links ]
94. Second International Consensus Meeting on Musculoskeletal Infections 2018 [Available from: https://icmphilly.com/document/icm-2018-trauma-document/. [ Links ]
95. Bhandari M, Zlowodzki M, Tornetta P, 3rd, Schmidt A, Templeman DC. Intramedullary nailing following external fixation in femoral and tibial shaft fractures. J Orthop Trauma. 2005; 19(2):140-44. [ Links ]
96. Yokoyama K, Uchino M, Nakamura K, Ohtsuka H, Suzuki T, Boku T, et al. Risk factors for deep infection in secondary intramedullary nailing after external fixation for open tibial fractures. Injury. 2006;37(6):554-60. [ Links ]
97. Ozturkmen Y, Karamehmetoglu M, Karadeniz H, Azboy I, Caniklioglu M. Acute treatment of segmental tibial fractures with the Ilizarov method. Injury. 2009;40(3):321-26. [ Links ]
98. Hutson JJ, Jr., Dayicioglu D, Oeltjen JC, Panthaki ZJ, Armstrong MB. The treatment of gustilo grade IIIB tibia fractures with application of antibiotic spacer, flap, and sequential distraction osteogenesis. Ann Plast Surg. 2010;64(5):541-52. [ Links ]
99. Lerner A, Fodor L, Soudry M. Is staged external fixation a valuable strategy for war injuries to the limbs? Clin Orthop Relat Res. 2006;448:217-24. [ Links ]
100. Nieuwoudt L, Marais LC. Short-term results of grade III open tibia fractures treated with circular fixators. SA Orthop J. 2016;15(3):20-26. [ Links ]
101. D'Alleyrand JC, Manson TT, Dancy L, Castillo RC, Bertumen JB, Meskey T, et al. Is time to flap coverage of open tibial fractures an independent predictor of flap-related complications? J Orthop Trauma. 2014;28(5):288-93. [ Links ]
102. Menakaya CU, Rigby AS, Hadland Y, Barron E, Sharma H. Fracture healing following high energy tibial trauma: Ilizarov versus Taylor Spatial Frame. Ann R Coll Surg Engl. 2014;96(2):106-10. [ Links ]
103. Henderson DJ, Barron E, Hadland Y, Sharma HK. Functional outcomes after tibial shaft fractures treated using the Taylor spatial frame. J Orthop Trauma. 2015;29(2):e54-59. [ Links ]
104. Nho SJ, Helfet DL, Rozbruch SR. Temporary intentional leg shortening and deformation to facilitate wound closure using the Ilizarov/Taylor spatial frame. J Orthop Trauma. 2006;20(6):419-24. [ Links ]
105. El-Rosasy MA. Acute shortening and re-lengthening in the management of bone and soft-tissue loss in complicated fractures of the tibia. J Bone Joint Surg Br. 2007;89(1):80-88. [ Links ]
106. Saleh M, Rees A. Bifocal surgery for deformity and bone loss after lower-limb fractures. Comparison of bone-transport and compression-distraction methods. J Bone Joint Surg Br. 1995;77(3):429-34. [ Links ]
107. Saleh M, Yang L, Sims M. Limb reconstruction after high energy trauma. Br Med Bull. 1999;55(4):870-84. [ Links ]
108. Hohmann E, Birkholtz F, Glatt V, Tetsworth K. The 'Road to Union' protocol for the reconstruction of isolated complex high-energy tibial trauma. Injury. 2017;48(6):1211-16. [ Links ]
109. Sen C, Kocaoglu M, Eralp L, Gulsen M, Cinar M. Bifocal compression-distraction in the acute treatment of grade III open tibia fractures with bone and soft-tissue loss: a report of 24 cases. J Orthop Trauma. 2004;18(3):150-57. [ Links ]
110. Gulsen M, Ozkan C. Angular shortening and delayed gradual distraction for the treatment of asymmetrical bone and soft tissue defects of tibia: a case series. J Trauma. 2009;66(5):E61-66. [ Links ]
111. Giovannini F, De Palma L, Panfighi A, Marinelli M. Intramedullary nailing versus external fixation in Gustilo type III open tibial shaft fractures: a meta-analysis of randomised controlled trials. Strategies Trauma Limb Reconstr. 2016;11 (1):1-4. [ Links ]
112. Cierny G, 3rd, Byrd HS, Jones RE. Primary versus delayed soft tissue coverage for severe open tibial fractures. A comparison of results. Clin Orthop Relat Res. 1983;178:54-63. [ Links ]
113. Caudle RJ, Stern PJ. Severe open fractures of the tibia. J Bone Joint Surg Am. 1987;69(6):801-807. [ Links ]
114. Fischer MD, Gustilo RB, Varecka TF. The timing of flap coverage, bone-grafting, and intramedullary nailing in patients who have a fracture of the tibial shaft with extensive soft-tissue injury. J Bone Joint Surg Am. 1991;73(9):1316-22. [ Links ]
115. Pollak AN, McCarthy ML, Burgess AR. Short-term wound complications after application of flaps for coverage of traumatic soft-tissue defects about the tibia. The Lower Extremity Assessment Project (LEAP) Study Group. J Bone Joint Surg Am. 2000;82(12):1681-91. [ Links ]
116. Mathews JA, Ward J, Chapman TW, Khan UM, Kelly MB. Single-stage orthoplastic reconstruction of Gustilo-Anderson grade III open tibial fractures greatly reduces infection rates. Injury. 2015;46(11):2263-66. [ Links ]
117. Harrison WJ, Lewis CP, Lavy CB. Open fractures of the tibia in HIV positive patients: a prospective controlled single-blind study. Injury. 2004;35(9):852-56. [ Links ]
118. Harrison WJ. Open tibia fractures in HIV-positive patients. Malawi Med J. 2009;21(4):174-75. [ Links ]
119. Aird J, Noor S, Lavy C, Rollinson P. The effect of HIV on early wound healing in open fractures treated with internal and external fixation. J Bone Joint Surg Br. 2011;93(5):678-83. [ Links ]
120. Howard NE, Phaff M, Aird J, Wicks L, Rollinson P. Does human immunodeficiency virus status affect early wound healing in open surgically stabilised tibial fractures?: A prospective study. Bone Joint J. 2013;95-B(12):1703-707. [ Links ]
121. Hao J, Herbert B, Quispe JC, Cuellar DO, Chadayammuri V, Kim JW, et al. An observational case series of HIV-positive patients treated with open reduction internal fixation for a closed lower extremity fracture. Eur J Orthop Surg Traumatol. 2015;25(5):815-19. [ Links ]
122. Phaff M, Aird J, Rollinson PD. Delayed implants sepsis in HIV-positive patients following open fractures treated with orthopaedic implants. Injury. 2015;46(4):590-94. [ Links ]
 Correspondence:
Correspondence:
Dr MA Manjra
Division of Orthopaedics, Tygerberg Hospital
Cape Town, Western Cape, 7505, South Africa
tel: +27 (21) 938 5456
email: m.manjra@ymail.com
Received: September 2019
Accepted: October 2019
Published: November 2019
Funding: There are no funding sources to declare.
Editor: Prof LC Marais, University of KwaZulu-Natal, Durban, South Africa
Conflict of interest: All authors confirm that there are no conflicts of interest to declare.


{kind=link}