










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.14 no.1 Centurion Fev./Mar. 2015
GENERAL
Early excision of heterotopic ossification for pain control: A case report
C YogeswaranI; PK OrokoII
IBMedSc, MBBS, MRCS Surgical Resident; Assistant Professor, Consultant Orthopaedic Surgeon Aga Khan University Hospital, Nairobi
IIMBChB, MMed(Surg), FRCS(Ed), FRCS (Tr. & Orth); Assistant Professor, Consultant Orthopaedic Surgeon Aga Khan University Hospital, Nairobi
ABSTRACT
BACKGROUND: Heterotopic ossification rarely presents with pain as the primary symptom
CASE: A 31-year-old soldier presented with severe right hip pain 2.5 months after a craniectomy following a penetrating brain injury. Examination revealed a right-sided hemiplegia and a stiff hip with the patient resisting any passive movements due to severe pain. A hip X-ray confirmed massive heterotopic ossification of the right hip. Pain was so severe that he required management by the pain control team who administered analgesics including the use of several epidural catheters and femoral nerve blocks. There was also significant restriction in activity, including physiotherapy, due to pain. Exploration and excision of the heterotopic bone at the right hip 2.5 months after diagnosis revealed significant compression and stretching of the sciatic nerve by the heterotopic bone. The massive heterotopic bone was excised followed by radiotherapy using 800 cGy within 24 hours of surgery. Post-operatively pain control was significantly improved with only simple analgesics being required
CONCLUSION: Heterotopic ossification at the hip can be associated with significant pain when compression of the sciatic nerve is involved. Early surgical excision is indicated, instead of waiting until maturity of heterotopic bone, for the main purpose of achieving pain control
Key words: heterotopic ossification, traumatic brain injury, hip, nerve entrapment
Introduction
Clinically significant heterotopic ossification following traumatic brain injury (TBI) has a reported incidence of 11%.1 Common presenting symptoms are limited joint movement, pain, erythema and swelling of the affected joint.2-4 More commonly, however, it is detected as an incidental finding on X-ray.5 Pain associated with fever, erythema and swelling may be prominent early in the course of the disease but does not often persist. Reduction in joint range of movement and ankylosis are prominent late features.5
Common presenting symptoms of heterotopic ossification are limited joint movement, pain, erythema and swelling of the affected joint
Surgical treatment for heterotopic ossification is usually delayed until maturity of the heterotopic bone is achieved. In patients with traumatic brain injury, a delay of up to 18 months has been recommended. Delay in surgery is thought be associated with fewer post-operative complications such as haemorrhage and recurrence.6 A case of a patient with heterotopic ossification of the right hip following traumatic brain injury presenting with significant hip pain due to entrapment of the sciatic nerve is discussed. Early surgery and excision of heterotopic ossification, in this instance, led to significant improvement in symptoms.
Case report
A 31-year-old soldier presented with severe right hip pain 2.5 months after craniectomy for penetrating brain injury. The initial neurological deficit from the brain injury was a right hemiparesis. The patient had made significant recovery from his brain injury. From an initial Glasgow Coma Scale (GCS) of 3/15, he was now able to communicate with persisting deficits being moderate cognitive impairment and a right hemiparesis. The patient was making significant gains in rehabilitation and was mobilising with assistance between parallel bars at the time of presentation. Pain occurred at rest and was worsened by any movements of the hip, leading to restriction of rehabilitation. On examination, right hip movements were restricted by pain. No flexion or extension was possible and there was about 5 degrees of hip rotation. Power was graded on the Medical Research Council (MRC) scale at 2/5 in the right lower limb. An X-ray of the right hip revealed Brooker Grade IV heterotopic ossification of the right hip.7 The patient was placed on simple analgesia but pain was still significant requiring management by the pain control team. The pain was difficult to control and the patient required multiple epidural catheters and femoral nerve blocks with large doses of opioids and bupivacaine. The patient's rehabilitation had regressed to only passive movements in bed.

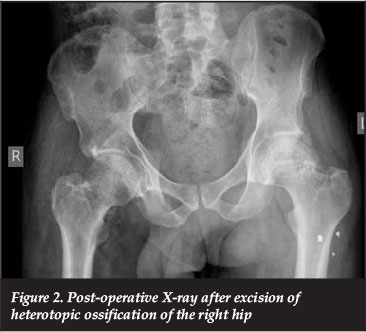
Due to poor pain control and significant restriction in activity, the patient underwent exploration and excision of heterotopic bone only 2.5 months after presentation. At surgery, examination under anaesthesia revealed a completely stiff right hip with no movement at all. Massive heterotopic bone was found extending from the right iliac wing to the proximal femur. This was exposed and removal of the bone begun distally. The sciatic nerve was exposed and found to be stretched posteriorly by the heterotopic bone. Almost all the heterotopic bone was excised while protecting the sciatic nerve throughout the procedure. Post-operatively, full extension, rotation and abduction were achieved with flexion of the right hip limited to 90-100 degrees. The patient received a single fraction of 800 cGy within 24 hours post-operatively as prophylaxis. On the subsequent days, the patient's analgesic requirement substantially reduced and his pain was controlled with simple analgesics consisting of paracetamol, diclofenac and tramadol. The patient was again able to participate in rehabilitation. No clinical features of recurrence have been noted to date, 3 months after surgery.
Discussion
Heterotopic ossification does not usually present with severe pain that persists. Heterotopic ossification in patients with neurological injury is typically asymptomatic and often detected as an incidental finding on radiographs.5 Early and intermediate symptoms include pain, swelling and stiffness which may be followed by decreasing pain, swelling and stiffness as the disease progresses. Early signs include erythema, swelling, warmth and loss of joint range of motion progressing to further decrease in range and movement and eventual possible ankylosis.2-4 Common complications of heterotopic ossification include progressive loss of joint motion and resulting loss of function. Rarely, compression of peripheral nerves by heterotopic bone can occur which results in severe pain.2-4
Direct pressure on the nerve from enlarging bone or inflammation that occurs during formation are thought to contribute to nerve compression.3 The majority of patients progress without these complications. However, about 10-20% of patients experience significant loss of movement, and up to 10% develop ankylosis.2
Management of heterotopic ossification is directed at maximising function and limiting progression. Non-steroidal anti-inflammatory medication, bisphosphonates and radiotherapy have been established as effective prophylaxis against heterotopic ossification. Surgery is generally performed when maturity of the heterotopic bone has been achieved.6,8 The aim of surgery is to improve mobility, reduce spasms and prevent complications of limited movement in patients with heterotopic ossification.3,6,9 Several studies have reported significant functional improvement following surgery in patients with heterotopic ossification following traumatic head injury.9-10
Recommended patient selection prior to surgical excision in patients following traumatic brain injury include radiologically mature heterotopic bone, good neurological and cognitive function and good selective control of the extremity.6,10 Good pre-operative neurological status has been associated with the lowest recurrence in patients with heterotopic ossification following traumatic head injury. Patients with Class I and II (minimal cognitive deficit with mild to moderate physical disability) Rancho Los Amigos Classification are associated with the lowest recurrence. In contrast patients with Class V (moderate to severe cognitive deficit with severe physical disability) had the highest recurrence.6
The aim of surgery is to improve mobility, reduce spasms and prevent complications of limited movement in patients with heterotopic ossification
Controversy regarding early versus late excision exists. Early studies have shown that delay in excision is associated with less recurrence and fewer complications.6 However, more recent studies on early excision at the elbow and hip have shown functional improvement without significant recurrence.11-12 Previous recommendations were to delay surgery for at least 1.5 years for patients with traumatic brain injury.6 The rationale for this was that majority of neurologic recovery has occurred by 1.5 years. Better neurologic recovery with voluntary muscle control and patient participation is associated with less recurrence.13 In addition, it is expected that at this stage there is less metabolically active bone, decreased rate of bone formation and therefore fewer post-operative complications of haemorrhage and recurrence are expected.14 More recently however, early excision has been found to improve function without increasing recurrence. A study looking at early excision of heterotopic ossification of the elbow in a series of eight patients observed no recurrence after an average of 46 months post excision and radiotherapy.
In addition, the authors found that early excision provided easier excision of immature bone from tissue planes resulting in fewer operative complications and better functional independence in rehabilitation.13 In addition, a recent study looking at late surgical excision of heterotopic ossification of the hip found increased incidence of femoral neck fractures in patients with established ankylosis compared to non-ankylosed hips. This was associated with an increased incidence of disuse osteopaenia associated with prolonged immobilisation.14


In the case of our patient, where pain due to sciatic nerve compression was a significant feature, early surgery with excision led to significant improvement in symptoms of pain and functional improvement. Although excision was performed 2.5 months after diagnosis, the patient did not experience the complication of significant haemorrhage requiring transfusion. Though there are no clinical features to suggest recurrence, this cannot be fully ruled out given that it has only been 3 months since excision. Importantly, however, recurrence has not been associated with maturity of the heterotopic bone and the only correlation with recurrence in traumatic brain injury has been the pre-operative neurological state, previous heterotopic ossification and multiple joint involvement.6 In our patient, delaying surgery could have led to opioid dependence with poor pain control and possible complications from multiple epidural catheter insertions. Regression in rehabilitation with immobilisation could have also led to associated complications of contractures, disuse osteoporosis and pressure ulcers.
Optimal timing to surgery therefore is a balance between risk of recurrence against potential benefits and complications. Early excision for improvement in symptoms and function may have a role in patients with heterotopic ossification following traumatic brain injury.
Conclusion
Heterotopic ossification can be associated with significant pain when entrapment of peripheral nerves occurs. In this instance, early surgery with excision led to significant improvement in pain control. This was associated with better early functional outcome and quicker rehabilitation. No good evidence exists to suggest that early excision is associated with greater complications or recurrence. Traditional recommendations to wait 1.5 years prior to excision for patients with traumatic brain injury may no longer be relevant and the decision to operate may be based on symptoms for quicker recovery of function.
References
1. Garland DE, Blum CE, Walters RL, California, D. Periarticular heterotopic ossification in head injured adults. J Bone Joint Surgery Am. 1980;62A(7):1143-46. [ Links ]
2. Garland DE. Clinical perspective on common forms of acquired heterotopic ossification. Clin Orthop Relat Res. 1991;263:13-29. [ Links ]
3. Cipriano CA, Pill SG, Keenan MA. Heterotopic ossification following traumatic brain injury and spinal cord injury. J Am Acad Orthop Surg. 2010;17(11):689-97. [ Links ]
4. Kaplan FS, Glaser DL, Hebela N, Shore EM. Heterotopic ossification. J Am Acad Orthop Surg. 2004;12(2):116-25. [ Links ]
5. Balboni TA, Gobezie R, Mamon HJ. Heterotopic ossification: pathophysiology, clinical features and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys. 2000;65(5):1289-99. [ Links ]
6. Garland DE, Hanscom DA, Keenan MA, Smith C, Moore T, California D. Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surgery Am. 1985;67A(8):1261-69. [ Links ]
7. Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement: Incidence and a method of classification. J Bone Joint Surgery Am. 1973;55:1629-32. [ Links ]
8. Garland DE. Clinical observations on fracture and heterotopic ossification in the spinal cord and traumatic brain injured populations. Clin Orthop Relat Res. 1988;233:86-101. [ Links ]
9. Kolessar DJ, Katz SD, Keenan MA. Functional outcome following surgical resection of heterotopic ossification in patients with brain injury. J Head Trauma Rehabil. 1996;11(4):78-87. [ Links ]
10. Moore TJ. Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma. 1993;7(1):11-14. [ Links ]
11. McAuliffe JA, Wolfson AH. Early excision of heterotopic ossification about the elbow followed by radiation therapy. J Bone Joint Surg Am. 1997;79A(5):749-55. [ Links ]
12. Genet F, Marmorat JL, Lautridou C, Schnitzler A, Mailhan L, Denormandie, P. Impact of late surgical intervention on heterotopic ossification of the hip after traumatic neurological injury. J Bone Joint Surg Am. 2009; 91-B(11):1493-98. [ Links ]
13. Garland DE. Surgical approaches for resection of heterotopic ossification for traumatic brain-injured adults. Clin Orthop Relat Res. 1991;263:59-70. [ Links ]
14. Shebab D, Elgazzar AH, Collier BD. Heterotopic ossification. J Nucl Med. 2002;43(3):346-53. [ Links ]
 Correspondence:
Correspondence:
Dr Carnjini Yogeswaran
Aga Khan University Hospital, Nairobi 3rd Parklands Avenue
PO Box 30270- 00100 GPO
Nairobi, Kenya
Tel: +254717022905
Email: carnjini@gmail.com

