










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.15 n.1 Centurion Mar./Apr. 2016
http://dx.doi.org/10.17159/2309-8309/2016/v15n1a7
TRAUMA
Evaluation of the first experience of intramedullary nail lengthening using PRECICE® in a South African limb lengthening and reconstruction unit
FF BirkholtzI, II; P de LangeIII
IMBChB, FC Orth(SA), MMed(Orth)(Pret); Department of Orthopaedic Surgery, University of Pretoria
IIMBChB, FC Orth(SA), MMed(Orth)(Pret); Walk-A-Mile Centre for Advanced Orthopaedics, Unit 2, Lifestyle Management Park, 223 Clifton Ave, Lyttelton, Centurion, South Africa, 0157
IIIMBChB, FC Orth(SA); Walk-A-Mile Centre for Advanced Orthopaedics, Unit 2, Lifestyle Management Park, 223 Clifton Ave, Lyttelton, Centurion, South Africa, 0157
ABSTRACT
BACKGROUND: Limb lengthening is performed through distraction osteogenesis after osteotomy and has traditionally been performed using external fixation. The PRECICE® Limb Lengthening System has recently emerged as an alternative method to control distraction. In this study, the first experience of intramedullary nail lengthening using PRECICE®, in a South African limb lengthening and reconstruction unit, was evaluated in terms of the accuracy of distraction and the number of implant-related complications that were reported
METHODS: A total of nine patients underwent the limb lengthening procedure in 11 limb segments. Distraction of the nail was initiated by ERC (external remote controller) around 10 days after surgery at a distraction rate of 1 mm/ day. The distraction was monitored every 2 weeks by clinical and radiographic examinations. Ongoing physiotherapy rehabilitation was performed until consolidation was achieved
RESULTS: A mean target distraction length of 45.18 mm (15 to 65 mm range) was obtained over an average follow-up period of 266 days, with an accuracy of 103% ± 18%. All the distraction segments united. Two complications were reported that were successfully treated
CONCLUSION: Limb lengthening using the PRECICE® nail system was found to have excellent accuracy of distraction, which is reproducible between different segments and indications. Acceptable complication rates were observed in this study
Key words: limb lengthening, PRECICE® nail, intramedullary lengthening, nail lengthening, leg lengthening
Introduction
Limb length discrepancies are often managed by limb lengthening of the long bones. The process of limb lengthening requires stabilisation of bones, followed by osteotomy and subsequently distraction of the limb segment. Various stabilisation methods exist including external fixation, internal lengthening devices and a combined approach.1 External fixation techniques like the Ilizarov Method have been the gold standard for limb lengthening.2 Although external fixation devices have numerous benefits and are widely used, it is associated
with various complications like pin tract infection, joint contractures and neurovascular impalement.3-6 Combined fixation techniques like lengthening over a nail (LON) or lengthening and then nailing (LATN), entails the removal of the external fixation device after the distraction phase. An intramedullary nail then supports the bone during the consolidation phase.7-9 This allows for a reduction of the external fixation time and a more comfortable consolidation phase, but this approach has also been associated with some complications.9,10 In an attempt to eliminate the associated adverse effects of both the external and combined fixation approaches, internal lengthening nails were introduced. These internal lengthening nails (ILNs) include devices such as the Albizzia®, Fitbone® and Intramedullary Skeletal Kinetic Distractor (ISKD).11-14 The ILNs are implanted into the intramedullary canal of long bones, and nail distraction then causes bone lengthening through distraction osteogenesis.1,11 High complication rates were previously reported with the ILNs and they tend to lack a dependable mechanism to monitor and control distraction.15-17 A new ILN system, the PRECICE® Limb Lengthening System (Ellipse Technologies, California, USA), has recently been FDA-approved for clinical use. The PRECICE® System is a magnetically operated intramedullary nail where the distraction of the tibia or femur can be controlled with precision and accuracy.18 This system uses an external remote control (ERC) technology to non-invasively adjust the required distraction rates.18 The PRECICE® System is predicted to be more accurate and reliable than previously used ILNs and to minimise the associated complications.11,19 The PRECICE® System was therefore evaluated in this study for accuracy of distraction and implant-related complications.
Materials and methods
Study patients
The study was a retrospective chart analysis of all consecutive PRECICE® nail patients. A total of nine patients (11 limb segments) underwent a limb lengthening procedure with this device between May 2013 and October 2014. The patients comprised seven males and two females with a mean age of 34 years (25-49 range). Of the lengthened limb segments, ten femoral and one tibial lengthening procedures were documented. Limb length discrepancies can be due to a number of origins, but in this study the aetiology was reported as post-traumatic for seven limb segments. The remaining four segments were lengthened for stature. All the involved patients were informed about the need for surgical removal after the desired target length was achieved and the regenerate had fully united. The appropriate institutional research ethics guidelines were adhered to.
Treatment, surgery and aftercare
The pre-operative assessment comprised clinical assessment as well as calibrated radiographs measured with a commercially available pre-operative planning software package. A newer version of the PRECICE® nail was introduced during the course of the study and patients received nails at a ratio of 5:6 (PRECICE 1:PRECICE 2). Nail diameter selection was based on the medullary canal diameter with eight and three patients receiving the 10.7 mm and 12.5 mm nails, respectively. The patient was placed on a fracture table under general anaesthesia. The anatomic axis of the bone was marked using fluoroscopic guidance, the nail length was marked on the limb and the osteotomy level was marked on average 12 cm proximal to the tip of the nail. Pre-drilling of the osteotomy site was performed through a 1 cm incision, thus venting the medullary canal. After placement of a guide wire, sequential reaming of the canal was performed to a diameter at least 1 mm larger than the nail diameter. The nail was brought down to the level of the osteotomy and, after completion of the osteotomy, advanced fully before the nail was locked proximally and distally. Nail functionality was tested intra-operatively using the ERC to distract the nail by 1 mm. Distraction of the nail started as an outpatient procedure at around 10 days after surgery (lag period ranging from 5-19 days) and proceeded at the conventional distraction rate of 1 mm/day in a single adjustment. Ongoing physiotherapy rehabilitation was performed and distraction was monitored by clinical and radiographic examinations every 2 weeks. Physiotherapy focused on maintenance of joint mobility and the prevention of contractures. Toe-touch weight bearing was allowed until consolidation was advanced.
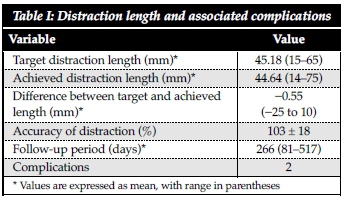
Distraction length, follow-up period and implant-related complications were documented (Table I). The distraction length measured radiographically at final follow-up visit was tabulated against the target distraction length (Table I). The complications were listed as observed during clinical and radiographic examinations. The statistical analysis was performed as outlined in Kirane et al. (2014), where the overall accuracy of distraction was calculated.11 The accuracy reflects the relative value of the target length (prescribed distraction) to the achieved distraction length represented as a percentage.
Results
The patients had a mean target distraction length of 45.18 mm (15 to 65 mm range). The distraction length that was achieved at final follow-up was 44.64 mm (14 to 75 mm range), leading to a mean difference between the target length and the actual distraction length of -0.55 mm (-25 to 10 mm range). The accuracy of distraction was calculated at 103% ± 18%. The average follow-up period was 266 days (81 to 517 days range).
All the regenerates showed satisfactory healing at final assessment. This was based on radiographic analysis showing the presence of neocorticalisation of the regenerate on two views. Two complications were reported.
The first complication occurred due to a protrusion of the tip of the nail through the femoral cortex and the nail was subsequently replaced with a trauma nail to stabilise the regenerate until union. This occurred because the tip of the PRECICE® nail ended in a previously lengthened part of the bone. The previous lengthening was performed with an external fixator and was done to reconstruct a large segmental bone defect in the femur. Due to the nail tip ending within a softer regenerate area, cortical resistance was lost and the distraction force pushed the nail through the cortex. The second complication was the failure of nail distraction in a femoral lengthening, in which case the nail was exchanged and distraction proceeded uneventfully. In this case it is suspected that under-reaming and a too tight interference fit of the nail prevented distraction and that additional reaming might have prevented this complication. All complications were successfully treated, and there were no other major complications.
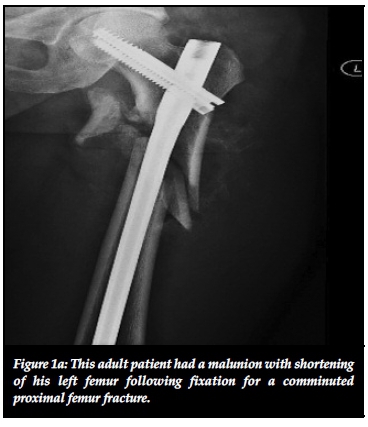
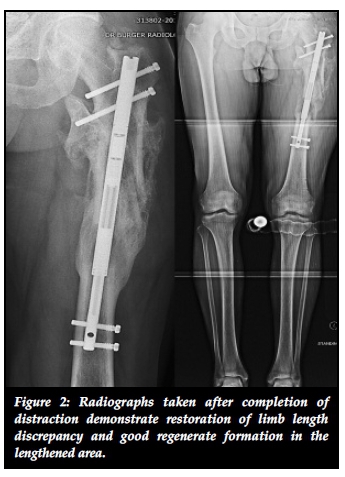
The nails were sized so that their tips ended up around 12 cm away from the osteotomy. For the femoral cases the osteotomy was in the proximal part, resulting in a nail that would end just distal to the midshaft region, as can be seen in Figure 1. The telescopic section of the nail is straight and this means that the nail cannot follow the natural sagittal curvature of the femur. This is another reason why the lengthening nail will not fill the whole length of the femur as is the case in trauma nails. Generally the regenerate formation was very satisfactory and consolidation occurred reliably and predictably (Figure 2).

Discussion
Various internal fixation devices have been developed to overcome the current limitations of external fixation in limb lengthening. Most of these devices (Albizzia®, Fitbone® and ISKD, etc.) have also been associated with implant-related complications. Albizzia® uses a patient's limb movements to acquire the mechanical forces needed for distraction but has been associated with premature consolidation, disproportionate fracture healing and nail rupture.20-22 Fitbone® is a motorised nail system driven by an external electronic controller but has been shown to lead to poor bone regeneration, pain during distraction and ROM restrictions.23-25 It also does not have the capability to back up the nail which is available with the PRECICE® Limb Lengthening System and useful in cases of poor regenerate formation or over distraction, although this was never required during this study. ISKD relies on lengthening by small rotational oscillations and have previously been associated with various complications including nail distraction failure, decreased ROM during distraction, pain and discomfort during nail distraction, infection, delayed union or insufficient regenerate requiring bone grafting.26-28 All three of the previously used internal lengthening devices seem to lack a dependable mechanism to monitor and control distraction.15-17 The recently FDA-approved PRECICE® Limb Lengthening System is a magnetically operated intramedullary nail where distraction can be controlled with precision and accuracy via an external remote controller.18 The PRECICE®
System is predicted to be more accurate and reliable than previously used ILNs and to minimise the associated complications.11,19 The PRECICE® System was therefore evaluated in this study based on the accuracy of distraction and implant-related complications.11-14
This small study comprised only nine patients with 11 limbs that required lengthening. This serves as a limitation of this study, as a larger patient pool would have been more significant. Subjects were chosen at random and led to a smaller range of gender and limb segment variance. When comparing the accuracy of the distraction to previous studies, an accuracy of 103% was obtained in this study compared to a previous study showing an accuracy of 96%.11 We showed that in the majority of the cases the required distraction length was achieved and even exceeded in some patients using the PRECICE® nail. The exceeded distraction length was primarily due to the cosmetic limb lengthening patients exceeding their initial lengthening targets.
When comparing the complications to previous studies investigating the efficacy of the PRECICE® nail system, the results were found to be similar, with limited implant-related complications.11,19 In previous cases the nail distraction failure also occurred (non-functional magnet mechanism), in which case the nail was replaced and distraction was successfully continued.11,19 In none of the previous studies or in the current study did any of the patients experience intolerable pain during distraction, as no external or painful rotational manipulation of the limbs was required.19 In a previous study done by Kirane et al. (2014), momentary loss of limb ROM was observed in various patients after surgery, and the original ROM recovered within a few months after surgery.11 This was not the case in the current study, as none of the patients experienced temporary loss of ROM in the limbs. This can possibly be attributed to the aggressive post-operative physiotherapy regimen. Non-implant related complications have been observed in previous studies that included premature osteotomy consolidation, delayed bone healing and toe clawing.11 This study did not show various non-implant related complications, but is limited by the small sample size. The occurrence of implant-related and non-implant related complications limits the efficacy of fixation devices used in limb lengthening surgery. The PRECICE® nail system may represent an accurate and controllable alternative to the existing intramedullary lengthening nails.
Acknowledgements
The authors wish to acknowledge Miss Nanika Coetzee for her assistance in manuscript preparation.
Conflict of interest statement
The content of the article is the sole work of the authors. No benefits of any form have been or are to be received from a commercial party related directly or indirectly to the subject of the article. The research was conducted in accordance with the institutional Ethics guidelines.
References
1. Taljanovic MS, Jones M, Ruth JT, Benjamin JB, Sheppard JE, Hunter TB. Fracture fixation. Radiographics 2003;23(6):1569-90. [ Links ]
2. Fragomen AT, Rozbruch SR. The mechanics of external fixation. HSS J 2007;3(1):13-29. [ Links ]
3. Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res 1990;250:81-104. [ Links ]
4. Noonan KJ, Leyes M, Forriol F, Canadell J. Distraction osteogenesis of the lower extremity with use of monolateral external fixation. A study of two hundred and sixty-one femora and tibiae. J Bone Joint Surg Am 1998;80(6):793-806. [ Links ]
5. Hantes ME, Malizos KN, Xenakis TA, Beris AE, Mavrodontidis AN, Soucacos PN. Complications in limb-lengthening procedures: a review of 49 cases. Am J Orthop 2001;30(6):479-83. [ Links ]
6. Faber FW, Keessen W, van Roermund PM. Complications of leg lengthening. 46 procedures in 28 patients. Acta Orthop Scand 1991;62(4):327-32. [ Links ]
7. El-Husseini TF, Ghaly NA, Mahran MA, Al Kersh MA, Emara KM. Comparison between lengthening over nail and conventional Ilizarov lengthening: a prospective randomized clinical study. Strategies Trauma Limb Reconstr 2013;8(2):97-101. [ Links ]
8. Paley D, Herzenberg JE, Paremain G, Bhave A. Femoral lengthening over an intramedullary nail. A matched-case comparison with Ilizarov femoral lengthening. J Bone Joint Surg Am 1997;79(10):1464-80. [ Links ]
9. Mahboubian S, Seah M, Fragomen AT, Rozbruch SR. Femoral lengthening with lengthening over a nail has fewer complications than intramedullary skeletal kinetic distraction. Clin Orthop Relat Res 2012;470(4):1221-31. [ Links ]
10. Rozbruch SR, Kleinman D, Fragomen AT, Ilizarov S. Limb lengthening and then insertion of an intramedullary nail: a case-matched comparison. Clin Orthop Relat Res 2008;466(12):2923-32. [ Links ]
11. Kirane YM, Fragomen AT, Rozbruch SR. Precision of the PRECICE Internal Bone Lengthening Nail. Clin Orthop Relat Res 2014. [ Links ]
12. Hankemeier S, Gosling T, Pape HC, Wiebking U, Krettek C. Limb lengthening with the Intramedullary Skeletal Kinetic Distractor (ISKD). Oper Orthop Traumatol 2005;17(1):79-101. [ Links ]
13. Guichet JM, Deromedis B, Donnan LT, Peretti G, Lascombes P, Bado F. Gradual femoral lengthening with the Albizzia intramedullary nail. J Bone Joint Surg Am 2003;85-A(5):838-48. [ Links ]
14. Cole JD, Justin D, Kasparis T, DeVlught D, Knobloch C. The intramedullary skeletal kinetic distractor (ISKD): first clinical results of a new intramedullary nail for lengthening of the femur and tibia. Injury 2001;32:Suppl 4:SD129-39. [ Links ]
15. Wang K, Edwards E. Intramedullary skeletal kinetic distractor in the treatment of leg length discrepancy-a review of 16 cases and analysis of complications. J Orthop Trauma 2012;26(9):e138-44. [ Links ]
16. Simpson AH, Kenwright J. Fracture after distraction osteogenesis. J Bone Joint Surg Br 2000;82(5):659-65. [ Links ]
17. Papanna MC, Monga P, Al-Hadithy N, Wilkes RA. Promises and difficulties with the use of femoral intra-medullary lengthening nails to treat limb length discrepancies. Acta Orthop Belg 2011;77(6):788-94. [ Links ]
18. Ellipse Technologies Inc. PRECICE Nail System: Ellipse Technologies. Available at: http://www.ellipse-tech.com/?q=ip. Accessed November 2, 2014. [ Links ]
19. Schiedel FM, Vogt B, Tretow HL, et al. How precise is the PRECICE compared to the ISKD in intramedullary limb lengthening? Reliability and safety in 26 procedures. Acta Orthop 2014;85(3):293-98. [ Links ]
20. Mazeau P, Assi C, Louahem D, L'Kaissi M, Delpont M, Cottalorda J. Complications of Albizzia femoral length ening nail: an analysis of 36 cases. J Pediatr Orthop B 2012;21(5):394-99. [ Links ]
21. Guichet JM, Deromedis B, Donnan LT, Peretti G, Lascombes P, Bado F. Gradual femoral lengthening with the Albizzia intramedullary nail. J Bone Joint Surg Am 2003;85-A(5):838-48. [ Links ]
22. Papanna MC, Monga P, Al-Hadithy N, Wilkes RA. Promises and difficulties with the use of femoral intra-medullary lengthening nails to treat limb length discrepancies. Acta Orthop Belg 2011;77(6):788-94. [ Links ]
23. Singh S, Lahiri A, Iqbal M. The results of limb lengthening by callus distraction using an extending intramedullary nail (Fitbone) in non-traumatic disorders. J Bone Joint Surg Br 2006;88(7):938-42. [ Links ]
24. Al-Sayyad MJ. Lower limb lengthening and deformity correction using the Fitbone motorized nail system in the adolescent patient. J Pediatr Orthop B 2012;21(2):131-36. [ Links ]
25. Kucukkaya M, Karakoyun O, Sokucu S, Soydan R. Femoral lengthening and deformity correction using the Fitbone motorized lengthening nail. J Orthop Sci 2015;20(1):149-54. [ Links ]
26. Lee DH, Ryu KJ, Song HR, Han SH. Complications of the Intramedullary Skeletal Kinetic Distractor (ISKD) in distraction osteogenesis. Clin Orthop Relat Res 2014;472(12):3852-59. [ Links ]
27. Kenawey M, Krettek C, Liodakis E, Wiebking U, Hankemeier S. Leg lengthening using intramedullay skeletal kinetic distractor: results of 57 consecutive applications. Injury 2011;42(2):150-55. [ Links ]
28. Wang K, Edwards E. Intramedullary skeletal kinetic distractor in the treatment of leg length discrepancy - a review of 16 cases and analysis of complications. J Orthop Trauma 2012;26(9):e138-44. [ Links ]
 Correspondence:
Correspondence:
Dr Franz Birkholtz
PO Box 11328, 0046 Centurion
Tel: +27 12 644 2641
Fax: +27 12 644 2642
Email: franz.birkholtz@walkamile.co.za

