










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.16 no.4 Centurion nov./dic. 2017
http://dx.doi.org/10.17159/2309-8309/2017/v16n4a3
TUMOUR AND SEPSIS
A rare case of angioleiomyoma around the ankle: case report and review of literature
Nakale NTI; Saragas NPII; Ferrao PNFIII; Strydom AIV
IBSc(UNAM), MBChB(UKZN), Registrar, Orthopaedic Surgery Department, University of Witwatersrand, Johannesburg, South Africa
IIMBBCh(Wits), FCS(SA)Ortho, MMed(Ortho Surg)(Wits), The Orthopaedic Foot and Ankle Unit, University of the Witwatersrand and Netcare Linksfield Hospital, Johannesburg, South Africa
IIIMBChB(Pret), FCS(SA)Ortho, The Orthopaedic Foot and Ankle Unit, University of the Witwatersrand and Netcare Linksfield Hospital, Johannesburg, South Africa
IVMBBCh(Wits), FC Ortho (SA), MMed(Ortho Surg)(Wits), The Orthopaedic Foot and Ankle Unit, University of the Witwatersrand and Netcare Linksfield Hospital, Johannesburg, South Africa
ABSTRACT
Angioleiomyoma is a slow-growing benign tumour that originates from the tunica media layer of vessel walls. It represents 4.4-5% of all benign soft tissue tumours and 0.2% of all tumours in the foot and ankle. Excisional biopsy of the tumour is both diagnostic and curative, with a low recurrence rate reported in the literature. Malignant transformation has been described in 1 % of cases. We present a case of a 67-year-old female diagnosed with angioleiomyoma at the lateral malleolus.
Level of evidence: Level 5
Key words: angioleiomyoma, benign ankle, soft tissue tumour, vascular tumour
Introduction
Angioleiomyoma of the foot and ankle is a rare benign soft tissue tumour of unknown aetiology originating from blood vessel walls typically affecting middle-aged women between the fourth and sixth decade. Angioleiomyoma should be considered as part of the differential diagnosis of painful masses around the foot and ankle as it has the potential of malignant transformation.
Case report
A 67-year-old female presented with acute pain, of three-month duration, over the right lateral aspect of the ankle. She described the pain as an extreme burning sensation, especially when touching the small nodule on the side of her leg. She described no prior history of injury. Clinical findings were those of a small hard nodule on the posterior border of the fibula approximately 5 cm proximal to the tip of the lateral malleolus (Figure 1). This area was extremely sensitive to light touch, with a positive Tinel sign. The rest of the examination was unremarkable.

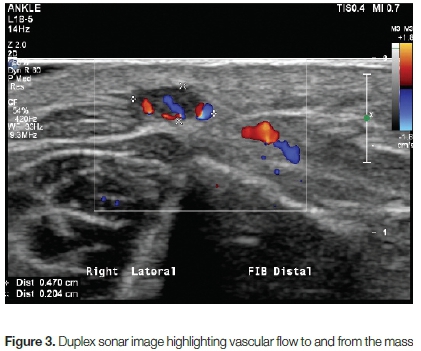
Ultrasound (Figure 2) reported a well-circumscribed 4.8x4.4x2.2 mm hypoechoic mass in the subcutaneous tissue overlying the right distal fibula with moderate to marked vascular flow (Figure 3). A nerve entering the tumour was identified, measuring 1.7 mm and appeared to be thickened on exiting the tumour, with a diameter of 4.3 mm.

The patient was advised to have an excisional biopsy of the mass, to which she agreed. The tumour was excised in its entirety through a direct approach (Figure 4). The mass was found to be in the subcutaneous tissue with no obvious nerves or vessels leading from it.

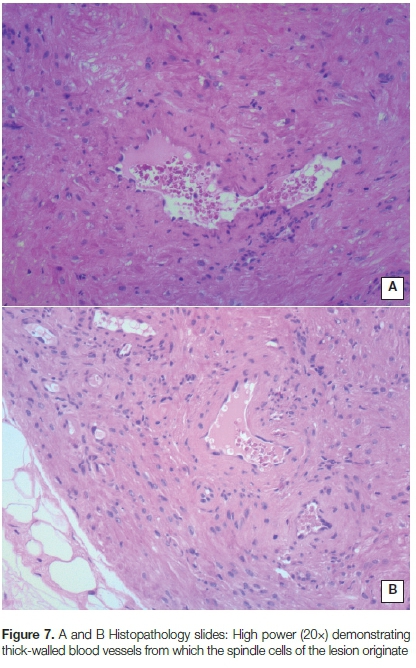
The tumour measured 9x5x1 mm macroscopically (Figure 5). Microscopic histopathological evaluation revealed a circumscribed but encapsulated proliferation of smooth muscle bundles arranged in intersecting fascicles (Figure 6). These were centred around and spanned thick-walled blood vessels within the lesion (Figure 7). With no cytologic atypia or malignancy present, these features represented a benign angioleiomyoma.


The wound healed at two weeks and the patient returned to normal activities at four weeks. At one-year follow-up, the patient's symptoms resolved completely with no post-operative complications reported.
Discussion
Angioleiomyoma is a benign slow-growing tumour that originates from the tunica media layer of smooth non-striated muscle in blood vessel walls. Angioleiomyomas are quite rare, representing 4.4-5% of all benign soft tissue tumours.1,2
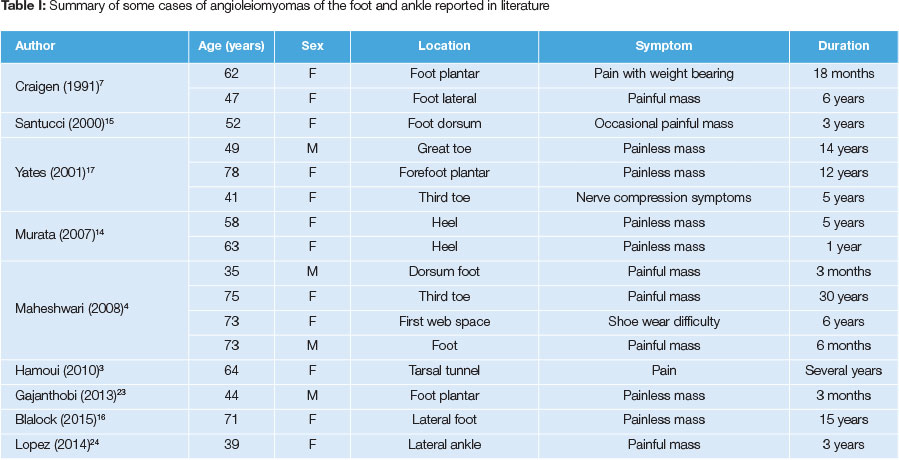
Angioleiomyomas have a predilection for the lower limb and are commonly found in women between the fourth and sixth decade.1,3,4The majority of cases of angioleiomyoma reported in the English literature are in the form of case reports and case series, some of which are summarised in Table I.
The reported incidence of angioleiomyoma around the foot and ankle is 0.2% of all tumours of the foot and ankle.5,6 Craigen and Anderson reported three cases of angioleiomyoma out of the 161 cases of smooth muscle tumours in the foot and ankle over a 10-year period.7Macdonald et al. reported a 2% incidence of angioleiomyomas in 101 cases of foot masses during a four-year period.8 Azevado et al. reviewed 72 cases of foot and ankle tumours treated at a single institution over a ten-year period and found that 5.5% of these tumours were angioleiomyomas.9
The aetiology of angioleiomyoma remains unknown, and multiple factors have been proposed ranging from minor trauma, venous stasis, pregnancy, oestrogen therapy and hormonal alteration.2,3,10-12A genetic predisposition has also been proposed in individuals with an autosomal dominant inheritance.13
Vascular malformations from arteriovenous anastomosis or haematoma formation following local minor trauma may also result in an angioleiomyoma. Up to 60% of cases will present with a painful, solitary subcutaneous nodule which may be associated with discomfort with shoe wear.1 The tumour may be asymptomatic for years prior to making the diagnosis.1 Presence of pain may be due to irritation of an involved nerve, smooth muscle contraction or blood vessel spasm secondary to ischaemia.3 The tumour rarely exceeds 2 cm in size.3,4,14,15
Clinical findings and imaging are supportive, with the diagnosis being confirmed on histopathological analysis of the excisional biopsy specimen. However, it is still important to consider other possible causes for a painful foot mass including glomus tumour, fibroma, haemangioma, lipoma, schwannoma and giant cell tumour (Table II). A few cases of a calcified angioleiomyoma, seen on plain radiographs as a calcified mass located at the site of symptoms, have been reported.4,14,16 The tumour may exert a compressive effect on bone which is visible on X-ray, otherwise plain X-rays are usually normal.17

Ultrasound features only show a homogenous structure with well-defined margins. MRI shows a smooth muscle mass, with numerous vessels within it, that is hyperintense on the T2-weighted sequence. There is strong enhancement after contrast media, consistent with abundant vascularity of the tumour.3,4
The classic morphological appearance is that of a sharply circumscribed but encapsulated mass usually measuring less than 2 cm in diameter.16 Microscopically there are bundles of mature smooth muscle oriented around blood vessels showing solid growth of compact spindle cells with ovoid nuclei. Mitotic activity is usually sparse to absent.
Hachisuga et al. described three histological types, which was modified by Katenkamp et al. who added a fourth type (Table III).1,18Secondary changes may also be present including myxoid change, hyalinisation or calcification.4,14,16 Excision biopsy is both diagnostic and curative, as recurrence is very rare. Malignant transformation has been reported in 1% of cases, into angioleiomyosarcoma.1,19-22

Conclusion
Angioleiomyoma is rarely encountered in the foot and ankle. However, it remains an important differential diagnosis for a painful foot and ankle soft tissue tumour, due to the risk of malignant transformation. Excisional biopsy is both diagnostic and curative.
Acknowledgements
• Dr Lauren Blackburn, associate pathologist, Drs Gritzman and Thatcher Inc. for providing the histopathology images and report
• Beverly Roos, ultrasonographer, The Centre for Sports Medicine and Orthopaedics for providing the ultrasound images
References
1. Hachisuga T, Hashimoto H, Enjoji M. Angioleiomyoma: A clinicopathologic reappraisal of 562 cases. Cancer. 1984;54:126-30. [ Links ]
2. Ramesh P, Annapureddy SR, Khan F, Sutaria PD. Angioleiomyoma: a clinical, pathological and radiological review. Int J Clin Pract. 2004;58:587-91. [ Links ]
3. Hamoui M, Largey A, Ali M, et al. Angioleiomyoma in the ankle mimicking tarsal tunnel syndrome: a case report and review of the literature. J Foot Ankle Surg. 2010;49(398):9-15. [ Links ]
4. Maheshwari AV, Temple HT, Murocacho CA. Calcified angiomyomas of the foot: a case report. Foot Ankle Int. 2008;29(4):449-55. [ Links ]
5. Berlin S. Statistical analysis of 307,601 tumours and other lesions of the foot. J Am Podiatr Med Assoc. 1995;85(11):699-703. [ Links ]
6. Berlin S. A laboratory review of 67,000 foot tumors and lesions. J Am Podiatr Med Assoc. 1984;74:341-47. [ Links ]
7. Craigen MAC, Anderson EG. Smooth muscle tumours in the foot. The Foot. 1991;1:33-34. [ Links ]
8. Macdonald DJ, Holt G, Vass K, Marsh A, Kumar CS. The differential diagnosis of foot lumps: 101 cases treated surgically. Ann R Coll Surg Engl. 2007;89:272-75. [ Links ]
9. Azevedo et al. Tumours of the foot and ankle: a single institution experience. J Foot Ankle Sur. 2013;52:147-52. [ Links ]
10. Jougla E, Grolleau JL, Chavoin JP. Angioleiomyoma of the hand: a post traumatic tumor? Chir Main. 1999;18:216-19. [ Links ]
11. Sweeney J, Keating S. Angioleiomyoma. J Foot Surg. 1983;36:21 -22. [ Links ]
12. Tozzi M, Bodman M. Angioleiomyoma. J Am Med Assoc. 1978;68:823-25. [ Links ]
13. Tsoutsouris G. Vascular leiomyoma. J Foot Surg. 1982;21:37-41. [ Links ]
14. Murata H, Matsui T, Horie N, Sakabe T, Konishi E, Kubo T. Angioleiomyoma with calcification of the heel: report of two cases. Foot Ankle Int. 2007;28:1021-25. [ Links ]
15. Santucci A, Albini M, Ventura A, De Palma L. Clinical and histological features of vascular leiomyoma of the foot: case report and literature review. Foot Ankle Surg. 2000;6:267-74. [ Links ]
16. Blalock TW, Kerr C, DeRienzo DP, Greenway HT. Rare case of acral calcified angioleiomyoma with macroscopic calcium extrusion. Foot and Ankle Surgery. 2015;21:e36-39. [ Links ]
17. Yates BJ. Angioleiomyoma: Clinical Presentation and Surgical Management. Foot Ankle Int. 2001;22(8):670-74. [ Links ]
18. Katenkamp D, Kosmehl H, Langbein L. Langiomyome. Eine pathologische-anatomisch analyse von 229 fallen. Zentralb. Allg. Pathol. Anat. 1988;134:423-33. [ Links ]
19. Berlin SJ, Binder DM, Emiley TJ, et al. Leiomyoma of the foot. A review of the literature and report of cases. J Am Podiatr Med Assoc. 1976;66:450-58. [ Links ]
20. Genakos JJ, Wallace JA, Napoli AE, Pontarelli A, Terris A. Angioleiomyoma. A case report and literature review. J Am Podiatr Med Assoc. 1987;77:101-102. [ Links ]
21. Herren DB, Zimmermann A, Buchler U. Vascular leiomyoma in an index finger undergoing malignant transformation. J Hand Surg. 1995;20(B):484-87. [ Links ]
22. Kinoshita T, Ishii K, Abe Y, Naganuma H. Angiomyoma of the lower extremity: MR findings. Skelet Radiol. 1997;26:443-45. [ Links ]
23. Gajanthodi S, Rai R, Chaundhry RK. A rare differential diagnosis of extremity swelling. J Clin Diagn Res. 2013;7(3):571 -72. [ Links ]
24. Chavez-Lopez M, Reyna-Olivera G, Pedroza-Herrera G. Vascular leiomyoma of the foot: Ultrasound and histologic correlation. Reumatol Clin. 2014;10(5):342-43. [ Links ]
 Correspondence:
Correspondence:
Dr NT Nakale
Division of Orthopaedic Surgery
Wits Medical School, 7 York Road, Parktown, 2193;
Email: tn.nakale@gmail.com
Cell: +27728676140
Received: August 2016
Accepted: May 2017
Published: November 2017
Funding: None
Conflict of interest: No benefits of any form have been received from a commercial party related directly or indirectly to the subject of this article.
Editor: Prof Anton Schepers, University of the Witwatersrand


{kind=link}