










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.15 n.1 Centurion Mar./Apr. 2016
http://dx.doi.org/10.17159/2309-8309/2016/v15n1a9
TRAUMA
Changes in short-term cognitive function following a hip fracture in the elderly and the effect of cognitive function on early post-operative function
S AdamI; L GodlwanaII; D MalekaIII
IBSc Physio, MSc Physio(Wits); Physiotherapy Department, Faculty of Health Sciences, University of the Witwatersrand, South Africa
IIBSc Physio(UCT), MSc Physio, PhD(Wits); Physiotherapy Department, Faculty of Health Sciences, University of the Witwatersrand, South Africa
IIIBSc Physio, MPH, PhD(Wits); Physiotherapy Department, Faculty of Health Sciences, University of the Witwatersrand, South Africa
ABSTRACT
OBJECTIVE: To evaluate the changes in short-term cognitive function and the relation between cognition and early post-operative functional outcome in the elderly following a hip fracture
DESIGN: Prospective pre-test-post-test observational study
SETTING: Two public hospitals in Johannesburg, South Africa
PARTICIPANTS: Ninety elderly patients with a first time unilateral hip fracture over the age of 60 years were consecutively sampled. Patients with polytrauma and those with co-morbidities affecting mobility (stroke, Parkinson's disease or a spinal cord injury) were excluded. Patients re-admitted with complications of a previous surgery or those managed conservatively were also excluded. Seventy-two participants completed the study
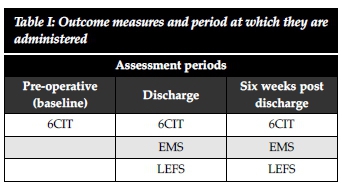
DATA COLLECTION: Pre-operative (baseline), discharge and six weeks post discharge assessments were carried out. Cognitive function was established using the Six-Item Cognitive Impairment Test (6CIT) at each of the three assessment periods. The participants' post-operative functional level was assessed using the Elderly Mobility Scale (EMS) and the Lower Extremity Functional Scale (LEFS) at discharge and at six weeks post discharge
RESULTS: This study revealed significant advances in cognition from baseline to six weeks post discharge (z-statistic -5.04, p=0.000). After adjusting for pre-fracture functional mobility and pre-existing co-morbidities, a multivariate regression analysis revealed that cognitive function is also a strong predictor of early post-operative functional outcome (β= -0.14, p=0.036
CONCLUSION: Cognitive function in elderly individuals with a hip fracture does improve over time. Cognitive function is a strong predictor of early post-operative functional outcome, when adjusted for pre-fracture functional mobility and pre-existing co-morbidities
Key words: hip fracture, elderly, cognitive function, early post-operative functional outcome, Six-Item Cognitive Impairment Test
Introduction
Hip fracture is a common, serious injury that occurs predominantly in the elderly.1 Hip fractures are a major cause of morbidity and mortality and occur in 20% to 30% of older people who fall.2
Cognitive function has been reported to be an important prognostic factor associated with rehabilitation success of older patients with a hip fracture. Impaired cognitive function may negatively affect functional recovery in disabled elderly patients with a hip fracture.3 Elderly patients with a hip fracture who present with cognitive impairments and depressive symptoms have poorer rehabilitation outcomes, which is due to poor participation during therapy.4
There are no studies available in South Africa that have evaluated the changes in short-term cognitive function, from a pre-operative state to discharge and six weeks post discharge, and the relation between cognition and early post-operative functional outcome in the elderly following a hip fracture prior to this study. The aim of this study was to establish these changes in cognitive function and determine the relation between cognitive function and the early post-operative functional outcome in elderly patients with a hip fracture.
Determining the effect of cognitive function on early post-operative functional outcome in elderly patients with a hip fracture in a selected public health setting in South Africa will help identify those patients who are especially at risk of not regaining independence in basic mobility. Evaluating the changes in cognitive function over time will assist practitioners in understanding elderly patients and exploring how best to motivate these patients, thus attempting to improve the medical management of these patients.
Method
Study design
A prospective pre-test-post-test observational study was conducted. Details of the study design are mentioned in the procedure section below.
Participants and sampling
Elderly patients with a first time unilateral hip fracture over the age of 60 years were consecutively sampled from the orthopaedic wards of two public health care hospitals in Johannesburg, South Africa. The exclusion criteria consisted of patients with polytrauma and those with co-morbidities affecting mobility (stroke, Parkinson's disease or a spinal cord injury). Patients re-admitted with complications of a previous surgery or those managed conservatively were also excluded.
In total, ninety (n=90) subjects were consecutively entered into the study. This figure was determined using a power calculation on STATA version 12. The power was set at 90% and alpha at 5%. A loss to follow-up ratio was taken into consideration and was set at 20%. Standard deviations and the minimal clinical important difference for each outcome measure were used.5-7 Ethical clearance was granted by the Human Research Ethics Committee of the University of the Witwatersrand (M110403); institutional approval was also obtained and participants gave informed consent.
Pilot study
A pilot study was conducted to determine the intra-rater reliability of the first author, to enable her to familiarise herself with the tools that were used in the main study, and to establish the time taken to implement these tools. Twenty-seven patients were used in the pilot study; the patients were divided into three groups, and each group consisted of nine patients (10% of the number of participants in the main study). Each group was assessed pre-operatively, at discharge and six weeks post discharge. Data of patients participating in the pilot study were not included in the main study.
Outcome measures
The Six-Item Cognitive Impairment Test (6CIT) comprises six questions that take three to four minutes to complete. The scoring system uses weighting techniques and is thus slightly more complicated than previous tests. The total score is 28; scores of 0 to 7 are considered normal while scores of above 8 are significant in confirming a cognitive impairment. At the 7 to 8 cut-off the 6CIT gives a specificity of 100% and a sensitivity of 78.57%.5
One of the most commonly used tools for screening for cognitive impairment, as well as being regarded as the 'gold standard' is Mini Mental State Examination (MMSE).8 The 6CIT was validated against the MMSE and its suitability as a screening tool for dementia was established.5 The 6CIT was confirmed to be a short and simple test of cognition.5 The 6CIT correlates well with the MMSE (r2 = -0.911 p < 0.01) but fares better when screening for milder dementia; the MMSE when used as a screening test for dementia is of little value. Hence the 6CIT was the outcome measure decided upon in the study.
The Elderly Mobility Scale (EMS) is a physical assessment of function and has a score out of 20. The EMS provides a physiotherapy-oriented measure for frail elderly people.9 The scale assesses seven dimensions of functional performance. These include: locomotion, balance and key position changes, all of which are skills required for the performance of activities of daily living. The maximum score is 20, with higher scores indicating better performance. Latent class analysis of the EMS showed strong inter-rater (R2=0.0037 ρ=1.00) and intrarater reliability (R2=0.0035 ρ=0.72). A high correlation between the EMS and Modified Rivermead Mobility Index was established (Spearman's ρ=0.89), thus demonstrating concurrent validity.6
The Lower Extremity Functional Scale (LEFS) is used to evaluate the functional activity level of a patient with a disorder of one or both lower extremities.7 The LEFS is a questionnaire containing 20 questions about a person's ability to perform everyday tasks. The questionnaire starts off by asking the patient: 'Today would you have any difficulty with followed by a list of functional activities. These activities are scored from zero (extreme difficulty) to four (no difficulty). The maximum score is 80. The lower the score, the greater the disability. The LEFS has shown to be both reliable and valid.7 Construct validity was determined by comparing the LEFS to the physical function subscale [r=0.80 (95% CI=0.73)] and the physical component score [r=0.64 (95% CI=0.54)] of the 36-item short form health survey (SF-36). Intra-rater reliability was r=0.86 (95% CI=0.80).7 The LEFS was modified for cultural appropriateness in this study, as not all elderly South Africans may relate to the activity description 'walking a mile'.
Procedure
Pre-operative assessment
Following a successful pilot study, participants (n=90) were evaluated pre-operatively for the main study. Cognitive function was assessed using the 6CIT. Table I summarises the outcome measures used and at which point they were performed.
Discharge and six weeks post discharge assessment
Post-operatively cognitive function was assessed using the 6CIT, and functional outcomes were assessed using the EMS and LEFS at discharge (n=82) and six weeks post discharge (n=72) respectively. At six weeks post discharge, one participant had dropped out, six participants had been lost to follow-up and 11 had demised since the beginning of the study. The six participants lost to follow-up could not be reached physically or telephonically.
The EMS was carried out in the physiotherapy gym. Lying to sitting and sitting to lying were the first two activities that participants performed. These two tests were performed on a standard plinth. Thereafter, the participants were assessed on their ability to rise to standing from a 47 cm (19 in) chair in less than three seconds allowing the use of upper limbs. The ability to maintain an upright standing position with or without the use of upper limbs to steady yourself was also assessed. Participants were then instructed to mobilise; the scoring for gait was based on the type of assistance required to walk, not the distance walked.9 The participant was then timed walking over a distance of 6 metres, at their normal speed, using their usual walking aid. A maximum score was given for a time of under 15 seconds.9 Finally the participant was required to reach forward beyond an arm's length while maintaining a fixed base of support. A maximum score was attained for a functional reach of 20 cm.9
Data analysis
Data were analysed using IBM SPSS Version 19. Descriptive statistics were used to deduce the participants' demographic data. The McNemar statistical test analysing inferential data was presented using frequency tables, means and standard deviation or medians and interquartile ranges depending on the distribution of the data. Wilcoxon signed-rank tests were used to test whether there was a median difference in paired data. Spearman's rank correlation coefficient (r) was used to test if a linear relationship existed between cognitive function and post-operative functional outcome. A multivariate regression analysis was used to determine associations between variables. The study was set at p<0.05 level of significance and 95% confidence interval (CI).
Results
Of the 90 participants studied, n=50 (69.4%) participants were female and n=22 (30.6%) were male. The mean age of the participants was 75.7 years (SD ± 9.54). The minimum age was 60 years and the maximum was 95 years.
Final analysis was carried out on the participants (n=72) who completed the study. A comparison between the baseline median 6CIT scores of deceased participants (median 6CIT score of 24) and participants who completed the final assessment (median 6CIT score of 11.5) revealed that those participants who demised during the study, originally presented with poor cognitive impairment at baseline. A Mann-Whitney U score of 203 was calculated with a corresponding p-value of 0.01.
Participants aged 80 years and over and female participants presented with poorer cognitive scores compared to their younger and male counterparts. The Kruskal-Wallis H test is a non-parametric test that determines significant changes between two or more groups with ordinal data. A comparison between participants aged 80 and over and those participants between 60 and 79 years revealed a Kruskal Wallis H-statistic value of 14.8 and a corresponding p-value of 0.00. The result for male versus female was 1.3 (p=0.26).
Table II presents the frequency of 6CIT scores and the percentages of each total score (n=72).
The results indicate that participants found it much easier to answer questions relating to the year and month, with approximately 80% of participants answering correctly.
Questions that involved memory and reverse listing were more difficult. More than half of the participants made one or more errors when asked to say the months of the year in reverse and 36.1% of participants could not remember any component of the address phase they were asked to memorise and repeat later on at the pre-operative assessment. This result improved at discharge and six weeks post discharge.
Table III indicates that many participants presented with moderate cognitive impairments pre-operatively (mean 6CIT score of 10.5), but these impairments resolved and improved leading up to the final assessment at six weeks post discharge (mean 6CIT score of 6). There were also significant advances in cognition from baseline to six weeks post discharge (z-statistic -5.04, p=0.000).

Cognitive function is indirectly related to post-operative functional outcome. The correlation between cognitive function and early post-operative functional outcome is shown in Table IV.

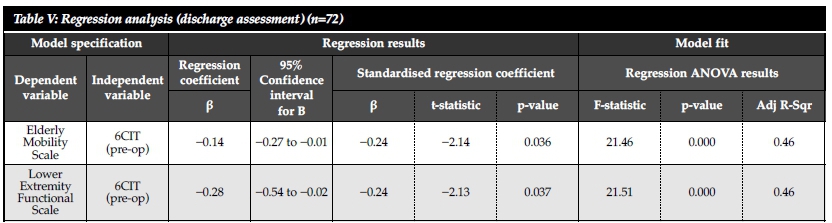
A multivariate regression analysis using the data collected at discharge revealed that the 6CIT (β= -0.14, p=0.036) assessed pre-operatively is a strong predictor of early post-operative functional outcome using only the EMS at discharge (Table V).
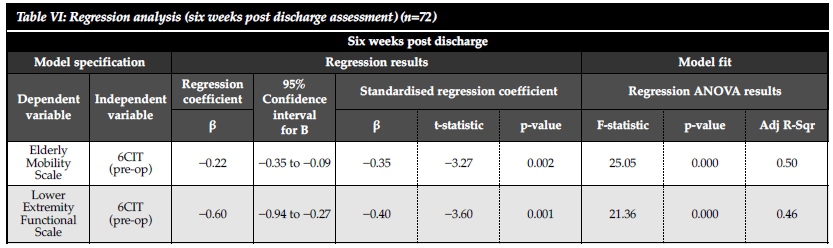
A multivariate regression analysis further revealed that the 6CIT assessed pre-operatively is a strong predictor of early post-operative functional outcome using the EMS (β= -0.22, p=0.002) and LEFS (β= -0.60, p=0.001), at six weeks post discharge. Table VI depicts the results of the multivariate regression analysis using the EMS and LEFS at six weeks post discharge.
In summary, cognitive impairment is a relatively strong predictor of early post-operative functional outcome. There is an interesting trend in the relationships between cognitive impairment at the three levels of functional outcome. The relationship gets stronger as you move through the different levels (i.e. from pre-operatively to six weeks post discharge). The relationship between pre-operative cognition and functional outcome at six weeks post discharge is stronger, thus indicating that pre-operative cognition is a stronger predictor of functional outcome at six weeks post discharge compared to functional outcome at discharge.
Discussion
A cognitive impairment in the context of this study includes the presence of any acute confusion states or the development of incident cognitive impairment during hospital admission. A cognitive impairment was diagnosed according to the score obtained on the 6CIT.
The current study revealed that the presence of a cognitive impairment pre-operatively has a negative influence on the post-operative functional level at discharge and six weeks post discharge. These findings of this study are consistent with another study that examined the adverse effects of cognitive impairment (Mini-Mental State Examination [MMSE]) in elderly hip fracture patients receiving inpatient rehabilitation.4 Fifty-seven elderly participants were recruited from a rehabilitation hospital in Pittsburgh, USA. It was concluded that poor cognitive function predicted poorer functional outcomes and these patients presenting with poor cognitive function were unable to participate as well in their therapy sessions.4 Participants' level of participation in therapy was evaluated using a newly developed Rehabilitation Participation Scale.4 This scale was found to have a ceiling effect and was modified later. Results similar to those of the current study were reported by two other studies.10,11 However, the final number of participants included in one of the studies was relatively small (n=59)11 and the mean age of participants included in the other study was 84 years, nine years older than the mean age of participants included in the current study.10
Improvement of cognitive function occurred during the course of this study. At six weeks post discharge only 19.4% of participants presented with a severe cognitive impairment compared to 30.6% pre-operatively. These results are consistent with those of a study that demonstrated that the incidence of acute confusion (measured by the NEECHAM Confusion Scale) after sustaining a hip fracture in the elderly population was 32% on admission and the day after surgery, and 14% the day before discharge.12 Despite the use of varying outcome measures used to determine the incidence of a cognitive impairment, fairly similar results were obtained. An interesting strength was the use of a self-reported measure to identify cognitive impairments.12
Conclusion
The results of this prospective pre-test-post-test observational study indicate that improvements in cognitive function do occur in the short term in elderly patients who sustain a hip fracture. The presence of cognitive impairments in elderly patients with a hip fracture does negatively influence the early post-operative functional outcome.
Implications for practice
Education and preventative measures to protect elderly patients from the trauma associated with a fall and subsequently a hip fracture is vital. For those patients who do sustain a hip fracture, intensive rehabilitation is especially necessary for the patient that presents with poor cognitive function. More importantly, determining that cognitive impairments do improve significantly in the short term assists medical practitioners in developing systematic approaches and interventions in the rehabilitation of these frail, elderly individuals.
Those patients who adopt a sedentary lifestyle or remain bedridden following surgical fixation of a hip fracture impact on the financial burden of health care. Therefore, those patients presenting with poorer cognitive function should be especially encouraged to participate in intensive rehabilitation.
Conflict of interest statement
Ethical approval: Human Research Ethics Committee of the University of the Witwatersrand (M110403).
Funding: No funding was received for this research.
Conflict of interest: None
No benefits of any form have been received from a commercial party related directly or indirectly to the subject of this article.
References
1. Holt G, Smith R, Duncan K, Hutchison JD, Gregori A. Outcome after surgery for the treatment of hip fracture in the extremely elderly. J Bone Joint Surg Am 2008;90:1899-1905. [ Links ]
2. Kalula S. Prevalence and problem of falls in older persons. Institute of Ageing in Africa 2012; University of Cape Town (unpublished). [ Links ]
3. Hershkovitz A, Kalandariov Z, Hermush V, Weiss R, Brill S. Factors affecting short-term rehabilitation outcomes of disabled elderly patients with proximal hip fracture. Arch Phys Med Rehabil 2007;88:916-21. [ Links ]
4. Lenze EJ, Munin MC, Dew MA, Rogers JC, Seligman K, Mulsant BH, Reynolds III CF. Adverse effects of depression and cognitive impairment on rehabilitation participation and recovery from hip fracture. Int J Geriatr Psychiatry 2004;19:472-78. [ Links ]
5. Brooke P, Bullock R. Validation of a 6 item cognitive impairment test with a view to primary care usage. Int J Geriatr Psychiatry 1999;14:936-40. [ Links ]
6. Nolan JS, Remilton LE, Green Me. The reliability and validity of the Elderly Mobility Scale in the acute hospital setting. Internet j. allied health sci. pract. 2008; http://ijahsp.nova.edu Volume 6 No. 4 ISSN 1540-58X Accessed 01/03/2011. [ Links ]
7. Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. Phys Ther 1999;79(4):371-82. [ Links ]
8. Folstein MF, Folstein SE, McHugh PR. 'Mini-Mental State' A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-98. [ Links ]
9. Smith R. Validation and reliability of the Elderly Mobility Scale. Physiotherapy 1994;80(11):744-47. [ Links ]
10. Soderqvist A, Miedel R, Ponzer S, Tidermark J. The influence of cognitive function on outcome after a hip fracture. J Bone Joint Surg 2006;88-A:2115-23. [ Links ]
11. Horgan NF, Cunningham CJ. Impact of cognitive impairment on hip fracture outcome in older people. Int J Ther Rehabil 2003;10(5):228-32. [ Links ]
12. Johansson I, Baath C, Wilde-Larsson B, Hall-Lord ML. Acute confusion states, pain, health, functional status and quality of care among patients with fracture during hospital stay. Int J of Orthop Trauma Nurs 2012; doi:10.1016/j.ijotn.2012.07.002 Published online 10 September 2012. Accessed 10/11/2012. [ Links ]
 Correspondence:
Correspondence:
Miss Saadiya Adam
Physiotherapy Department, Faculty of Health Sciences
School of Therapeutic Sciences, University of the Witwatersrand
7 York Road, 2193 Parktown, Johannesburg, South Africa
Tel: +2782 947 4268
Email: adam.saadiya@gmail.com


{kind=link}
{kind=link}
{kind=link}