










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.16 n.2 Centurion May./Jun. 2017
http://dx.doi.org/17159/2309-8309/2017/v16n2a3
SPINE
Ligamentous integrity in Spinal Cord Injury without Radiographic Abnormality (SCIWORA): a case series
A HornI; MI WorkmanII; S Dix-PeekIII; RN DunnIV, V
IMBChB(Pret), FC Orth(SA), MMed(UCT)Ortho, Consultant, Orthopaedic Surgery, Groote Schuur Hospital, Cape Town
IIBSc(Physio)(Wits), MBBCh(Wits) Registrar, Orthopaedic Surgery, Groote Schuur Hospital, Cape Town
IIIMBChB(UCT), FC Orth(SA), MMed(UCT)Ortho, Head of Paediatric Orthopaedic Services, Red Cross Children's Hospital and Maitland Cottage Home for Disabled Children, Cape Town
IVMBChB(UCT), FC Orth(SA), MMed(UCT)Ortho Consultant Spine and Orthopaedic Surgeon, Professor and Head of Department of Orthopaedic Surgery, University of Cape Town
VHead: Orthopaedic Spinal Services, Groote Schuur Hospital and Spinal Deformity Service, Red Cross Children's Hospital, Cape Town
ABSTRACT
PURPOSE OF STUDY: Prolonged bracing following injury in patients with Spinal Cord Injury without Radiographic Abnormality (SCIWORA) remains controversial. Some authors claim that there is occult instability and a risk of recurrent injury whereas others propose that the spinal column will deform elastically, but will return to its baseline stability by elastic recoil. We aim to assess the presence of ligamentous injury on MRI and the incidence of recurrent instability following SCIWORA in order to determine the need for prolonged bracing.
METHODS: A retrospective chart review was performed for a series of 12 patients with documented SCIWORA that presented to Red Cross Children's Hospital over the past 8 years. Details regarding mode of injury, age at presentation, neurological deficit at presentation, MRI findings and long-term prognosis were documented.
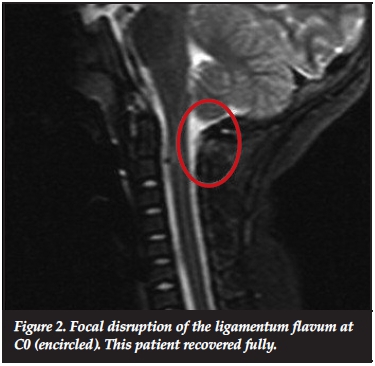
RESULTS: There were nine males and three females. The median age was 4.35 years. All patients were victims of high energy motor vehicle accidents. In two patients there was disruption of the ligamentum flavum at the level of the injury. There were no episodes of recurrent instability or neurological compromise in those patients that had recovered. None of our patients had rigid bracing following the diagnosis of SCIWORA.
CONCLUSION: Infrequently observed disruption of isolated stabilising structures in SCIWORA did not lead to early or delayed instability in our patients. We did not find evidence to support the practice of prolonged rigid bracing to prevent recurrence following SCIWORA.
LEVEL OF EVIDENCE: Prognostic case study, level IV.
Key words: SCIWORA, paediatric spinal cord injury, MRI findings in SCIWORA, bracing in SCIWORA, paediatric trauma
Introduction
The clinical entity of spinal cord injury without radiographic evidence of spinal column disruption has been recognised since the 1920s.1 The term SCIWORA (Spinal Cord Injury Without Radiographic Abnormality) was popularised by Pang and Wilberger in 19822 and was defined as 'objective signs of myelopathy as a result of trauma, whose plain films of the spine, tomography, and occasionally myelography carried out at the time of admission showed no evidence of skeletal injury or subluxation'.
The concept of occult spinal instability following SCIWORA remains a contentious subject among authors. Two conflicting theories exist. The 'Segmental Spinal Instability' theory states that, following SCIWORA, the injured spinal column is prone to re-injury, even in the absence of any objective clinical or radiographic features of instability, including MRI.2,3 The contradicting 'differential stretch hypothesis' is based on the fact that the inherently mobile paediatric spine will deform elastically under significant tension, exceeding the elastic deforming potential of the more fragile spinal cord, causing damage or rupture to the cord, but returning to baseline stability by elastic recoil.4 Proponents of the 'segmental spinal instability theory' recommend immobilisation of the affected spinal segment in a rigid brace for 12 weeks following injury, regardless of the presence of radiographic signs of instability.2,3 Those supporting the 'differential stretch hypothesis', on the other hand, recommend that protection in a soft collar for 2 weeks is sufficient and that bracing is unnecessary and does not prevent recurrence.*5
Rigid immobilisation of the spine, especially the cervical spine, is not without complications and is therefore best avoided if not indicated. The most common complication is pressure ulceration of the bony prominences of the head and neck. Rigid collars also interfere with nursing, feeding, oral care, central venous catheterisation and patient positioning in the severely injured child.6
The purpose of this study is to determine whether there was any evidence of injury to the paraspinal soft tissues on MRI in patients diagnosed with SCIWORA at our institution. We aim to provide objective evidence to support clinical practice, be it rigid immobilisation or not. The secondary aim was to gather data on demographics, clinical course, the incidence of recurrent injury, and other MRI findings in order to improve our understanding of the epidemiology and natural history of this condition.
Materials and methods
The Picture Archiving and Communication System (PACS) of our institution's radiology service was searched for patients with features of spinal cord injury (SCI) on MRI but no features of instability or injury on plain films or CT scan. The hospital records of these patients were obtained and data collected regarding demographic details, mode of injury, presenting complaint, X-ray and MRI findings, in-hospital management, and neurological recovery.
The presence of recurrent neurological complaints following resolution of the original injury was specifically sought for.
The plain films and MRI scans were reviewed by senior radiologists at our institution as well as by one of the authors (AH) for evidence of soft tissue injury or spinal instability. Spinal instability was defined as an increase beyond the normal limit of the atlanto-dens interval (<3.5 mm) on plain films. Soft tissue swelling was similarly defined as a retropa-harangeal shadow exceeding 6 mm at the level of C3 and 14 mm at the level of C6.
Standard T1- and T2-weighted MRI sequences were performed on all patients. Specific soft-tissue sequences were not routinely performed and are therefore not reported on in this review.
Due to the small cohort identified, meaningful statistical analysis was not feasible. We therefore report on descriptive statistics only.
Results
The demographic details are summarised in Table I.
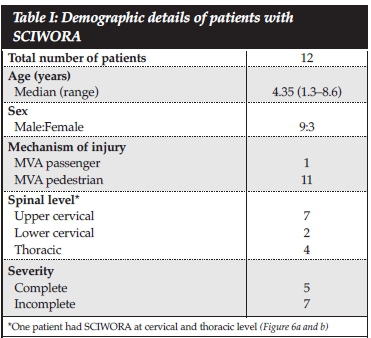
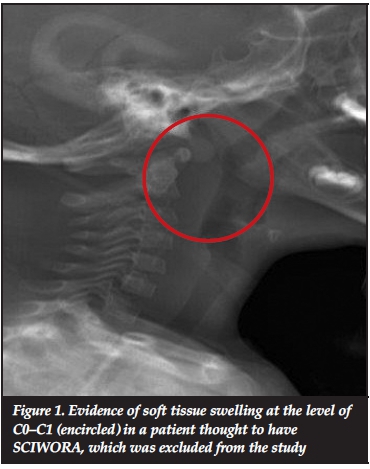
Thirteen patients with a diagnosis of SCIWORA for the years 2006-2014 were identified. One patient was found to have soft tissue swelling on cervical spine X-rays (Figure 1) and was excluded on the grounds that the injury was not technically a SCIWORA. Of the remaining 12 patients, nine were male, all were aged 8 years or younger and all were victims of high energy motor vehicle accidents (MVAs). All the patients in our series presented with significant neurological deficit.
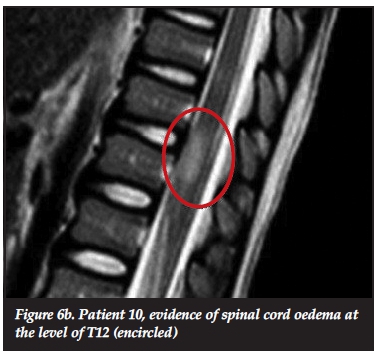
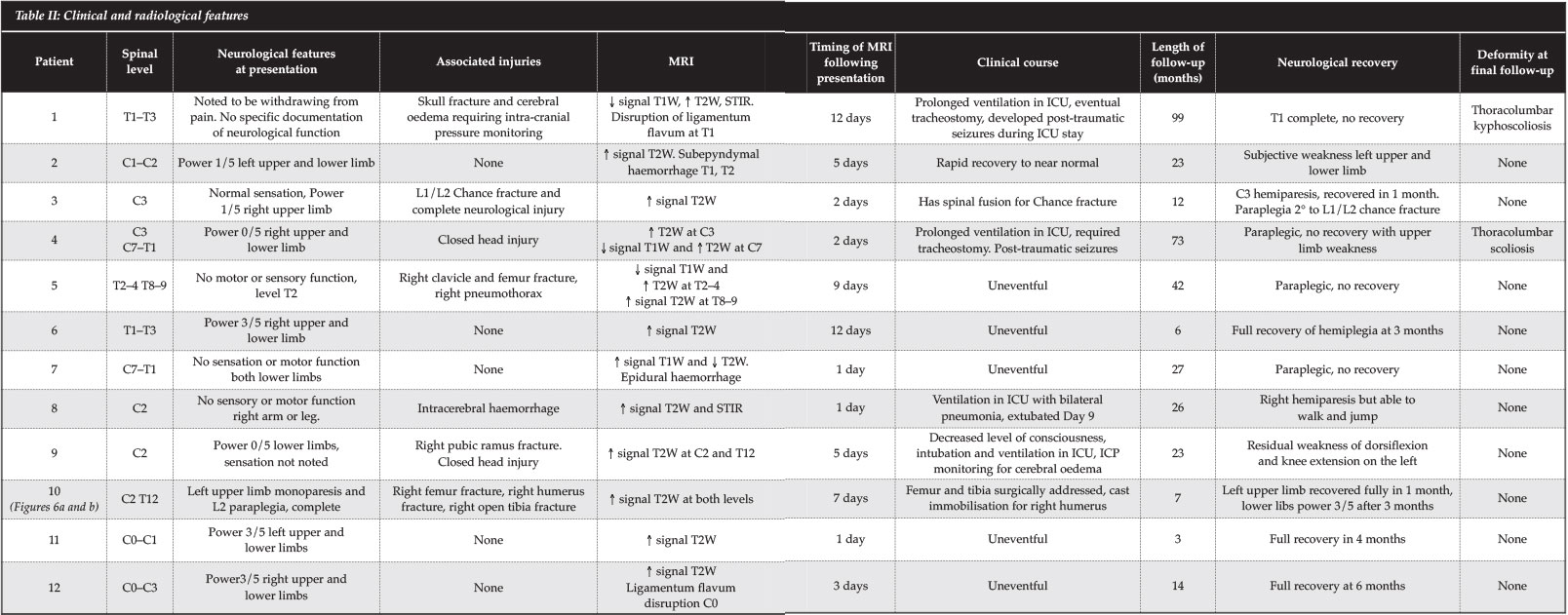
Details of clinical and radiological findings at presentation and follow-up, as well as clinical course, are summarised in Table II.
No evidence of spinal instability was identified on reviewing the available X-rays. MRI was performed on all our patients. In two patients, focal disruption of the ligamentum flavum at the level of the injury (Figures 2 and 3) was noted.

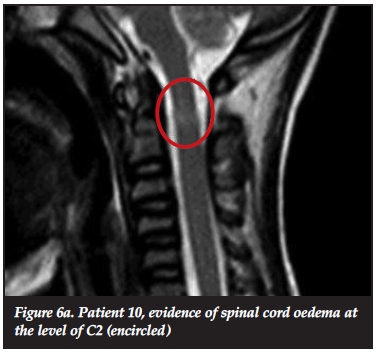
There was no evidence of soft tissue swelling, ligamentous disruption or spinal instability in the other patients. The MRI findings are summarised in Table II. All patients had hyperintense lesions on T2W series (Figure 4), only five had hypointense lesions on T1W series (Figure 5, red arrow). Four patients had evidence of epidural bleeds on either T1W or T2W series. Patients with changes on T1W series consistently had complete injuries and no neurological recovery, whereas those with T2W signal change only, demonstrated partial or full recovery at a median follow-up of 51 months (range 3-99 months).


None of the patients had rigid spinal immobilisation following their injury. Patients with C-spine lesions were treated in a soft collar for two weeks, those with thoracic lesions were treated with bed rest until able to mobilise with the assistance of a physiotherapist. No recurrent injuries were reported in those patients who had recovered from the initial injury. One patient was documented to be 'withdrawing from pain' on admission, suggesting intact motor function, but was later found to be paraplegic (patient 1). The initial neurological examination in this patient was perfunctory to say the least, as there were significant distracting injuries for which the patient required prolonged ICU admission and ventilation. The paralysis was only noted several days after admission. Whether this represents neurological deterioration or a missed injury is uncertain.
The use of corticosteroids in acute spinal cord injury is not routine at our institution and none of our patients received steroids as treatment for their spinal cord injury.
Discussion
Demographics of SCIWORA
Although SCIWORA has been described in adults, it is much more common in children, and depending on the criteria used, accounts for 19-34% of paediatric spinal cord injury.7 Several factors predispose the paediatric population to the development of SCIWORA and are generally agreed upon. The paraspinal soft tissues in a paediatric patient are more elastic and therefore more prone to significant distraction than in the adult spine. This includes joint capsules, paraspinal ligaments and intervertebral discs.2-5,7 Bony stability is also reduced compared to the adult spine due to shallow, more horizontally oriented facet joints, absent uncinate processes and anterior wedging of the vertebral bodies.3 Lastly, due to the relatively large head in the paediatric population, the cervical spine is subjected to greater bending forces during flexion and extension, placing it at greater risk for more severe injuries.3-5
As the paediatric spine assumes adult morphology around the age of 8 years,5 the incidence of SCIWORA decreases and children start exhibiting adult-type injuries such as fractures and dislocations. In our series, all the patients were younger than 8 years of age. Most authors agree that children under the age of 8 have more severe injuries and worse prognosis,2,3,6-8 which is in keeping with our study findings. The mean age of patients with complete injuries in our study was 2 years, and for those who had incomplete injuries it was 6.1 years.
In the infant and very young child, the fulcrum for maximum flexion is at the level of C2-3,3 predisposing this younger population to higher cervical injuries. This, by its very nature, explains the worse prognosis in this group of patients, as survival potential is extremely low with such a high injury. In the older age group, the fulcrum of maximal flexion is at the level of C5-6, the same as in adults. In our series, the more severe complete neurological injuries were seen in the younger patients, but interestingly, the average age for high cervical injuries was higher than for low cervical and thoracic injuries (5.8 years vs 2 years).
Occult instability and the need for immobilisation
The question of occult instability following SCIWORA and the need for prolonged bracing remains contentious. Several studies have been published citing series of patients who were seemingly normal following an injury to the spine and then subsequently, following relatively minor trauma, developed progressive neurology or a recurrence of the injury.3,7,9 The time from initial injury to 'recurrent injury' ranged from a few days to several months or even years. On closer examination of these cases, the majority occurred in patients older than 8 years of age, followed minor trauma such as sporting injuries, and symptoms were mild and transient both on initial and subsequent presentation. In the very few patients in whom the recurrent injury led to severe, permanent neurological deficit, the possibility of an alternative diagnosis, such as acute transverse myelitis, was often considered but never excluded.3,6,7
An alternative explanation for the phenomenon of recurrent or delayed presentation, SCIWORA is the well understood progressive nature of spinal cord injuries. Several inflammatory mediators such as arachidonic acid and glutamate cause progressive lipid peroxidation and cell membrane destruction in the injured spinal cord, gradually causing expansion of the zone of injury.10
In a recent comprehensive literature review by Rozelle et al.,11 no compelling evidence could be found to suggest that any patient developed delayed instability when initial dynamic studies were normal. Furthermore, even in the presence of paraspinal soft tissue injury on MRI, no patient demonstrated early or delayed instability. The author's recommendation, graded as level III evidence, was 2 weeks' immobilisation in a soft collar for patients with normal initial studies, including somatosensory evoked potentials, and 3 months' rigid immobilisation for all other patients.
In our study, patients were included based on an MRI diagnosis of SCIWORA, which naturally excluded those with normal MRI findings. Only two of the 12 patients had evidence of paraspinal soft tissue injury on MRI and no patient developed recurrent neurological symptoms or signs following resolution of the initial injury. Flexion-extension films were not performed routinely to demonstrate occult instability, and until now has not been indicated. Two patients (patients 1 and 4) in this study developed spinal deformity during the follow-up period. In both cases the deformity appeared to be as a result of paralysis and was below the level of the spinal cord injury. It is likely that more patients will demonstrate the development of deformity associated with paralysis with longer follow-up.
Our findings support the differential stretch theory as proposed by Bosch et al.* and Gore et al.5There is a wide spectrum of injury in spinal cord trauma, and certainly there are instances where instability is indeed a feature. However, in the absence of evidence of instability, either on plain films or CT, there appears to be no indication for immobilisation of the spine based on this series and other series reported in the literature.4
MRI findings
The description of the clinicoradiologic mismatch that is SCIWORA predates the age of MRI and therefore does not include MRI abnormalities. There has been much debate about the relevance of the term SCIWORA in an age where MRI is readily available and often performed as initial investigation in patients with spinal injuries. Several alternatives have been suggested, such as SCIWORET (SCI without radiographic evidence of trauma), SCIWOCTET (SCI without CT-evidence of trauma)12 or SCIWONA (SCI without neuroimaging abnormality),13 which may be a more accurate and relevant description of this particular injury.
Three different types of injuries, as seen on MRI, have been described in SCIWORA (Table III): complete transection of the cord; haemorrhage, either intra- or extraspinal; and cord oedema.3,14 Complete transection carries the worst prognosis, and neurological deficit will be complete and irreversible.
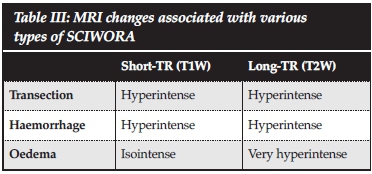
Intraspinal haemorrhage also carries a poor prognosis and patients will not recover function beyond what they initially present with. Small extraspinal haemorrhages and isolated cord oedema are associated with a better prognosis and patients usually demonstrate full or nearly full recovery.12 This prognostic value of early MRI was confirmed in our study. T2-weighted images have the best prognostic value for closed spinal cord injuries and are excellent at demonstrating disc, capsular and muscle injuries.12 Although the short tau inversion recovery (STIR) method is preferred to detect subtle cord oedema in spine injured patients,14 not all of our patients had this sequence performed and we therefore did not report on it.
In our patients, MRI was often performed several days (median 7.5 days, range 1-12) following the initial injury. Plain radiography and CT remain the primary investigations performed for acute spinal cord injury as MRI is a relatively scarce and expensive resource. Therefore, we believe the term SCIWORA does still have some clinical relevance in countries with limited resources. The authors also believe that SCIWORA, as originally defined, and as represented in our series, describes an injury pattern that does not compromise spinal stability but may have significant neurological consequences.
The limitations of this study include the small cohort, the retrospective nature of the study and our chosen method of identifying candidates. Systematic and detailed neurological examination was therefore either not performed or not properly documented, neither at presentation nor at most recent follow-up. Our institution only treats patients of 12 years and younger, therefore excluding the older population from our database. We do however propose that our small population represents SCIWORA under the strictest definition, and therefore our results may well be extrapolated to the paediatric population at large.
Conclusion
Once SCIWORA has occurred, there is little that can be done to alter the natural history of the injury. It is however prudent to determine whether our treatment has any value and of course, to be able to predict the prognosis in order to inform and counsel our patients and their families adequately. Based on our findings and a review of the current literature, we did not find convincing evidence to support the practice of prolonged, rigid immobilisation following SCIWORA. We also conclude that the neurological prognosis can be formulated on the basis of the MRI features at presentation, as well as the severity of the initial injury.
Compliance with ethical guidelines
No funding was received for the execution of this study. Ethical approval was granted by our institutional human research ethics committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Disclosure: The content of this article is the sole work of the authors. No benefits of any form have been or are to be received from a commercial party related directly or indirectly to the subject of this article.
Author identifying information: Author AH has received no research funding and has no conflicts of interest to declare.
Authors MW, SDP RND have no conflicts of interest to declare.
References
1. Crothers B. Injury of the spinal cord in breech extraction as an important cause of foetal death and paraplegia in childhood. Am J Med Sci 1923;94-110. [ Links ]
2. Pang D, Wilberger J. Spinal cord injury without radiographic abnormality in children. J Neurosurg 1982;57:114-29. [ Links ]
3. Pang D. Spinal cord injury without radiographic abnormality, 2 decades later. Neurosurgery 2004;55(66):1325-43. [ Links ]
4. Bosch PP, Vogt MT, Ward WT. Pediatric Spinal Cord Injury without Radiographic Abnormality (SCIWORA): The absence of occult instability and lack of indication for bracing. Spine 2002;27(24):2788-2800. [ Links ]
5. Gore PA, Chang S, Theodore N. Cervical spine injuries in children: attention to radiographic differences and stability compared to those in an adult patient. Semin Pediatr Neurol 2009;16:42-58. [ Links ]
6. Scott TE, Coates PJB, Davies SR, et al. Clearing the spine in the unconscious patient: an update. Journ Int Care Soc 2002;13(3):227-31. [ Links ]
7. Buldini B, Amigoni A, Faggin R, et al. Spinal cord injury without radiographic abnormalities. Eur J Pediatr 2006;165:108-11. [ Links ]
8. Kalra V, Gulati S, Mahesh K, et al. SCIWORA- Spinal Cord Injury Without Radiological Abnormality. Indian J Pediatr 2006;73(9):829-31. [ Links ]
9. Pollack IF, Pang D, Sclabassi R. Recurrent spinal cord injury without radiographic abnormalities in children. J Neurosurg 1988;69:177-82. [ Links ]
10. Bydon M, Lin J, Macki M, et al. The current role of steroids in acute spinal cord injury. World Neurosurg. 2014. http://dx.doi.org /10.1016/j.wneu.2013.02.062 [ Links ]
11. Rozelle CJ, Aarabi B, Dhall S, et al. Spinal cord Injury Without Radiographic Abnormality (SCIWORA). Neurosurgery 2013;72(2):227-33. [ Links ]
12. Dreisen D, Kim W, Kim JS, et al. Will the real SCIWORA please stand up? Exploring clinicoradiologic mismatch in closed spinal cord injuries. Am J Radiol 2015;205:863-60. [ Links ]
13. Yucesoy K, Yuksel KZ. SCIWORA in the MRI era. Clin Neurol Neurosurg 2008;110:429-33. [ Links ]
14. Szwedowski D, Walecki J. Spinal Cord Injury Without Radiographic Abnormality (SCIWORA) - clinical and radiological aspects. Pol J Radiol 2014;79:461-64. [ Links ]
 Correspondence:
Correspondence:
Dr Anria Horn
Postnet Suite 342
Pvt Bag X18 7701
Rondebosch , South Africa
Tel: +27 (0)21 404 5108
Fax: +27 (0)21 447 2709
Email: anriahorn@gmail.com


{kind=link}