










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309
Print version ISSN 1681-150X
SA orthop. j. vol.14 n.3 Centurion Aug./Sep. 2015
http://dx.doi.org/10.17159/2309-8309/2015/V14N3A5
SHOULDER
Simple bilateral anterior shoulder dislocation: A case report and review of the literature
N AliI; A BhatI; FA BangrooI; MS DhandaII; SC SharmaIII
IMS, Senior Resident, Department of Orthopaedics, SHKM Government Medical College Mewat, Haryana, India
IIMS, Assistant Professor. Department of Orthopaedics, SHKM Government Medical College Mewat, Haryana, India
IIIMS, DNB Professor and Director. Department of Orthopaedics, SHKM Government Medical College Mewat, Haryana, India
ABSTRACT
Bilateral shoulder dislocations are usually of the posterior type, which is commonly associated with seizures, electrocution or electroconvulsive therapy. Bilateral anterior shoulder dislocations are very rare and usually result from significant trauma. Simple bilateral anterior shoulder dislocations without associated fracture are much rarer and not many cases have been reported in the literature. We present a traumatic bilateral simple anterior shoulder dislocation in a 24-year-old male without any features of ligamentous laxity, and review the international literature on simple bilateral anterior shoulder dislocations. From the review we conclude that seizures are as important an aetiology of simple bilateral anterior shoulder dislocation as is trauma. Moreover, this injury is not as rare as was considered in the past.
Key words: shoulder, dislocation, bilateral, seizures, glenoid, anterior dislocation
Introduction
Shoulder dislocation is the most common type of joint dislocation encountered in humans.1,2 Anterior shoulder dislocation represents 95% of unilateral shoulder dislocations while unilateral posterior dislocation is far less common (4%).2,3 Bilateral shoulder dislocations do occur and unlike unilateral dislocations they are most commonly of the posterior type.2,4 Bilateral posterior dislocations are usually associated with seizures, electrocution and electroconvulsive therapy while bilateral anterior dislocations result from significant trauma.2,5,6 Asymmetrical bilateral dislocations with one shoulder dislocated anterior and the other one posterior are extremely rare and have been reported in the literature.7,8
Simple bilateral anterior shoulder dislocations without associated fracture are extremely rare. Very few cases have been reported in the literature.4,9 We present a case of traumatic simple bilateral anterior shoulder dislocation and review the international literature on this rare type of injury.
Case history
A young patient, 24 years of age, presented to our emergency department with complaints of pain and inability to move both his shoulders after he had suffered a backward fall from the edge of his bed. There was no history of alcohol intake, any medication or loss of consciousness.
There was no history suggestive of diabetes mellitus or seizure activity in the past. On examination the patient was conscious, cooperative and oriented. Vitals were normal. The respiratory and cardiovascular system examination was unremarkable. Both upper extremities were in the attitude of external rotation and abduction. Shoulders were bilaterally symmetrical but appeared squared. Laterally the sulcus sign was present together with the inability to palpate the greater tuberosity below the acromion on both sides. Movements were painful and restricted on both sides. Distally there was no motor, sensory or vascular deficit. There were no signs of generalised ligamentous laxity. Antero-posterior radiographs of both shoulder joints had empty glenoid cavity with the humeral head lying below the coracoid process, without any associated fractures (Figure 1). A diagnosis of traumatic simple bilateral anterior shoulder dislocation was made.

After baseline investigations for general anaesthesia, dislocation was reduced by Kocher's manoeuvre, first on one side followed by the other, under sedation. Reduction was secured in adduction and internal rotation by bilateral slings. Post-reduction radiographs had concentric reduction of both shoulder joints (Figure 2).

The patient was discharged from the hospital with both shoulders immobilised in slings.
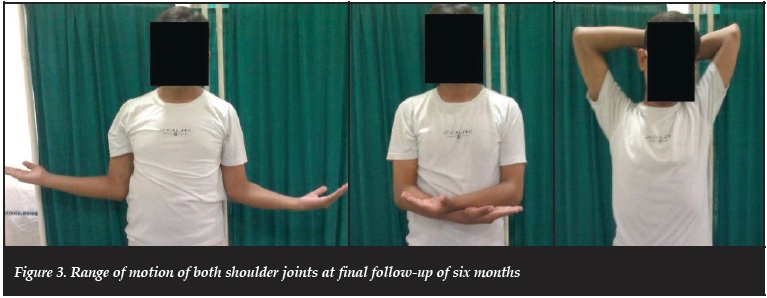
Intermittent pendulum movements of the upper extremities were started at two weeks and slings were discarded at four weeks after which full range of movement of shoulder joints was started. At eight weeks the patient gained full range of movement. At final follow-up of six months the patient had painless, full range of movement at the shoulder joints without any sign of shoulder instability (Figure 3).
Discussion
Trauma is the most common mode of bilateral anterior shoulder dislocation.5,6,10 The mechanism is the same as that of unilateral dislocation but the traumatic force should be uniformly distributed between the two shoulder joints to dislocate both.2,5,11 When a person falls backwards as happened in our case, there is a reflex tendency to take the weight of the body on the hands by extending the elbow joints and abducting, externally rotating and extending the shoulder joints. The shoulder joint in the position of abduction, external rotation and extension will have greater tuberosity impinged on the posterior aspect of the acromion.
Once vertical force is transmitted along the humerus it tends to hyper-extend the shoulder joint, which is prevented by this impingement and rather acts as a lever to deliver the head anterior out of the glenoid.12
Bilateral anterior shoulder dislocation is a rare injury and such an injury without an associated fracture is far rarer. Dinopoulos et al.(1999) in their review of literature had 28 cases of bilateral anterior shoulder dislocation reported since 1966 out of which only 11 were simple dislocations without any associated fracture.13 Siwach et al. (2008), in a similar type of literature review, reported only 14 cases of simple bilateral anterior dislocations.14 Dodds et al. (2008) in their review of 1966 reported 24 cases of bilateral anterior shoulder dislocations of which 18 were simple dislocations.15 After an extensive search of international literature we found 41 published papers since 1973 with 46 cases of simple bilateral anterior shoulder dislocation, which is the first of its kind and largest review ever of this rare injury in the orthopaedic literature (Table I).Sreesobh et al. (2005),9 Rouhani et al. (2010),4 Bilsel et al. (2012)16 and Yashavantha et al. (2013)10 in their reviews have mentioned, respectively, only two, four, eight and three cases of bilateral simple anterior shoulder dislocation being reported so far. Our literature review refutes this injury being so rare.

In our review of the case presented, fall on hands or elbows was the most common mode of injury (16 cases) followed by seizure activity, including hypoglycaemic seizures (12 cases). In seizures, anterior dislocation occurs by extension, abduction and external rotation of shoulder joint by direct or indirect trauma.14 Weight-lifting in gymnasiums and during military drill is emerging as aetiology (four cases).
Our literature review refutes this injury being so rare
Sudden exhaustion of shoulder muscles during work out can make the heavy weight push the shoulder joints in the position of instability and finally dislocation.11,17-19 Both sudden forward traction to upper extremities in position of flexion, internal rotation and slight abduction (four cases) as well as sudden backward traction in position of extension, internal rotation and adduction (one case) can dislocate the shoulder joints anterior.14,20-22 Fall with hands catching an overhead bar tends to dislocate the shoulder posteriorly but in the elderly population with age-related ligamentous laxity anterior shoulder dislocation is a possibility (two cases).6 Diving (one case), backstroke swimming (one case), domestic assault (one case), push-ups (one case) and chin-ups (one case) were the other rare mode of injuries.23-27 In three cases of bilateral simple anterior shoulder dislocation aetiology was unknown.28-30
Shoulder dislocation is said to be chronic when it remains unreduced beyond three weeks.31 Four cases had chronic bilateral shoulder dislocation at the time of diagnosis among which two cases had seizures as the aetiology and in other two cases the cause was unknown.28,29,32,33
Sequential bilateral anterior dislocations with one shoulder dislocating after the other have been reported in the literature and are extremely rare. There have been two cases of sequential simple bilateral anterior dislocation reported to date.9,34
Bilateral anterior shoulder dislocation is managed on the same lines as unilateral dislocation.8 Closed reduction followed by immobilisation for three weeks in bilateral sling is the standard protocol.12,35 But bilateral immobilisation of the upper extremities makes the patient dependent and his routine suffers. For this reason some authors recommend the use of upper extremities for personal hygiene and feeding purpose only during the period of immobilisation.8 Others recommend early rehabilitation of the shoulder which is less painful, while continuing immobilisation of the more painful one.36 Even early rehabilitation of both shoulders has been recommended especially in elderly patients.35 Surgical intervention is rarely required in simple bilateral anterior dislocations as most of them are reduced closed. Failure of closed reduction, and old missed or neglected dislocation, are indications for open reduction. All the requirements for internal fixation of proximal humerus as well as for shoulder prosthetic replacement should be available and on hand before attempting closed reduction under general anaesthesia as it carries a risk for fracture of the proximal humerus during manipulation, especially in elderly with osteo-porosis.16 Patients with old neglected dislocations can be managed by open reduction but the results are poor. In elderly patients with neglected dislocations who are at high risk during surgical intervention, a benign neglect strategy can be followed.35
Conclusion
Final functional outcome of bilateral simple shoulder dislocations is the same as that of unilateral dislocations.
Trauma is the most common aetiology of simple bilateral anterior shoulder dislocation. Seizure is nearly as common an aetiology as is trauma. Dislocations that are chronic at diagnosis are usually associated with seizures. Moreover, bilateral simple anterior shoulder dislocation is not as rare an injury as was previously thought.
We declare that no benefits of any form have been received from a commercial party related directly or indirectly to the subject of this article.
References
1. Aronson PL, Mistry RD. Intra-articular lidocaine for reduction of shoulder dislocation. Pediatr Emerg Care 2014;30(5):358-62. [ Links ]
2. Galanakos S, Christodoulou E, Panayi C, Papadakis AS, Nicolaides V, Macheras GA. EEXOT 2008;59(4):252-56. [ Links ]
3. Ngim NE, Udorroh EG, Udosen AM. Acute bilateral anterior shoulder dislocation following domestic assault - case report. West Afr J Med 2006;25(3):256-57. [ Links ]
4. Rouhani A, Zonooz KA, Aghdam HA. An unusual cause of bilateral anterior shoulder dislocation. Pak J Med Sci 2010;26(4):976-77. [ Links ]
5. Thakur A, Gupta R, Kotwal V, Arora D. A rare case of bilateral anterior dislocation of the shoulder. J clin diagn res 2010;4:3567-69. [ Links ]
6. Kalkan T, Demirkale I, Ocguder A, Unlu S, Bozkurut M. Bilateral anterior shoulder dislocation in two cases due to housework accidents. Acta Orthop Traumatol Turc 2009:43(3):260-63. [ Links ]
7. Sandeep K, Nema DR, Pai NKS, Krishna KG. A unique case of non- traumatic asymmetric shoulder dislocation with four-part fractures of proximal humeri following seizures. J Emerg Trauma Shock 2013;6(3):231-23. [ Links ]
8. Botha AH, Du Toit AB. Bilateral anterior shoulder dislocation: A case report of this rare entity. SA orthop J 2010;9(4):68-70. [ Links ]
9. Sreesobh KV, Chacko B. An unusual case of bilateral anterior dislocation of the shoulder. J Orthop 2005;2(4):e6. [ Links ]
10. Yashavantha KC, Nalini KB, Maini L, Nagaraj P. Bilateral traumatic anterior dislocation of the shoulder - a rare entity. J Orthop Case Reports 2013;3(1):23-25. [ Links ]
11. Creswell TR, Smith RB. Bilateral anterior shoulder dislocations in bench pressing: an unusual cause. Br J Sports Med 1998;32:71-72. [ Links ]
12. Silva LP, Sousa CV, Rodrigues E, Alpoim B, Leal M. Bilateral anterior glenohumeral dislocation: clinical case. Res Bras Orthop 2011;46(3):318-20. [ Links ]
13. Dinopoulos HT, Giannoudis PV, Smith RM, Matthews SJ. Bilateral anterior shoulder fracture - dislocation. A case report and review of the literature. Int Orthop 1999;23(2):128-30. [ Links ]
14. Siwach R, Singh R, Rohilla R, Sangwan SS. Bilateral anterior dislocation of the shoulder - A case report and review of the literature. Injury Extra 2008;39:394-97. [ Links ]
15. Dodds SD, Medvecky MJ. Chronic bilateral locked anterior shoulder fracture-dislocations. Am J Orthop 2008;37(7):364-68. [ Links ]
16. Bilsel K, Sayar S, Ceylan HH, Erdil M, Elmadag M, Tuncay I. Bilateral Traumatic Anterior Shoulder Dislocation. J Clin Analytical Med 2012;2012:385782. [ Links ]
17. Sciammarella JC Jr. Bilateral shoulder dislocations. Ann Emerg Med 1986;15(6):763. [ Links ]
18. Maffulli N, Mikhail HMT. Bilateral anterior glenohumeral dislocation in a weightlifter. Injury 1990;21(4):254-56. [ Links ]
19. Esenkaya I, Tuygun H, Turkmen M. Bilateral Anterior Shoulder Dislocation in a Weight Lifter. An improperly performed military press put this patient at risk. Phys Sports Med 2000;28(3):782. [ Links ]
20. McFie J. Bilateral anterior dislocation of the shoulder. Injury 1976;8:67-9. [ Links ]
21. Segal D, Yablon IG, Lynch JJ, Jones RP. Acute bilateral anterior dislocation of the shoulders. Clin Orthop Relat Res 1979;140:21-22. [ Links ]
22. Turhan E, Demirel M. Bilateral anterior glenohumeral dislocation in a horse rider: a case report and a review of the literature. Arch Orthop Trauma Surg 2008;128(1):79-82. [ Links ]
23. Mathis RD. Bilateral shoulder dislocation: an unusual occurrence. J Emerg Med 1990;8(1):41-43. [ Links ]
24. Ngim NE, Udorroh EG, Udosen AM. Acute bilateral anterior shoulder dislocation following domestic assault - case report. West Afr J Med 2006;25(3):256-57. [ Links ]
25. De la Fuente FA, Hoyte C, Bryant SM. Push-ups may be hazardous to your health: an atraumatic etiology for bilateral shoulder dislocation. Am J Emerg Med 2008;26(1):116.e3-4. [ Links ]
26. Felderman H, Shih R, Maroun V. Chin-Up-Induced Bilateral Anterior Shoulder Dislocation: A Case Report. J Emerg Med 2009;37(4):400-402. [ Links ]
27. Dlimi F, Rhanim, Lahlou A, Kharmaz M, Ouadghiri M, El Bardouni A, Berrada MS, Mahfoud M, El Yaacoubi M. Bilateral anterior dislocation of the shoulders at the start of a backstroke competition. J Orthop Traumatol 2012;13:47-49. [ Links ]
28. Onabowale BO, Jaja MO. Unreduced bilateral synchronous shoulder dislocations. A case report. Niger Med J 1979; 9(2):267-71. [ Links ]
29. Costigan PS, Binns MS, Wallace WA. Undiagnosed bilateral anterior dislocation of the shoulder. Injury 1990;21(6):409. [ Links ]
30. Bellazzini MA, Deming DA. Bilateral anterior shoulder dislocation in a young and healthy man without obvious cause. Am J Emerg Med 2007;25(6):734.e1-3. [ Links ]
31. Jekic M. Der seltene Fall beiderseitiger Oberarmverrenkung. Langenbecks Arch Chir 1973;334:331. [ Links ]
32. Sadhra K. Unusual dislocations associated with epileptic fits. Br Med J 1984;288(6418):681-82. [ Links ]
33. Brown RJ. Bilateral dislocation of the shoulders. Injury 1984;15:267-73. [ Links ]
34. Singh S, Kumar S. Bilateral anterior shoulder dislocation: a case report. Eur J Emerg Med 2005;12(1):33-35. [ Links ]
35. Ballesteros R, Benavente P, Bonsfills N, Chacon M, Garcia-Lâzaro FJ. Bilateral anterior dislocation of the shoulder: review of seventy cases and proposal of new etiological-mechanical classification. J Emerg Med 2013;44(1):269-79. [ Links ]
36. Dunlop CCR. Bilateral anterior shoulder dislocation - a case report and review of the literature. Acta Orthop Belg 2002;68(2):168-70. [ Links ]
37. Hartney-Velazco K, Velazco A, Fleming LL. Bilateral anterior dislocation of the shoulder. South Med J 1984;77:1340-41. [ Links ]
38. Jones M. Bilateral shoulder dislocation. Br J Sports Med 1987:21:139. [ Links ]
39. Litchfield JC, Subhedar VY, Beevers DG, Patel HT. Bilateral dislocation of the shoulders due to nocturnal hypoglycaemia. Postgrad Med J 1988;64(752):450-52. [ Links ]
40. Mehta MP, Kottamasu SR. Anterior dislocation of the shoulders with bilateral brachial plexus injury. Ann Emerg Med 1989;18(5):589-91. [ Links ]
41. Echarri Sucunza A, Santesteban Echauri E, Irigoyen J, Aldaz Berruezo J. Anterior bilateral scapulohumeral luxation after convulsive crisis. Aten Primaria 2002;30(2):134. [ Links ]
42. Ozcelik A, Dincer M, Cetinkanat H. Recurrent bilateral dislocation of the shoulders due to nocturnal hypoglycemia: a case report. Diabetes Res Clin Pract 2006;71(3):353-55. [ Links ]
43. O'Connor-Read L, Bloch B, Brownlow H. A missed orthopaedic injury following a seizure: a case report. J Med Case Rep 2007;1:20. [ Links ]
44. Abalo A, Dossim A, Songne B, Ayouba G. Bilateral anterior dislocation of the shoulders. Chir Main 2008;27(2):118-21. [ Links ]
45. Akdur O, Ozkan S, Durukan P, Ikizceli A, Avsarogullari L, Vardar A, Sozuer EM. Erciyes Med J 2008;30(2):125-27. [ Links ]
46. Mofidi M, Kianmehr N, Farsi D, Yazdanpanah R, Majidinezhad S, Asadi P. An unusual case of bilateral anterior shoulder and mandible dislocations. Am J EmergMed 2010;28(6):745.e1-2. [ Links ]
47. Tripathy SK, Sen RK, Aggarwal S, Dhatt SS, Tahasildar N. Simultaneous bilateral anterior shoulder dislocation: report of the two cases and review of the literature. Chin J Traumatol 2011;14(5):312-15. [ Links ]
 Correspondence:
Correspondence:
Dr Nadeem Ali
Cell: +919812962979; Phone: + 9101942423211
Email: drnadeeem@gmail.com


{kind=link}