










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.16 no.2 Centurion Mai./Jun. 2017
http://dx.doi.org/10.17159/2309-8309/2017/v16n2a2
PAEDIATRICS
Assessment of emotional distress and parenting stress among parents of children with clubfoot in south-western Nigeria
O EsanI; A AkinsuloreII; MB YusufIII; OO AdegbehingbeIV
IMBChB, FWACS, FMCS(Ortho) Senior lecturer, Department of Orthopaedic Surgery and Traumatology, Obafemi Awolowo University, Ile-Ife, Nigeria
IIMBChB, MPH, FWACP, FMCPsych, Senior lecturer, Department of Mental Health, Obafemi Awolowo University, Ile-Ife, Nigeria
IIIMBChB, FWACS Consultant orthopaedic surgeon, Department of Surgery, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria
IVMBChB, FMCS(Ortho) Associate professor, Department of Orthopaedic Surgery and Traumatology, Obafemi Awolowo University, Ile-Ife, Nigeria
ABSTRACT
BACKGROUND: Clubfoot, the commonest orthopaedic congenital deformity in the tropics, is usually recognised from birth and affects one or both feet. The discovery of the child's deformity may diminish the joy of childbirth with attendant emotional reactions. Hence, this study assessed the levels of emotional distress and parenting stress among parents of children with clubfoot in Nigeria.
METHODOLOGY: This was a cross-sectional study conducted among 58 parents of children with clubfoot attending the clubfoot clinic of a tertiary health institution in Nigeria. They completed a socio-demographic questionnaire, the Hospital Anxiety and Depression Scale (HADS) and Parenting Stress Index Short Form.
RESULTS: The prevalence of emotional distress and parenting stress were 15.5% and 12.0% respectively. The mean score of parenting stress and its subscales were 67.44 (SD=18.07); parental distress 26.71 (SD=8.82); parents-child dysfunctional interaction 19.13 (SD=5.91) and difficult child 21.60 (SD=7.19). The patient age group was significantly associated with emotional distress level (x2=13.566, p=0.004). Pearson's correlation showed significant positive correlation between parental stress and the patient's age (r=0.277, p<0.05) and HADS depression score (r= 0.290, p<0.05).
CONCLUSION: This study has provided relevant information on the experiences of Nigerian parents caring for children with clubfoot. Health care professionals involved with the care of children with clubfoot should also pay attention to the emotional wellbeing of the parents.
Key words: clubfoot, emotional distress, parenting stress, Nigeria
Introduction
Clubfoot or congenital talipes equinovarus (CTEV) is the most common orthopaedic congenital deformity of the lower limb seen in the tropics.1,2 The diagnosis of clubfoot is usually made at birth but it can be detected in the third trimester of pregnancy using ultrasound. Clubfoot affects one or both feet, and males are more affected than females.3 The incidence of clubfoot in studies from the developed countries ranges from 1.1 to 2.57 per 1 000 births.4
In the Eastern part of Africa, the incidence was estimated to be up to 2 per 1 000 births5 while among black South Africans, it was reported to be 3.5 per 1 000 births.6 In Nigeria, the incidence was estimated to be 3.4 per 1 000 births.7
The birth of a baby is a major life event for parents, and in the south-western part of Nigeria it is a celebrated event. After first observing the baby's deformed limb, parents are initially shocked and then tend to experience emotional distress characterised by mood disturbances such as anxiety, depression, anger and fearfulness.8,9 The obvious deformity of clubfoot makes the child's foot a source of worry for most parents. Before commencement of treatment, parents tend to worry about the diagnosis, the long-term functioning of the child, treatment availability, selection of the treatment and competing sources of information.
The process of managing a child with clubfoot involves diagnosis, treatment and follow-up. This process is obviously emotionally charged, resulting in high levels of stress for parents.10 Furthermore, caring for a child with clubfoot is also very stressful for many parents as a result of increased demands for their time and energy as well as worries about the functional future of the child.11 Thus, parents have to cope with the emotional aspect of the child's treatment. Mothers, given their traditional family roles, usually take up more of the emotional and practical responsibility of caring for the child.12 To achieve a good treatment outcome in a patient with clubfoot, it is imperative that parents are active members of the managing team. However, a very important barrier or factor to becoming an active member of the managing team is the parent's emotional state. An earlier study conducted among mothers of children with clubfoot reported a negative impact of the diagnosis of clubfoot on their psychological well-being.13
To this end, we set out to determine the levels of emotional distress and parenting stress among parents of Nigerian children with clubfoot and identify associated risk factors. Furthermore, in Nigeria there is a dearth of research undertaken to assess the experiences of parents of children with clubfoot. Therefore, this study examines the experiences of parents caring for a child with clubfoot with the intention of utilising the findings to develop a better and more effective service for these families.
Methodology
Setting and sample
The cross-sectional study was conducted over a period of two years (July 2013-June 2015) in Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC), Ile-Ife, a tertiary hospital in south-western Nigeria. Study participants were parents of children with clubfoot attending the clubfoot clinic of the hospital and were undergoing the Ponseti method of clubfoot treatment. This centre has personnel that have undergone training in the Ponseti method of clubfoot treatment. Inclusion criteria were: being a parent of a child with clubfoot receiving treatment for the clubfoot. Parents with a history of mental illness and with a child with other additional congenital abnormalities were excluded from the study.
Procedure and assessment
The study protocol was approved by the Ethics and Research Committee of the institution. Written informed consent was taken from all the parents after the objectives of the study had been explained to them. The respondents were assessed using the following questionnaires:
• Socio-demographic characteristics: This questionnaire was designed specifically for this study and elicited information such as age, gender, relationship to child and other related data.
• Hospital Anxiety and Depression Scale (HADS): This was developed to assess anxiety and depressive symptoms among non-psychiatric patients in the hospital.14 The instrument consisted of seven questions each for both anxiety and depression. The scales are rated on a four-point scale ranging from 0-3. A cut-off point of 8 and above in either the anxiety or depressive subscale indicates depression or anxiety. We categorised the respondents in this study into two groups based on their scores in the HADS. Respondents with a score of 8 and above in either or both of the HADS subscales were considered to have emotional distress. Those with scores of less than 8 in both subscales were considered to be normal.
• Parenting Stress Index Short Form (PSI-SF): Parenting stress was assessed using the PSI-SF15 which is a self-reported questionnaire with 36 questions rated on a five-point Likert scale ranging from 1-5. It has three subscales: parental distress (PD), which measures impaired sense of competence in the parenting role; parents-child dysfunctional interaction (PCDI), which assesses the failure of the child to meet their parents' expectation; and difficult child (DC), which examines the characteristics of the child that makes them easy or difficult to manage. Each of the three subscales consists of 12 items with scores ranging from 12-60. The total stress score is the sum of the three subscales which can range from 36-180. A total parenting stress score between 36 and 55 is said to be a low level of stress; between 56 and 85 is normal stress; between 86 and 90 is a high level of stress; and above 90 is said to be a clinically significant stress level.
Statistical analysis of data was done using the SPSS version 20 software for Windows. Descriptive statistics were calculated as frequencies, percentages and means. The chi-square test and independent t-test was used to test for associations. Correlations between parents' and patients' age, depression, anxiety and parenting stress were studied using Pearson's product moment correlation coefficient. The level of significance was considered to be a p-value less than 0.05.
Results
A total of 58 parents were recruited into the study. Table I shows the socio-demographic variables of parents of patients with clubfoot. The mean age of the parents was 31.10 years (SD=6.22) with the majority between 26 and 35 years (62.1%). Mothers constituted 82.8% with a male to female ratio of 1:5. Most of the respondents (86.3%) had at least secondary education. Among the patients with clubfoot, most of them were males (70.7%) with a male to female ratio of 2.4:1.
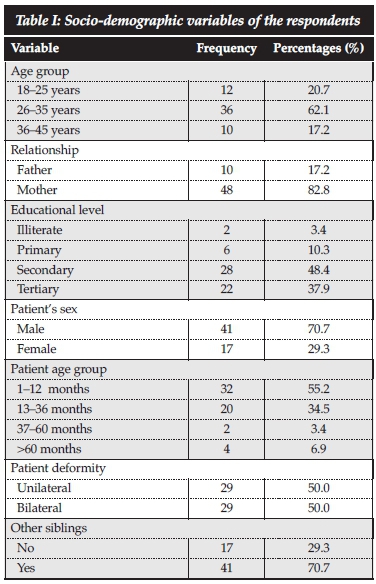
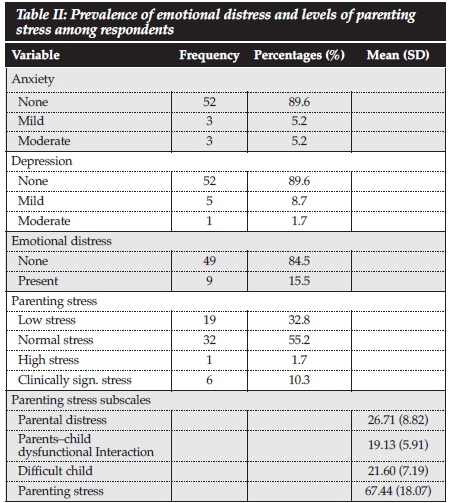
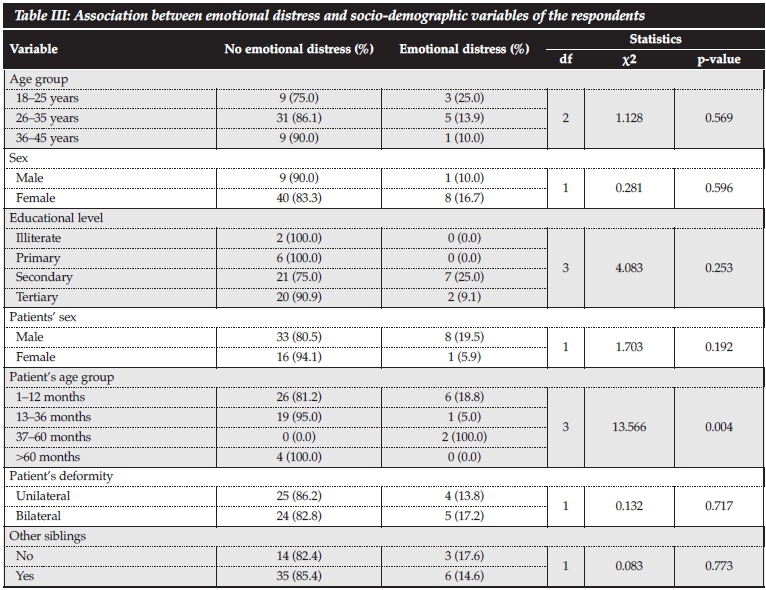
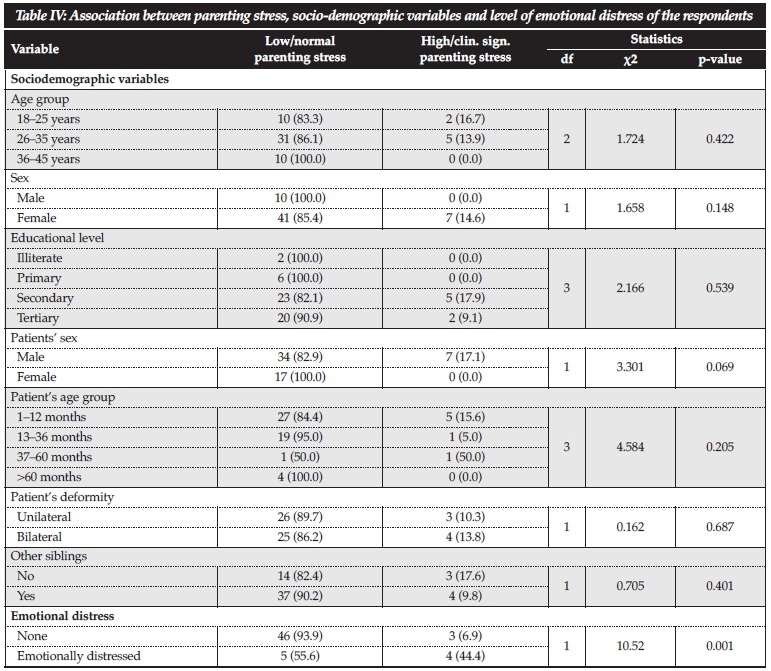
The mean age of patients was 18.43 months (SD=22.26) with most of them presenting in the first 12 months of life (55.2%). Half (50%) had bilateral clubfoot, and the majority of patients (70.7%) had siblings. In Table II, emotional distress based on the HADS scores was found among nine (15.5%) parents. This consisted of anxiety (n=6; 10.4%), depression (n=6; 10.4%) and co-morbid anxiety-depression (n=3; 5.2%) among the parents. Parenting stress based on PSI-SF scores was found among seven (12.0%) parents with one (1.7%) having high stress and six (10.3%) clinically significant stress. The mean score of parenting stress was 67.44 (SD=18.07) while the score for the subscales were: parental distress 26.71 (SD=8.82); parents-child dysfunctional interaction 19.13 (SD=5.91); difficult child 21.60 (SD=7.19). The association between emotional distress, parenting stress and socio-demographic variables of the parents is shown in Tables III and IV. A test of association between level of emotional distress among parents and their socio-demographic variables showed that only the patients' age group (x2=13.566, p=0.004) was significantly associated with emotional distress levels.
Pearson's correlation between parents' and patients' age, HADS score and parenting stress and its subscales showed significant positive correlation between parental stress and the patients' age (r=0.277, p<0.05) and HADS depression score (r= 0.290, p<0.05). There was also significant positive correlation between parenting stress score and HADS depression scores of parents (r=0.285, p<0.05) (Table V).
Discussion
The study of emotional distress and parenting stress associated with caring for children with clubfoot in a tertiary hospital is a pioneering effort in Nigeria. There are few studies in the literature on the experiences of parents of children with clubfoot.8,13 However, research focusing on the experiences of parents/caregivers of patients with chronic diseases in the clinical setting is increasing.16-19 This study assessed emotional distress and parenting stress associated with caring for children with clubfoot using HADS and PSI-SF in which nine (15.5%) parents reported emotional distress and seven (12.0%) had parenting stress. The majority of parents in this study were mothers and this is understandable as it is a common tradition that women are saddled with the duties of care for their children in the family. Since most of the patients were infants, they were dependent on their mothers for feeding and other care.
The mean age of the caregivers was 31.10 years (SD=6.22) with the majority between 26 and 35 years of age (62.1%). Most of the parents in this study were in their most productive age range. This implies that the caregiving role of parents, especially mothers, may interfere with their effectiveness at work, leading to reduced or loss of productivity with significant economic impact on the family.
Most of the patients were male children and this finding is similar to previous studies that reported male preponderance in clubfooted babies.3,7 This study also reported that 50% of children with clubfoot had it bilaterally, which is in contrast with findings of a study conducted in southeast Nigeria that reported that 60% of clubfoot cases are bilateral.7
The prevalence of emotional distress in this study was 15.5% which is relatively low when compared with the prevalence of 65.7% reported among caregivers of patients with epilepsy in the northern part of Nigeria using a similar questionnaire.16 The prevalence of high/clinically significant parenting stress was 12.0%, and the level of parenting stress was highest for parental distress and lowest for parent-child dysfunctional interaction. Since clubfoot is a non-life threatening birth defect without any associated pain in the child's limb, some parents may not really worry. In addition, some of the patients and caregivers started assessing care during the period of data collection which might explain the low level of emotional distress and parenting stress observed in this study. Another possible explanation is that some parents have access to the internet where they were able to obtain information about the management of clubfoot.
In this study, emotional distress was significantly associated with a patient's age in the range of 3-5 years. A possible explanation for this observation is that this is the period when the child is expected to leave the home (such as when commencing schooling) and mix with other children outside the home. However, the obvious deformity of clubfoot makes it embarrassing and emotionally distressing to the parents. This study has shown that parents of patients with clubfoot experience emotional distress as well as parenting stress as a result of caring for their children. The attendant discomfort of having a child with obvious deformity could be responsible for the association between emotional distress and parenting stress. In this study, increasing age of patients was related to greater severity of parental distress experienced by parents of children with clubfoot. This implies that older parents were more vulnerable to parenting stress than younger ones. Similarly, increased severity of depression symptoms as measured by HADS was related to increased severity of parental distress as well as increased severity of parenting stress.
The findings of this study should be interpreted in the context of some limitations. This study assessed the cross-sectional association between child characteristics, parenting stress and emotional distress; thus causality cannot be implied. Therefore, research with a longitudinal approach is required to clarify if parenting stress and emotional distress are actually caused by the child's problem. Moreover, a self-reported questionnaire was used which was based on parents' subjective assessment of their condition. Despite these limitations, the strength of the study lies in the use of a standardised instrument to measure parenting stress and emotional distress.
In conclusion, this study has provided relevant information on the experiences of Nigerian parents caring for children with clubfoot. The results of this study highlight that parents of children with clubfoot experience low levels
of emotional distress and parenting stress. However, there is need for psychological support for parents of children with clubfoot. It is important that the health professionals involved with the care of children with clubfoot pay attention to the emotional needs of the parents so as to reduce associated emotional distress and parenting stress.
Compliance with ethical guidelines
I, A Akinsulore, hereby declare that this article is the origianl work of the co-authors and myself. This article has never been published and is submitted exclusively to the South African Orthopaedic Journal for publication.
All the authors have no conflict of interest and have received no commercial benefits of any kind for the writing of this article. The study protocol was approved by the Ethics and Research Committee of our institution. Written informed consent was taken from all the parents after the objectives of the study had been explained to them.
References
1. Omololu B, Ogunlade SO, Alonge TO. Pattern of congenital musculoskeletal malformations in an African teaching hospital. West African Journal of Medicine 2005;24(2):92-95. [ Links ]
2. Orimolade EA, Adepiti AE, Ikuomola AA, Ige OO. Congenital anomalies in a state specialist hospital: A secondary level of healthcare. East and Central Africa Journal of Surgery 2014;19(2):44-48. [ Links ]
3. Chesney D, Barker S, Macnicol MF, Porter RW, Maffulli N. Management of congenital Talipes Equinovarus in Scotland: a nationwide audit. Journal of the Royal Colleges of Surgeons of Edinburgh and Ireland 2004;2:47-51. [ Links ]
4. Barker S, Chesney D, Miedzybrodzka Z, Maffulli N. Genetics and epidemiology of idiopathic congenital talipes equinovarus. Journal of Paediatric Orthopaedics 2003;23:265-72. [ Links ]
5. Mkandawire N, Kaunda E. Incidence and patterns of congential talipes equinovarus (clubfoot) deformity at Queen Elizabeth Central Hospital. East and Central African Journal of Surgery 2004;2:2-31. [ Links ]
6. Ballantyne J A, Macnicol, M F. Congenital talipes equino- varus (clubfoot): an overview of the aetiology and treatment. Mini-symposium: The paediatric foot. Current Orthopaedics 2002;16:85-95. [ Links ]
7. Ukoha U , Egwu OA , Okafor IJ , Ogugua PC , Udemezue OO , Olisah R , Anyabolu AE incidence of congenital talipes equinovarus among children in southeast Nigeria. International Journal of Biological and Medical Research 2011;2(3):712-15. [ Links ]
8. Pietrucin-Materek M, van Teijlingen ER, Barker S, Keenan KF, Miedzybrodzka Z. Parenting a child with clubfoot: A qualitative study. International Journal of Orthopaedic and Trauma Nursing 2011;15:176-84. [ Links ]
9. Goldbeck L. The impact of newly diagnosed chronic paediatric conditions on parental quality of life. Quality of Life Research 2006;15:1121-31. [ Links ]
10. Skari H, Malt UF, Bjornland K, Egeland T, Haugen G, Skreden M, et al. Prenatal diagnosis of congenital malformations and parental psychological distress- a prospective longitudinal cohort study. Prenatal Diagnosis 2006;26:1001-1009. [ Links ]
11. Wallander JL, Venters TL. Perceived role restriction and adjustment of mothers of children with chronic physical disability. Journal of Paediatric Psychology 1995;20:619-32. [ Links ]
12. Quittner AL, Espelage DL. Opipari LC, Carter B, Eid N, Eigen H. Role strain in couples with and without a child with a chronic illness: Associations with marital satisfaction, intimacy, and daily mood. Health Psychology 1998;17:112-24. [ Links ]
13. Coppola G , Costantini A, Tedone R, Pasquale S, Elia L, Barbaro MF, d'Addetta I. The impact of the baby's congenital malformation on the mother's psychological well-being: an empirical contribution on the clubfoot. Journal of Paediatric Orthopaedics 2012;32(5):521-26. [ Links ]
14. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica 1983;67:361-70. [ Links ]
15. Abidin RR. Parenting Stress Index, Psychology Press, Odessa 1995. [ Links ]
16. Yusuf AJ, Nuhu FT, Olisah VO. Emotional distress among caregivers of patients with epilepsy in Katsina State, Northern Nigeria. African Journal of Psychiatry 2013;16:41-44. [ Links ]
17. Feizi A, Najmi B, Salesi A, Chorami M, Hoveidafar R. Parenting stress among mothers of children with different physical, mental, and psychological problems. Journal of Research in Medical Sciences 2014;19(2):145-52. [ Links ]
18. Larson NC. Parenting stress among adolescents mothers in the transition to adulthood. Child and Adolescent Social Work Journal 2004;21(5):457-75. [ Links ]
19. Leung C, Leung S, Chan R, Tso T, Ip F. Child behaviour and parenting stress in Hong Kong families. Hong Kong Medical Journal 2005;11:373-80. [ Links ]
 Correspondence:
Correspondence:
Dr Adesanmi Akinsulore
Department of Mental Health Obafemi Awolowo University Ile-Ife
Osun State, Nigeria
Phone: +2348033968554
Email: sanmilore@gmail.com


{kind=link}
{kind=link}
{kind=link}