










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Orthopaedic Journal
versão On-line ISSN 2309-8309
versão impressa ISSN 1681-150X
SA orthop. j. vol.13 no.1 Centurion Jan./Mar. 2014
KNEE
The influence of posterior condylar offset on maximum knee flexion: a retrospective analytical study
W van GraanI; W van der MerweII
IMBChB(Pret). Orthopaedic Registrar, Department of Orthopaedics, Faculty of Health Sciences, University of the Free State, Bloemfontein
IIMBChB, MMed (Ortho)UFS. Orthopaedic Surgeon, Medi-Clinic, Bloemfontein
ABSTRACT
BACKGROUND: Achieving maximum knee flexion following total knee replacement (TKR) remains a major goal for every knee arthroplasty surgeon. Studies to understand the kinematics of the knee therefore remain of utmost importance. Speculation remains regarding what the correct posterior condylar ratio should be after surgery and whether a change in posterior condylar offset will have an impact on the amount of flexion achieved.
OBJECTIVES: The aim of this study was to determine the role of the posterior condylar offset on knee flexion and whether a change in posterior condylar offset influenced the amount of flexion achieved. Since multiple causes for a change in knee flexion have been identified before, we have tried to eliminate as many variables as possible to keep our focus on the influence on posterior condylar offset on knee flexion.
METHODS: Our study was unique in that all our surgery was performed using computer-assisted surgery (CAS), which ensured our measurements were very accurate and allowed us to eliminate more of the variables that could influence the results. Pre- and post-operative flexion were determined and compared to the pre- and postoperative posterior condylar offset ratio (PCOR) as measured by the Bristol knee group.
RESULTS: We found an almost uniform increase in the posterior condylar offset post surgery, although a poor correlation between the pre- and post-operative flexion achieved was observed.
CONCLUSION: An increase in PCOR after surgery does not lead to an increase in flexion achieved post-surgically. The pre-operative flexion a patient has is still the benchmark in predicting post-surgical outcome.
Key words: posterior condylar offset, PCOR, knee flexion, computer-assisted surgery, TKA.
Introduction
In a progressively challenging society, the necessity for optimal knee flexion following a total knee replacement (TKR) is becoming increasingly important. Understanding the kinematics regarding TKR function and how small changes influence knee function is therefore of utmost importance. A high demand to achieve deep flexion exists among our current population of patients, with even higher demands for this result existing in the Middle and Far East due to cultural reasons.
A great deal of speculation remains with regard to the ideal posterior condylar offset (PCO) after a TKR to obtain maximum flexion of the knee. During a knee replacement, a change in this offset is inevitable as a standardised prosthesis is fitted. Whether this change leads to improved or worse flexion is still being debated.
The concept of PCO was first introduced in an article in 2002.1 The idea that an increase in PCO can increase flexion is easily illustrated as seen in Figure 1, showing that a larger condylar offset should increase flexion achieved.
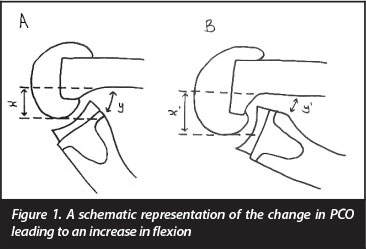
As shown in Figure 1, a higher PCO is achieved in knee B than in knee A, as shown by distance x. This in turn leads to an increase in the clear space behind the femoral condyle, which results in more superior flexion in knee B than in knee A, with a decrease in distance y. During flexion, the posterior edge of the tibia needs to move into this space to allow flexion. A small amount of clear space would lead to early abutment and prevent further flexion, while a larger amount of clear space would result in more flexion being allowed before the edge of the tibia would come into contact with the femur shaft. The concept of expressing this measurement as a ratio was introduced,2 enabling us to compare knees of different sizes, as this ratio has been proven to be very consistent in anatomic studies.
Another important aspect of knee replacement that can be evaluated is whether any gender-based discrepancies occur when comparing male and female patients. Trends in the prosthetic design industry to make gender specific implants are currently observed,3 and it is a topic under consideration. This study also investigated possible differences in anatomy with regard to gender.
A review and assessment of the literature focused on the different components that could cause a lack of flexion in a TKR. A number of major components was brought to light and considered in our study. PCO, femoral roll-back and femoral component external rotation were regarded as some of the possible factors that could influence knee flexion after a TKR.4 Condylar roll-back and paradoxical roll-forward as a cause for poor flexion were also proposed.5 Controversy was also found, with the importance of the PCO still being debated. Some studies showed that a higher PCO would increase flexion,2,6 while others pointed out that the degree of PCO made no difference.7-9 Pre-operative flexion as a predictor for post-operative outcome has been investigated extensively,10,11 and this points towards a close correlation between pre-operative and post-operative ranges of motion.
Our study focused on the role of the posterior condylar offset ratio (PCOR) and how this influenced the amount of knee flexion achieved after a TKR. We attempted to eliminate as many variables as possible, such as rehabilitation, pain experienced, accuracy of measurement, standardising the tibial slope and using only one specific implant, to keep our focus on the PCO, and whether a change in offset after a TKR will change the amount of flexion achieved.
Methods
A retrospective analytic review of a case series of navigated posterior stabilised TKRs was performed. The protocol for the study was approved by the Ethics Committee of the Faculty of Health Sciences, University of the Free State (ECUFS NR 45/2011). An independent statistical mathematician was contracted to assist the authors with the interpretation of data.
Our study is unique in the sense that we used computer-assisted surgery (CAS) software to do the knee replacements. With the patient anaesthetised, we measured the maximum amount of flexion before surgery commenced and immediately afterwards, which allowed us to exclude a substantial number of the variables that had occurred in previous studies. Pre-operative patient pain or discomfort was eliminated since patients were anaesthetised. Postoperative rehabilitation and other patient factors that could inhibit flexion after surgery were also eliminated because measurements were done immediately post-operatively. Data were stored on the computer intra-operatively. The computer also measured flexion with considerably more precision than could be obtained using hand-held devices. The angulation of the knee could be measured to within half a degree.
Posterior stabilised knees (PFC Sigma implants) were used and eliminated possible paradoxical roll-forward that could cause a block in flexion. Using a single brand also contributed to standardisation of the findings. The posterior tibial slope cut was standardised, as well as the femoral component external rotation fitment, once again creating a situation in which more of the possible variables were standardised to keep the focus on our study.
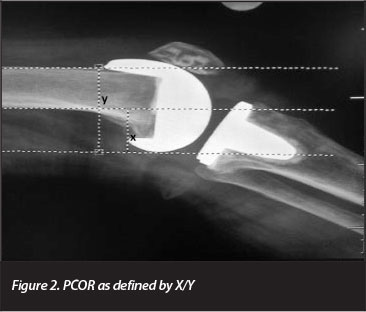
One hundred and twenty-six consecutive knee replacements were reviewed and considered for inclusion in our study. Pre- and post-operative perfect lateral X-ray views were necessary for inclusion to allow correct measurements. Adequate navigational data were also required to determine pre- and post-operative flexion. The way in which PCOR was measured is illustrated in Figure 2, and was first proposed as the best way to measure PCOR at the 14th European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) Congress in Oslo, 2010.12
Results
Eighty (63.5%) of the 126 patients qualified for inclusion in the study, of whom 51 (63.8%) were female.
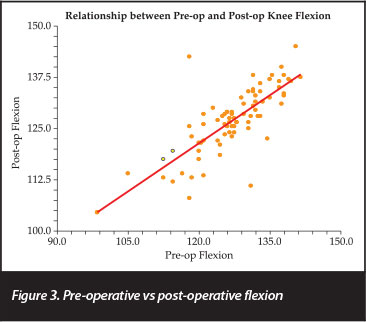
The relationship between pre- and post-operative flexion was determined, the results of which are shown in Figure 3. The mean pre-operative flexion was 126 degrees, with a range of 98.5 to 141.5 degrees. This correlated well with the mean post-operative flexion, also 126 degrees (range 104.0 to 145.0 degrees), suggesting a statistically significant correlation between pre- and post-operative flexion (p-value 0.001).
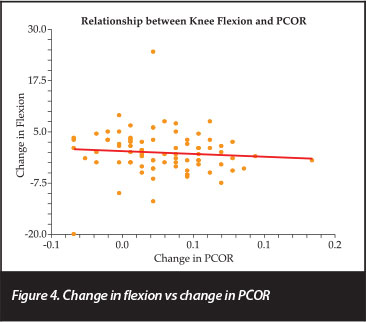
With regard to change in the PCOR, a general increase of this ratio from 0.44 to 0.49 after a knee replacement occurred. Although we could demonstrate an increase in PCOR, a similar increase in flexion achieved was not observed, as shown in Figure 4, and the p-value of 0.46 pointed towards a poor correlation between the increase in PCOR and flexion achieved.
Separate plotting of results for each gender was done in order to determine whether the correlation between change in PCOR and change in flexion differed between male and female patients. This comparison is shown in Figure 5, representing female and male patients, respectively.
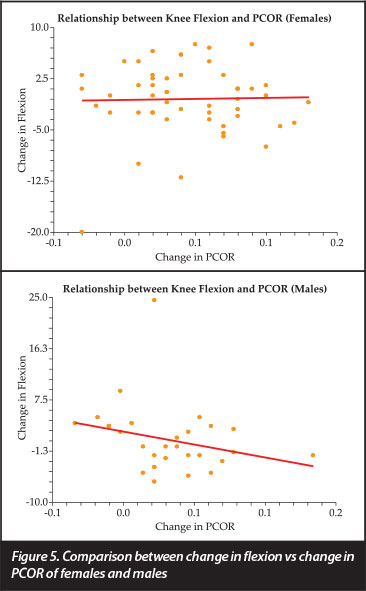
Results shown in Figure 5 reflect a poor correlation between post-operative flexion and change in PCOR among females. Male patients actually tended to have a downwards curve, implicating a decrease in flexion as change in PCOR increased. The small number of patients, however, led to a poor p-value of 0.16, and consequently, interpretation of the results was rendered unspecific.
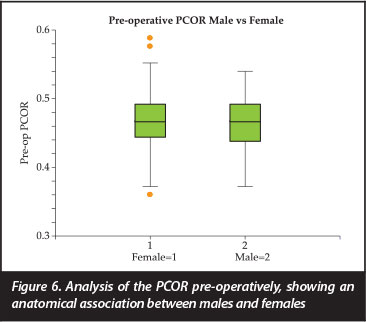
A comparison of pre-operative PCOR between genders is presented in Figure 6. The results point towards a close anatomic relationship of the pre-operative PCOR between male and female patients, with females tending to have a number of outliers both ways. Little difference concerning the PCOR could therefore be expected between males and females.
Discussion
With a large amount of data currently being produced in order to understand the kinematics of knee flexion and function, this study produced some noteworthy findings and is unique in its design. The use of CAS opens the door for more accurate measurements and easier data storage. The data can then be used to further our knowledge of orthopaedics and improve on future prosthetic design and placement.
The first notable observation that came forward was that despite an obvious change in the anatomy of the knee, the amount of pre- and post-operative flexion achieved was almost identical. This finding correlates with other studies which also report that pre-operative flexion could be considered as a major predictive factor for post-operative range.10
The current prosthetic design obviously favours an increase in PCOR. In our study, 91% of the patients had an increase in PCOR, which should theoretically lead to an increase in flexion achieved.13 We found no evidence from our data to support this theory in practice. We observed a poor correlation between change in PCOR and flexion achieved, leading us to believe that other factors could be at play that might also influence the amount of flexion achieved. We standardised the tibial slope, implant used and amount of external rotation, and ensured a perfect mechanical axis and balanced gap workflow with the CAS system. Some or all of these factors could still play a role to optimise flexion. The exact role that soft tissue plays in knee flexion is still unclear, but may probably be substantial in the eventual amount of flexion a knee can achieve. Our study focused on the amount of flexion achieved directly post-operatively, and did not consider whether future rehabilitation would be able to improve flexion.
We also noted that at an anatomic level, little difference could be observed in the PCOR between male and female TKR patients, reiterating the necessity for further research and careful anatomical comparisons between genders.
Only then will it be clear whether gender-specific implants have a role to play in the prosthesis design and manufacturing industry. From our current results, however, there seems to be no specific requirements for different gender implants with relation to PCO.
Acknowledgements
Dr Daleen Struwig, medical writer, Faculty of Health Sciences, University of the Free State, is acknowledged for technical and editorial preparation of the manuscript.
References
1. Bellemans J, Banks S, Victor J, Vandenneucker H, Moemance A. Fluoroscopic analysis of the kinematics of deep flexion in total knee arthroplasty: influence of posterior condylar offset. J Bone Joint Surg. Br. 2002;84:50-53 [ Links ]
2. Soda Y, Oishi J, Nakasa T, Nishikawa K, Ochi M. New parameter of flexion after posterior stabilized total knee arthroplasty: posterior condylat offset ration on X-ray photographs. Arch Orthop Trauma Surg 2007;127:167-70. [ Links ]
3. Greene KA. Gender-specific design in total knee arthroplasty. Arthroplasty 2007;22(3):27-31 [ Links ]
4. Victor J, Bellemans J. Physiologic kinematics as a concept for better flexion in TKA. Clin Orthop Relat Res 2006;452:53-58. [ Links ]
5. Massin P, Gournay A. Optimization of the posterior condylar offset, tibial slope, and condylar roll-back in total knee arthro-plasty. J Arthroplasty 2006;21:889-96. [ Links ]
6. Malviya A, Lingard EA, Weir DJ, Deehan DJ. Predicting range of motion after knee replacement: the importance of posterior condylar offset and tibial slope. Knee Surg Sports Traumatol Arthrosc 2009;17:491-98. [ Links ]
7. Kim YH, Sohn KS, Kim JS. Range of motion of standard and high-flexion posterior stabilized total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am 2005;87:1470-75. [ Links ]
8. Hanratty BM, Thompson NW, Wilson RK, Beverland DE. The influence of posterior condylar offset on knee flexion after total knee replacement using a cruciate-sacrificing mobilebearing implant. J Bone Joint Surg Br 2007;89:915-18. [ Links ]
9. Bauer T, Biau D, Colmar M, Poux X, Hardy P, Lortat-Jacob A. Influence of posterior condylar offset on knee flexion ater cruciate-sacrificing mobile-bearing total knee replacement: a prospective analysis of 410 consecutive cases. Knee 2010;17:375-80. [ Links ]
10. Ho ST, Chui KW. Range of motion after total knee replace ment for osteoarthritis. Hong Kong J Orthop Surg 2003;7:108-12. [ Links ]
11. De Carvalho LH Jr, De Castro CAC, Gongalves MBJ, Rodrigues LCM, Da Cunha FVP, Lopes FDL. Range of motion after total knee replacement. Acta Ortop Bras 2005;13:233-34. [ Links ]
12. Johal P, Hassaballa M, Eldridge J, Murray J, Robinson J, Porteous A. The posterior condylar offset ratio in total knee arthroplasty (Abstract number FP27-1311). Knee Surg Sports Traumatol Arthrosc 2010;18(Suppl 1):S60. [ Links ]
13. Bellemans J, Banks S, Victor J, Vandenneucker H, Moemans A. Fluoroscopic analysis of the kinematics of deep flexion in total knees arthroplasty. Influence of posterior condylar offset. J Bone Joint Surg Br 2002;84:50-53. [ Links ]
 Correspondence:
Correspondence:
Dr Wouter van Graan
Department of Orthopaedics (M5)
Faculty of Health Sciences University of the Free State
PO Box 339
Bloemfontein 9300
Tel: 0027 82 0853 019
Email: woutervangraan@gmail.com

