










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSA Orthopaedic Journal
versión On-line ISSN 2309-8309
versión impresa ISSN 1681-150X
SA orthop. j. vol.13 no.4 Centurion dic. 2014
Glenoid hypoplasia: A case series of ten shoulders
P RyanI; P JordaanII; JP du PlessisIII; B VrettosIV; S RocheV
IMBChB(UCT), FC(Orth)(SA), MMed(Orth)UKZN; Department of Orthopaedic Surgery, University of KwaZulu-Natal
IIMBChB(US); Department of Orthopaedic Surgery, University of Cape Town
IIIMBChB(UCT), FC(Otho)(SA), MMed(Orth)UCT; Department of Orthopaedic Surgery, University of Cape Town
IVMBChB(Zim), FRCS(Eng), FCS(SA)Orth, MMed(Orth)UCT; Department of Orthopaedic Surgery, University of Cape Town
VMBChB(UCT), LMMC, FCS(SA)Orth; Department of Orthopaedic Surgery, University of Cape Town
INTRODUCTION
The terms 'glenoid hypoplasia', 'glenoid dysplasia' and 'dentate glenoid' refer to an uncommon developmental abnormality of the lower glenoid and scapular neck. The presenting symptoms are variable depending on the age at presentation, and in many cases the diagnosis is made incidentally on X-ray. The exact incidence is unknown, but is estimated in cadaveric and MRI studies to be in the region of 14.3% to 35% depending on the ethnic population studied.12 Current orthopaedic literature consists of case reports and small case series, with some of the more recent papers focusing on the arthroplasty management and implications.3-5
Key words: glenoid hypoplasia, glenoid dysplasia, dentate glenoid
Patients and methods
From January 2002 to May 2013, nine patients (ten shoulders) with radiological signs of glenoid hypoplasia were identified.
There were eight male and one female patients. The mean age at presentation was 37.2 years (range 23-77) and the mean symptom duration was 11.7 months (range 1-48). Six shoulders were managed conservatively. The four shoulders that underwent surgical management were for labral tears/pathology, one patient of whom suffered from multidirectional instability.
Results
Table I summarises the clinical data, including management, follow-up and subjective shoulder scores. Concerning the non-surgically managed patients, the diagnosis was impingement and tendonitis in three, calcific tendonitis in one, adhesive capsulitis in one and a labral tear in one.
One patient was not contactable. In the remaining five, the mean follow-up was 27 months (range 5 to 60) and the mean Oxford shoulder score was 47. All were subjectively very satisfied with their shoulder function.
Of the four surgically managed patients, one (patient 5, posterior labral tear) was not contactable. Of the remaining three, all had labral pathology. The patient with a SLAP lesion and anterior labral extension was doing well at 23 months post surgery with an OSS of 47. One patient with a posterior labral tear was doing well with an OSS of 45 at 3 months post surgery, while the other had a slightly lower OSS of 43 at 15 months post-op. This patient has multidirectional instability, and was found at the time of surgery to have a posterior labral tear, a reverse HillSacks and early cartilage eburnation.
Although rare, glenoid hyperplasia may be more common than previously recognised
The summary of the radiographic evaluation is seen in Table II.
According to the Wirth classification, one shoulder was graded as mild, five graded as moderate, and four graded as severe. Additional radiological features of lateral clavicular hooking were seen in three, acromial enlargement in four, humeral changes of hypoplasia and varus in four, and coracoid hypoplasia in two.
Discussion
Glenoid hypoplasia, first described by Valentine in 1931,6 is a rare developmental abnormality, which affects the osseous development of the inferior glenoid. It has also been termed 'glenoid dysplasia', 'posterior glenoid rim deficiency', and 'dentate glenoid'. The incidence is largely unknown as many cases are asymptomatic and discovered incidentally on radiographs. Symptomatic dysplasia accounts for around 0.5% of patients seen in some shoulder units.7
Two articles report on the incidence of glenoid hypoplasia in a general population. Edelson2 evaluated dry bone specimens and reported an incidence of between 19% and 35% for different ethnic groups. The highest incidence was seen in Alaskan Eskimo and northern Chinese populations. In an MRI study of 103 consecutive MR arthrograms, Harper et al.1 report an incidence of 14.3% for moderate to severe glenoid dysplasia. Most series of symptomatic dysplasia report a male predominance.7-9
Although the exact aetiology is unknown, familial occurrence has been noted in a few case reports10-13 and a spontaneous mutation, resulting in an autosomal dominant pattern with low penetrance, has been suggested.7,14 In a review of the genetics of scapular anomalies, Williams et am.15 conclude that the various parts of the scapula develop under different genetic control genes, and that the scapula has a different embryonic origin and genetic control than the rest of the upper limb.
Similar bony abnormalities are seen in Apert syndrome,16 and in cases secondary to other primary pathologies, such as obstetric brachial plexus trauma, muscular dystrophy, avitaminosis A and C, childhood bone and joint infection, haemophilic arthropathy and trauma.7
The scapula forms from at least eight ossification centres. The glenoid fossa forms from an inferior and a superior (or subcoracoid) centre (Figure 1). The coracoid has primary, secondary and tertiary centres, and the acromion has a further two centres. In utero, part of the body of the scapula is ossified. At birth, the majority of the lateral aspect of the scapula including the glenoid, coracoid, lateral scapular border and acromion are cartilaginous, and ossification of these scapular processes, including the glenoid, is complete by mid-adolescence.

The superior or subcoracoid centre fuses at around age 15 years, and the inferior, horse shoe-shaped epiphysis fuses after this. It is suggested that glenoid hypoplasia results from abnormal ossification of either or both the upper and lower glenoid centres.
Clinical presentation
The clinical presentation of patients with symptomatic dysplasia is variable. Smith et am.7 evaluated 12 patients, and divided them into two groups based on their age at presentation and symptoms. The first group was patients who presented prior to adulthood with symptoms of instability and clicking, while the second group (after the age of 40 years) presented with symptomatic early onset osteoarthritis. Wirth et am.,8 in their evaluation of 16 patients, divided them into three groups. Group 1 included patients with bilateral dysplasia without instability. Group 2 were patients with bilateral dysplasia and instability. Group 3 had unilateral hypoplasia with associated humeral head deformity. They too recognise the association of dysplasia with early onset glenohumeral arthrosis.
Both Pettersson et am}7 and Wirth et am.8 demonstrated an inverse relationship between the degree of dysplasia and the resultant shoulder range of motion.
In our series, five patients presented with labral pathology at an average age of 27.4 years (23-30 years) and four patients presented with tendonitis/impingement at an average age of 50 years (35-77 years). There were no cases of early onset glenohumeral arthrosis.
The association of posterior labral tears with glenoid dysplasia has been evaluated by Harper et am.1 who report a 64.3% incidence of labral tears seen on MRI scans in patients with moderate to severe dysplasia. Impingement and tendinopathy are thought to occur due to the relatively large and inferiorly sloping acromion, and the mechanical disadvantage of a more medialised centre of rotation and relatively shortened rotator cuff musculature.
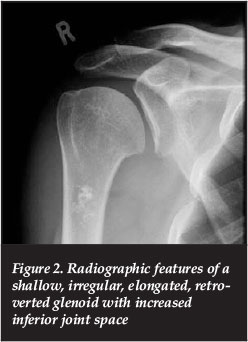
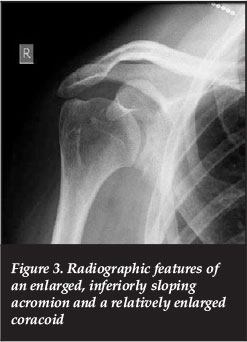
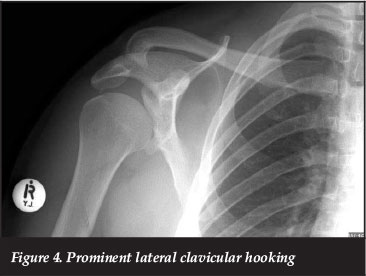
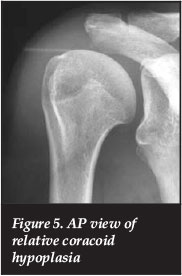
Radiographic features
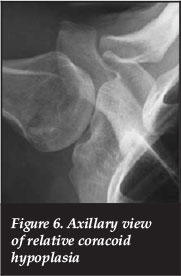
The radiographic features of glenoid hypoplasia have been well documented7-918 and include a shallow, irregular, elongated, retroverted glenoid with increased inferior joint space; an enlarged and infero-lateral tilted acromion; a prominent coracoid; and a hooked clavicle (Figures 2 to 4). Although the classical feature is that of relative coracoid prominence, we found two shoulders (Figures 5 and 6) with hypoplasia of the process. This is thought to have resulted from a more diffuse dysplastic process which has affected the coracoid ossification centres.
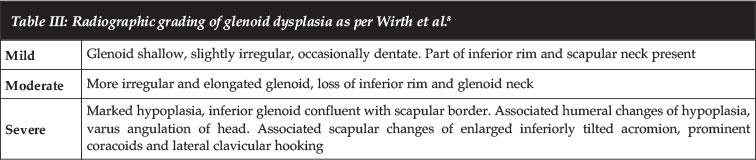
The above features are present to varying degrees depending on the severity of the dysplasia, and have been graded by Wirth et al. (Table III) into mild, moderate and severe.8
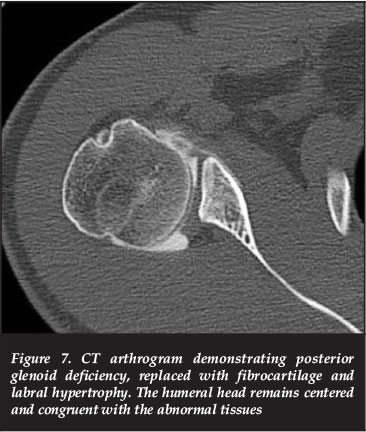
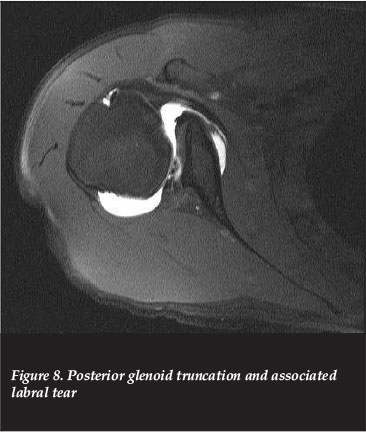
MRI features include rounding or truncation of the posterior glenoid rim, and hypertrophied low and medium signal intensity posterior labral tissues. Despite significant bony abnormality, both MRI and CT arthrography may show a smooth articular surface which is congruent with the humeral head (Figure 7). On MRI, the hypoplastic area is seen to be replaced with tissue which has similar signal characteristics to fibrocartilage or fat (Figure 8), supporting the theory that failure of ossification is the causes of the pathology. Associated secondary labral changes such as tears, degeneration, detachment and ganglion cysts may also been seen (Figure 8).9
Harper et am.1 grade the severity of the dysplasia on the axial MRI cuts into mild, moderate or severe depending on the degree of postero-inferior glenoid truncation and posterior sloping.
In our series, plain radiographs were obtained for all patients, MRI in one and CT arthrography in one. One glenoid was graded as mild, five as moderate and four as severe. Associated bony changes were seen as follows: hooking of the clavicle in three, coracoid hypoplasia in two shoulders which demonstrated more severe upper glenoid hypoplasia, acromial enlargement in four, and humeral varus and hypoplasia in four.
In the two cases of relative coracoid hypoplasia, the upper glenoid and coracoid changes are thought to represent a more diffuse affectation of the relevant ossification centres.
Management
The management of glenoid hypoplasia has been described in a few papers. In their series of 12 patients, Smith et am.7 report symptom resolution with physiotherapy and rehabilitation in their younger patients with presenting complaints of minor instability or pain. One patient with multidirectional instability underwent surgery in the way of posterior glenoid augmentation and capsular shift, with an unfavourable outcome. In their group of patients over the age of 40, all five had early onset osteoarthritis which responded poorly to non-operative management. Three patients underwent hemiarthroplasty, which they report as technically difficult and with relatively disappointing outcomes.
In a review of 16 patients, Wirth et am.8 managed all patients with a tailored rehabilitation programme, and report that at a mean of five years follow-up, the majority had returned to their previous activity level with symptom resolution. However, they allude to hemiarthroplasty possibly playing a role in certain patients with unremitting symptoms.
There are conflicting reports regarding the place and results of hemi and total arthroplasty in the management of secondary osteoarthritis with underlying glenoid hypoplasia. Bonnevialle et am.5 report satisfactory results, at a mean of 71 months follow-up (28-126), in ten shoulders treated with hemarthroplasty. One patient underwent revision surgery for instability secondary to subscapularis insufficiency. Contradicting this, Sperling et am.1 in their study of seven patients (four hemiarthroplasties and three total shoulder arthroplasties), revised three of their hemiarthroplasties to total shoulder replacements for continued symptoms. The one hemiarthroplasty that was not revised had the glenoid addressed at the time of hemiarthroplasty, with a posterior re-directional osteotomy. Of the three shoulders that had glenoid components inserted, two demonstrated loosening; however, none needed revision. They conclude that the glenoid deficiency and cartilage wear should be addressed at the time of surgery.
Reconstructive arthroplasty surgery is technically demanding, may have inferior results to that performed on the normal shoulder, and one should consider addressing the glenoid deficiency at the time of surgery
The indications for reverse total shoulder arthroplasty continue to expand to include pathologies other than rotator cuff tear arthropathy. A number of recent articles highlight the use of the reverse prosthesis in cases of severe glenoid bone loss.19-22 Hyun et am.22 describe a case of glenoid dysplasia secondary to Kniest syndrome which was managed with a reverse total shoulder arthroplasty. They report satisfactory radiographic appearance at six-month follow-up.
In our study, none of the patients presented with symptomatic early degeneration of the gleno-humeral joint. All patients were managed initially with nonoperative measures based on the presenting pathology, with good clinical outcomes in six, as evident by the subjective shoulder scores. Of the patients that required surgical intervention, all were for labral pathology. Two patients did well with Oxford Shoulder scores of 47 and 45, while one did less well with an OSS of 43. This patient was noted at the time of surgery to have degenerative cartilaginous changes secondary to instability.
Conclusion
We present a case series of patients with glenoid hypoplasia and associated shoulder pathologies. We confirm the male predominance, association with labral pathology and the poor clinical outcome when associated with multidirectional instability. In addition, we present a number of other patients who presented with pathologies other than labral tears, instability or early onset arthrosis. These were managed successfully with routine nonoperative means.
Although glenoid hypoplasia is rarely seen in clinical practice, it appears the abnormality may be more common than previously recognised. Shoulder symptoms should be treated on their merits and on an individual case basis. Should reconstructive arthroplasty surgery be embarked upon, the caveats should include: this is technically demanding, it may have inferior results to that performed on the normal shoulder, and one should consider addressing the glenoid deficiency at the time of surgery.
References
1. Harper KW, et am. Glenoid dysplasia: incidence and association with posterior labral tears as evaluated on MRI. AJR Am J Roentgenol, 2005;184(3):984-88. [ Links ]
2. Edelson JG. Localized glenoid hypoplasia. An anatomic variation of possible clinical significance. Cmin Orthop Remat Res, 1995(321):189-95. [ Links ]
3. Edwards TB, et al. Shoulder arthroplasty in patients with osteoarthritis and dysplastic glenoid morphology. J Shoulder Elbow Surg, 2004;13(1):1-4. [ Links ]
4. Sperling JW, Cofield RH, Steinmann SP. Shoulder arthroplasty for osteoarthritis secondary to glenoid dysplasia. J Bone Joint Surg Am, 2002;84-A(4):541-46. [ Links ]
5. Bonnevialle N, et al. Hemiarthroplasty for osteoarthritis in shoulder with dysplastic morphology. J Shoulder Elbow Surg, 2011;20(3):378-84. [ Links ]
6. Valentine B. Die kongenitale schulter-luxation. Orthop Chir, 1931(55):229. [ Links ]
7. Smith SP, Bunker TD. Primary glenoid dysplasia. A review of 12 patients. J Bone Joint Surg Br, 2001;83(6):868-72. [ Links ]
8. Wirth MA, Lyons FR, Rockwood CA Jr. Hypoplasia of the glenoid. A review of sixteen patients. J Bone Joint Surg Am, 1993;75(8):1175-84. [ Links ]
9. Theodorou SJ, Theodorou DJ, Resnick D. Hypoplasia of the glenoid neck of the scapula: imaging findings and report of 16 patients. J Comput Assist Tomogr, 2006;30(3):535-42. [ Links ]
10. Kozlowski K Scougall J. Congenital bilateral glenoid hypoplasia: a report of four cases. Br J Radiol, 1987;60(715):705-706. [ Links ]
11. Samilson RL. Congenital and developmental anomalies of the shoulder girdle. Orthop Clin North Am, 1980;11(2):219-31. [ Links ]
12. Stanciu C, Morin B. Congenital glenoid dysplasia: case report in two consecutive generations. J Pediatr Orthop, 1994;14(3):389-91. [ Links ]
13. Weishaupt D, Zanetti M, Exner GU. Familial occurrence of glenoid dysplasia: report of two cases in two consecutive generations. Arch Orthop Trauma Surg, 2000;120(5-6):349-51. [ Links ]
14. Andrews SB, Smithson SF. Dominant inheritance of primary glenoid dysplasia. Shoulder and Elbow, 2007;7:13-15. [ Links ]
15. Williams MS. Developmental anomalies of the scapula-the 'omo'st forgotten bone. Am J Med Genet A, 2003;120A(4):583-87. [ Links ]
16. Murnaghan LM, et al. A clinicoradiologic study of the shoulder in Apert syndrome. J Pediatr Orthop, 2007;27(7):838-43. [ Links ]
17. Pettersson H. Bilateral dysplasia of the neck of scapula and associated anomalies. Acta Radiol Diagn (Stockh), 1981;22(1):81-84. [ Links ]
18. Suryawanshi A, et al. Unilateral glenoid hypoplasia: a case report and review of the literature. Case Rep Orthop, 2011;article ID 412721. [ Links ]
19. Sears BW, et al. Glenoid bone loss in primary total shoulder arthroplasty: evaluation and management. J Am Acad Orthop Surg, 2012;20(9):604-13. [ Links ]
20. Mizuno N, et al. Reverse total shoulder arthroplasty for primary glenohumeral osteoarthritis in patients with a biconcave glenoid. J Bone Joint Surg Am, 2013;95(14):1297-304. [ Links ]
21. Macaulay A, Levine W. Reverse total shoulder replacement in patients with severe glenoid bone loss. Operative Techninques in Orthopaedics, 2011;21(1):86-93. [ Links ]
22. Hyun YS, et al. Uncommon indications for reverse total shoulder arthroplasty. Clin Orthop Surg, 2013;5(4):243-55. [ Links ]
 Correspondence:
Correspondence:
Dr P Ryan
Email: paullisa.ryan@gmail.com
This article is also available online on the SAOA website (www.saoa.org.za) and the SciELO website (www.scielo.org.za). Follow the directions on the Contents page of this journal to access it.


{kind=link}
{kind=link}
{kind=link}