










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.16 n.4 Centurion Nov./Dec. 2017
http://dx.doi.org/10.17159/2309-8309/2017/v16n4a6
SHOULDER
Introduction of the angle of shoulder slope in a South African population
Naidoo NI; Lazarus LII; Van Tongel AIII; Osman SAIV; Satyapal KSV
IB Med Sci (UKZN), B Med Sci Hons (Anat)(UKZN), PhD (Health Sciences)(Anat)(UKZN), Assistant Professor (Anat), College of Medicine, Mohammed Bin Rashid University of Medicine and Health Sciences, Dubai Healthcare City, Dubai, United Arab Emirates
IIB Med Sci (with Honours) (UKZN), M Med Sci (cum laude) (UKZN), PG Dip in Higher Education (UKZN), PhD (Health Sciences)(Anat)(UKZN), Lecturer (Anat), Department of Clinical Anatomy, School of Laboratory Medicine and Medical Sciences, UKZN, Durban, South Africa
IIIMD (KU Leuven, Belgium), PhD (Health Sciences)(UGhent, Belgium), Clinical Professor (Orth Surg), Director of Clinical Research (Orth Dept UGhent), Department of Physical Medicine and Orthopaedic Surgery, Ghent University, Ghent, Belgium
IVLRCP SI MBBCh BAO (NUI) (Ireland), FSC (SA) Orth (SA), Orthopaedic Surgeon, Suite 11: Medical Centre East, Life Entabeni Hospital, Durban, South Africa
VRCP, LRCS, LM (Royal College of Physicians & Surgeons in Ireland), MD: General Surgery (Doctor of Medicine: University of Natal), FRCPI (Fellow of the Royal College of Physicians of Ireland), FICA (Fellow of the International College of Angiology, USA), Fellow of the UKZN, LLM (Medical Law)(UKZN), Senior Professor and Fellow, Department of Clinical Anatomy, School of Laboratory Medicine and Medical Sciences, UKZN, Durban, South Africa
ABSTRACT
BACKGROUND: The angle of shoulder slope has been reported in accordance with the specific occupational activities of the aviation and textile industries. However, as no accurate definition nor standardised anatomical landmarks exist within the medical field, this study aimed to devise an appropriate definition with preplaced reference landmarks. In addition, the vertebral level of the acromial tip was also determined.
METHODS: The sample series comprised 260 posterior radiographs of the shoulder, of which 127 were males and 133 females. The ethnic distribution included ten black, 13 coloured, 49 Indian and 188 white individuals. In accordance with the trapezial line, the angle of shoulder slope was defined and measured as the angle between the line from the spinous process of C7 to the acromial tip and the line from the acromial tip directly across to the median plane of the vertebral column.
RESULTS: The standard mean angle of shoulder slope was approximately 13.56±3.70°. Left and right sides appeared to have mean angles of 13.81±3.41° and 13.33±3.95°, respectively. Mean angular values were also calculated in accordance with the demographic representation - sex: male 13.64±3.71°, female 13.48±3.71°; ethnic groups: black: 13.81±3.81°, coloured: 12.18±3.82°, Indian: 12.97±3.09°, white: 13.64±3.96°. Although the acromial tip was commonly aligned to the level of the spinous process of T3, the incidence of the vertebral level of the acromion was categorised into seven groups, viz. i) intervertebral disc between T1 and T2; ii) intervertebral disc between T2 and T3; iii) intervertebral disc between T3 and T4; iv) spinous process of T1; v) spinous process of T2; vi) spinous process of T3; vii) spinous process of T4.
CONCLUSION: Since a statistically significant P value was recorded for the comparison between the angle of shoulder slope and the acromial vertebral level, it was postulated that the magnitude of the angle may determine the acromial vertebral level. As the present study incorporated standard osteological landmarks into the definition and calculation of the angle of shoulder slope, it may provide reference data regarding the position of the acromion which may be indicative of shoulder asymmetry and distorted shoulder setting.
Level of evidence: Level 3.
Key words: angle, shoulder slope, acromion, vertebral level
Introduction
Although the textile and aviation industries have reported the angle of shoulder slope in accordance with the specific occupational activities, a comprehensive investigation of the literature found a distinct discrepancy in the actual definition of the angle of shoulder slope between these industries.1,2
As a result of variation in the physique of human bodies and the need to produce garments that fit a wide range of body types, the textile industry has employed computer-aided 3D body scanner software to randomly determine antero-lateral points at the cervical and glenohumeral regions in attempts to quantify the angle of shoulder slope.2 On the contrary, the popularity of male pilots and the accepted socio-economic standards specific to the 1960s led the aviation industry to include the angle of shoulder slope for the design of aviation harnesses.1 Since a unilateral concentration of load causes the compression of the underlying structures and impairment of pilot performance, this posterior morphometric parameter incorporated the profile of the shoulder from the contour of underlying soft tissue.1 While the aviation industry integrated both the trapezial and deltoid segments of the back, no accurate record of preplaced landmarks exists within the textile industry.1,2
Despite the apparent lack of an accurate definition and standardised anatomical landmarks within the medical field, the asymmetry of the shoulders and subsequent distorted shoulder setting are considered to be characteristic of scoliosis.1-3Therefore, this study devised an appropriate definition of the angle of shoulder slope with standardised anatomical landmarks. Since current literary sources are yet to describe the vertebral level of the acromion, the current study also proceeded to document this.4
Materials and methods
Subsequent to the gatekeepers' permission from the University of KwaZulu-Natal and Life Entabeni Hospital, Durban, South Africa (Ethical Clearance Approval Number: BE279/15), 260 posterior radiographs of the shoulder were subjected to the devised methodology (GE Healthcare Centricity PACS - IW Dynamic Imaging 3.7.3.9). The sample consisted of 127 male and 133 female individuals with a mean age of 51.80±13.93 years. The demographic representation included ten black, 13 coloured, 49 Indian and 188 white individuals.
With regard to the radiographical protocol, each patient was seated upright with the hand supinated, the arm externally rotated and without support of the arm. The greater humeral tubercle was situated laterally, while the lesser humeral tubercle was seen to lie anteriorly.
Since the trapezial line accounted for the contour of the shoulder (i.e. trapezius muscle arises from the spinous process of C7),4 the standard anatomical definition of the angle of shoulder slope was based upon osteological landmarks and was measured as the angle between the line from the spinous process of C7 to the acromial tip (SpA) and the line from the acromial tip directly across to the respective point in the median plane of the vertebral column (AVc) (Figure 1). As the horizontal line extending medially from the acromial tip was directly perpendicular to the vertebral column, the vertebral level corresponding to the acromial tip was identified and recorded (Figure 1).

Non-parametric and descriptive statistical tests were conducted to determine the means and frequencies of the sample (IBM Statistical Package for Social Sciences, version 21.0). Levels of significance were reported when P values were less than 0.05.
Results
The mean angle of shoulder slope was found to be 13.56±3.70° (Table I).

In male and female individuals, the mean angles of shoulder slope were 13.64±3.71° and 13.48±3.71°, respectively (Table I).
Left and right sides presented with mean angles of 13.81±3.41° and 13.33±3.95°, accordingly (Table I).
The mean angle of shoulder slope was also documented within each ethnic group, viz. black: 13.81±3.81°, coloured: 12.18±3.82°, Indian: 12.97±3.09° and white: 13.64±3.96° (Table I).
A statistically significant P value of 0.000 was recorded between the standard mean angle and age (Table I).
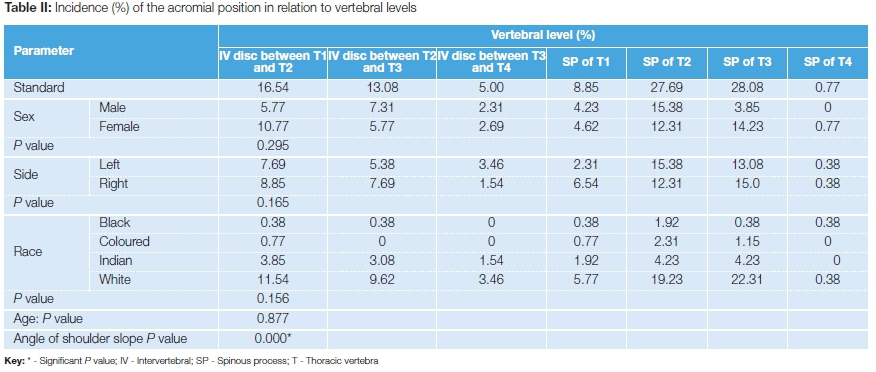
The incidence of the vertebral level of the acromial tip was categorised into seven groups according to standard, side and the respective demographic factors (Figure 1, Table II):
i) Intervertebral disc between T1 and T2 - 16.54%
Sex: male [5.77%], female [10.77%]; side: left [7.69%], right [8.85%]; race: black [0.38%], coloured [0.77%], Indian [3.85%], white [11.54%]
ii) Intervertebral disc between T2 and T3 - 13.08%
Sex: male [7.31%], female [5.77%]; side: left [5.38%], right [7.69%]; race: black [0.38%], coloured [0%], Indian [3.08%], white [9.62%]
iii) Intervertebral disc between T3 and T4 - 5.00%
Sex: male [2.31%], female [2.69%]; side: left [3.46%], right [1.54%]; race: black [0%], coloured [0%], Indian [1.54%], white [3.46%]
iv) Spinous process of T1 - 8.85%
Sex: male [4.23%], female [4.62%]; side: left [2.31%], right [6.54%]; race: black [0.38%], coloured [0.77%], Indian [1.92%], white [5.77%]
v) Spinous process of T2 - 27.69%
Sex: male [15.38%], female [12.31%]; side: left [15.38%], right [12.31%]; race: black [1.92%], coloured [2.31%], Indian [4.23%], white [19.23%]
vi) Spinous process of T3 - 28.08%
Sex: male [13.85%], female [14.23%]; side: left [13.08%], right [15.0%]; race: black [0.38%], coloured [1.15%], Indian [4.23%], white [22.31%]
vii) Spinous process of T4 - 0.77%
Sex: male [0%], female [0.77%]; side: left [0.38%], right [0.38]; race: black [0.38%], coloured [0%], Indian [0%], white [0.38%]
The comparison between the angle of shoulder slope and the vertebral level of the acromial tip yielded a statistically significant P value of 0.000 (Table II).
Discussion
The current study investigated the angle of shoulder slope within the South African population by providing mean angle values according to the general and demographic representation of the sample. As the biomechanical imbalance in the angle of shoulder slope may impair shoulder functionality as well as other closely related organ systems, the definition of the angle of shoulder slope was denoted by standard anatomical reference points, viz. the spinous process of the seventh cervical vertebra, the median plane of the vertebral column and the acromial tip, which were unique to this study.3
Although the only former study was conducted in 1965, the sample was exclusively limited to male air traffic service trainees. On the contrary, the present study evaluated the angle of shoulder slope in both male and female individuals. Male individuals presented with marginally larger angles which may be linked to the presence of testosterone. Furthermore, Hughes and Gallup5 reported that the correlation of such parameters to the hip and waist, may assist to predict dimensions of sexual behaviour.
Despite the right-side dominance that is predominantly seen in the upper limb, the mean angle of shoulder slope appeared slightly larger on the left side.6 Given that the mean angle of shoulder slope was largest within the black ethnic group (13.81±3.81°), there were negligible differences in the mean value when compared to the white ethnic group. This may be accounted for by the small number of black individuals represented within the sample.
The statistically significant P value of 0.000, that was recorded for the comparison between the standard mean angle and age, may suggest that a proportionality relationship exists between these two parameters such that an increase in age may result in a larger angle.
While the acromion bears relevance to the geometry of the shoulder, the vertebral level of the acromial tip has not been stated in the literature reviewed, therefore this study was also complemented by the analysis of the vertebral level of the acromial tip.7-9 This study established seven categories reporting the vertebral level of the acromion. The acromial tip was most commonly situated in relation to the level of the spinous process of T3 (28.08%) (Figure 2).

In male and female individuals, the acromial tip was frequently aligned to the spinous processes of T2 (15.38%) and T3 (14.23%), respectively.
On the left side, the acromion tip was located at the level of the spinous process of T2 (15.38%), while the right side was marked with the highest incidence at the level of the spinous process of T3 (15.0%).
With regard to the predominance of vertebral levels within each ethnic group, the acromial tip was situated at the level of the spinous process of T2 in both black (1.92%) and coloured (2.31 %) individuals. Although the Indian ethnic group presented with equal incidences of the acromial tip at the level of spinous processes of T2 (4.23%) and T3 (4.23%), the acromial tip was frequently located at the level of the spinous process of T3 in white individuals.
It may be postulated from the statistically significant P value yielded for the comparison between the angle of shoulder slope and the acromial vertebral level (P value=0.000), that the magnitude of the angle may determine the vertebral level at which the acromion would be situated.
In accordance with the economic conditions and trends of the 1960s, somatotype photography was used as the popular imaging resource of choice to measure the posterior angle of shoulder slope as reported by Snow.1 However, the present study employed the use of radiographs which are inexpensive, easily accessible and frequently-used imaging resources. Furthermore, the use of the spinous process of C7 as an anatomical landmark accounted for the trapezial contour of the shoulder as it is also the origin site of the trapezius muscle.4
Although this study excluded all radiographs that presented with fracture and/or abnormalities of the cervico-thoracic vertebral column and scapula, the presence of a malunited clavicle may result in an abnormal shoulder setting, thus affecting magnitude of the angle of shoulder slope and the vertebral level of the acromial tip. In addition, acromial osteophytes resembling hooked type III acromia may have influenced the size of the angle of shoulder slope. Since periosteal apposition leads to an increased cross-sectional vertebral body area in elderly males, it may be recommended that future studies also evaluate the vertebral body size during quantification of the angle of shoulder slope and acromial tip vertebral level.10,11
Conclusion
The quantification of the angle of shoulder slope and the determination of the acromial vertebral level may provide reliable reference landmarks and morphometric data necessary for glenohumeral surgery. This study also classified the vertebral levels of the acromial tip into seven categories which may prevent misinterpretation during analysis of radiographs. In addition, the acromial tip was commonly situated at the level of the spinous process of T3.
Acknowledgements
The authors wish to acknowledge the National Research Foundation.
Compliance with ethics guidelines
Permission to conduct this study was obtained from the University of KwaZulu-Natal and Life Entabeni Hospital, Durban, South Africa (Ethical Clearance Approval Number: BE279/15).
References
1. Snow CC. 1965. The angle of shoulder slope in normal males as a factor in shoulder-harness design. AM 1965;65(14):1 -3. [ Links ]
2. Chen C-M. Analysis of upper physical characteristics based on angle measurements. Textile Res J 2011 ;81 (3):301 -10. [ Links ]
3. Drzal-Grabiec J, Snela S, Podgorska-Bednarz J, Rykala J, Banas A. Examination of the compatibility of the photogrammetric method with the phenomenon of mora projection in the evaluation of scoliosis. BioMed Res Int 2014;1-6. [ Links ]
4. Standring S. Gray's Anatomy: The Anatomical Basis of Clinical Practice. Spain: Elsevier Ltd; 2016. [ Links ]
5. Hughes SM, Gallup GG. Sex differences in morphological predictors of sexual behavior: Shoulder to hip and waist to hip ratios. Evolution and Human Behavior 2003;24(3):173-78. [ Links ]
6. Singh I. Functional asymmetry in the lower limbs. Cells Tissues Organs 1970;77(1):131 -38. [ Links ]
7. Bigliani L, Morrison D, April E. The morphology of the acromion and its relationship to rotator cuff tears. Orthop Trans 1986;228. [ Links ]
8. Collipal E, Silva H, Ortega L, Espinoza E, Martinez C. The acromion and its different forms. Int J Morphol 2010;28(4):1189-92. [ Links ]
9. Gupta C, Priya A, Kalthur SG, D'Souza AS. A morphometric study of acromion process of scapula and it clinical significance. CHRISMED J Health Res 2014;1 (3):164-69. [ Links ]
10. Mosekilde L. Sex differences in age-related changes in vertebral body size, density and biomechanical competence in normal individuals. Bone 1990;11 (2):67-73. [ Links ]
11. Junno J-A, Paanenen M, Karppinen J, Niinmaki J, Niskanen M, Maijanen H, Vare T, Jarvelin M-R, Nieminen MT, Tuukkanen J, Ruff C. Age-related trends in vertebral dimensions. Journal of Anatomy 2015;226(5):434-39. [ Links ]
 Correspondence:
Correspondence:
Prof KS Satyapal
Department of Clinical Anatomy, College of Health Sciences
School of Laboratory Medicine and Medical Sciences, Westville Campus, College of Health Sciences
University of KwaZulu-Natal
Private Bag X54001, Durban, 4000
Tel: +27 31 260 7899
Cell: +27 83 777 8780
Fax: + 27 31 260 7890
Email: satypalk@ukzn.ac.za
Received: September 2016
Accepted: March 2017
Published: November 2017
Funding: This work was supported by the National Research Foundation (Grant UID: 94970).
Conflict of interest: xThe authors have no conflicts of interest to declare.
Editor: Prof Anton Schepers, University of Witwatersrand


{kind=link}